Untitled
The smear layer in endodontics – a review D. R. Violich1 & N. P. Chandler21Private Endodontic Practice, Tauranga, New Zealand; and 2Sir John Walsh Research Institute, School of Dentistry, University ofOtago, Dunedin, New Zealand texts, whilst older books revealed historic informationand primary research not found electronically, such Violich DR, Chandler NP. The smear layer in endodontics – that this paper does not represent a ‘classical' review.a review. International Endodontic Journal, 43, 2–15, 2010.
Data obtained suggests that smear layer removal Root canal instrumentation produces a layer of organic should enhance canal disinfection. Current methods and inorganic material called the smear layer that may of smear removal include chemical, ultrasonic and also contain bacteria and their by-products. It can laser techniques – none of which are totally effective prevent the penetration of intracanal medicaments into throughout the length of all canals or are universally dentinal tubules and influence the adaptation of filling accepted. If smear is to be removed, the method of materials to canal walls. This article provides an choice seems to be the alternate use of ethylenedi- overview of the smear layer, focusing on its relevance aminetetraacetic acid and sodium hypochlorite solu- to endodontics. The PubMed database was used tions. Conflict remains regarding the removal of the initially; the reference list for smear layer featured smear layer before filling root canals, with investiga- 1277 articles, and for both smear layer dentine and tions required to determine the role of the smear layer smear layer root canal revealed 1455 publications.
in the outcomes of root canal treatment.
Smear layer endodontics disclosed 408 papers. A Keywords: dentine, ethylenediaminetetraacetic acid, forward search was undertaken on selected articles endodontic treatment, smear layer.
and using some author names. Potentially relevantmaterial was also sought in contemporary endodontic Received 20 June 2007; accepted 21 July 2009 first reported by Eick et al. (1970). These workers showed that the smear layer was made of particles Whenever dentine is cut using hand or rotary ranging in size from less than 0.5–15 lm. Scanning instruments, the mineralized tissues are not shredded electron microscope studies of cavity preparations by or cleaved but shattered to produce considerable Bra¨nnstro¨m & Johnson (1974) demonstrated a thin quantities of debris. Much of this, made up of very layer of grinding debris. They estimated it to be small particles of mineralized collagen matrix, is 2–5 lm thick, extending a few micrometres into the spread over the surface to form what is called the dentinal tubules.
smear layer. Identification of the smear layer was The smear layer in a cavity and in the root canal made possible using the electron microprobe with may not be directly comparable. Not only are the tools scanning electron microscope (SEM) attachment, and for dentine preparation different in coronal cavities, butin the root canal the dentinal tubule numbers showgreater variation and there are likely to be more soft Correspondence: Nicholas Chandler, Associate Professor, tissue remnants present. The first researchers to School of Dentistry, University of Otago, P.O. Box 647, describe the smear layer on the surface of instrumented Dunedin 9054, New Zealand (Tel.: 0064 3 479 7124; fax:0064 3 479 5079; e-mail [email protected]).
root canals were McComb & Smith (1975). They International Endodontic Journal, 43, 2–15, 2010 ª 2010 International Endodontic Journal
Violich & Chandler Smear layer in endodontics
suggested that the smear layer consisted not only ofdentine as in the coronal smear layer, but also theremnants of odontoblastic processes, pulp tissue andbacteria. Lester & Boyde (1977) described the smearlayer as ‘organic matter trapped within translocatedinorganic dentine'. As it was not removed by sodiumhypochlorite irrigation, they concluded that it wasprimarily composed of inorganic dentine. Goldmanet al. (1981) estimated the smear thickness at 1 lmand agreed with previous investigators that it waslargely inorganic in composition. They noted its pres-ence along instrumented canal surfaces. Mader et al.
(1984) reported that the smear layer thickness wasgenerally 1–2 lm. Cameron (1983) and Mader et al.
(1984) discussed the smear material in two parts: first,
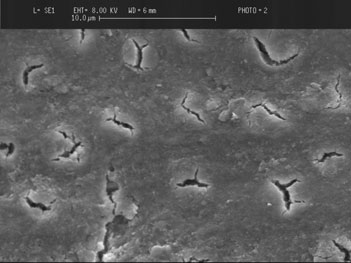
Figure 2 Scanning electron micrograph of dentine surface
superficial smear layer (Fig. 1) and second, the material
showing smear plugs occluding tubules. The surface has been
packed into the dentinal tubules. Packing of smear
treated for 60 s with Tubulicid Blue Label (Dental Therapeu-
debris was present in the tubules to a depth of 40 lm.
tics AB, Nacka, Sweden).
Bra¨nnstro¨m & Johnson (1974) and Mader et al. (1984)concluded that the tubular packing phenomenon wasdue to the action of burs and instruments. Components
surface-active reagents in the canal during endodontic
of the smear layer can be forced into the dentinal
instrumentation. The thickness may also depend on the
tubules to varying distances (Moodnik et al. 1976,
type and sharpness of the cutting instruments and
Bra¨nnstro¨m et al. 1980, Cengiz et al. 1990) to form
whether the dentine is dry or wet when cut (Barnes
smear plugs (Fig. 2). However, Cengiz et al. (1990)
1974, Gilboe et al. 1980, Cameron 1988). In the early
proposed that the penetration of smear material into
stages of instrumentation, the smear layer on the walls
dentinal tubules could also be caused by capillary
of canals can have a relatively high organic content
action as a result of adhesive forces between the
because of necrotic and/or viable pulp tissue in the root
dentinal tubules and the material. This hypothesis of
canal (Cameron 1988). Increased centrifugal forces
capillary action may explain the packing phenomenon
resulting from the movement and the proximity of the
observed by Aktener et al. (1989), who showed that the
instrument to the dentine wall formed a thicker layer
penetration could increase up to 110 lm when using
which was more resistant to removal with chelatingagents (Jodaikin & Austin 1981). The amount pro-duced during motorized preparation, as with Gates-Glidden or post drills, has been reported as greater involume than that produced by hand filing (Czonstkow-sky et al. 1990). However, McComb & Smith (1975)observed
K-reamers, K-files and Giromatic reciprocating filescreated similar surfaces. Additional work has shownthat the smear layer contains organic and inorganicsubstances that include fragments of odontoblasticprocesses, microorganisms and necrotic materials(Pashley 1992). The generation of a smear layer isalmost inevitable during root canal instrumentation.
Whilst a noninstrumentation technique has beendescribed for canal preparation without smear forma-tion, efforts rather focus on methods for its removal,
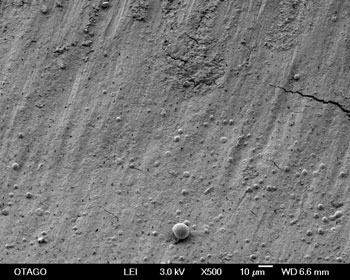
Figure 1 Scanning electron micrograph of smeared surface of
such as chemical means and methods such as ultra-
dentine. The crack shapes are processing artefacts overlying
sound and hydrodynamic disinfection for its disruption.
dentinal tubules.
Root canal preparation without the creation of a smear
ª 2010 International Endodontic Journal
International Endodontic Journal, 43, 2–15, 2010
Smear layer in endodontics Violich & Chandler
Vassiliadis et al. 1996, Taylor et al. 1997, Timpawat& Sripanaratanakul 1998, Economides et al. 1999,2004, von Fraunhofer et al. 2000, Froe´s et al. 2000,Goya et al. 2000, Timpawat et al. 2001, Clark-Holkeet al. 2003, Cobankara et al. 2004, Park et al. 2004).
Workers have reached different conclusions, with
current knowledge of interactions between the smearlayer and factors such as filling technique and sealertype being limited. In addition, the methodology ofstudies, the type and site of leakage tests, and thesample size should be taken into account and consid-eration given to these variables before conclusions arereached (Shahravan et al. 2007).
Some authors suggest that maintaining the smear
layer may block the dentinal tubules and limit bacterial
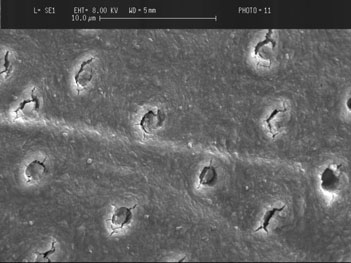
Figure 3 Scanning electron micrograph of dentine surface
or toxin penetration by altering dentinal permeability
with typical amorphous smear layer with granular appear-
(Michelich et al. 1980, Pashley et al. 1981, Safavi et al.
ance and moderate debris present (courtesy of Dr Artika
1990). Others believe that the smear layer, being a
loosely adherent structure, should be completelyremoved from the surface of the root canal wallbecause it can harbour bacteria and provide an avenue
layer may be possible. A noninstrumental hydrody-
for leakage (Mader et al. 1984, Cameron 1987a,
namic technique may have future potential (Lussi et al.
Meryon & Brook 1990). It may also limit the effective
1993), and sonically driven polymer instruments with
disinfection of dentinal tubules by preventing sodium
tips of variable diameter are reported to disrupt the
hypochlorite, calcium hydroxide and other intracanal
smear layer in a technique called hydrodynamic
medicaments from penetrating the dentinal tubules.
disinfection (Ruddle 2007).
When viewed under the SEM, the smear layer often
Should the smear layer be removed?
has an amorphous irregular and granular appearance(Bra¨nnstro¨m et al. 1980, Yamada et al. 1983, Pashley
The question of keeping or removing the smear layer
et al. 1988) (Fig. 3). The appearance is thought to be
remains controversial (Drake et al. 1994, Shahravan
formed by translocating and burnishing the superficial
et al. 2007). Some investigations have focussed on its
components of the dentine walls during treatment
removal (Garberoglio & Bra¨nnstro¨m 1976, Outhwaite
(Baumgartner & Mader 1987).
et al. 1976, Pashley 1985), whilst others have consid-ered its effects on apical and coronal microleakage(Madison & Krell 1984, Goldberg et al. 1995, Cha-
The significance of the smear layer
ilertvanitkul et al. 1996), bacterial penetration of the
Root canal treatment usually involves the chemome-
tubules (Pashley 1984, Williams & Goldman 1985,
chanical removal of bacteria and infected dentine from
Meryon & Brook 1990) and the adaptation of root
within the root canals. The process is often followed by
canal materials (White et al. 1987, Genc¸og˘lu et al.
an intracanal dressing and a root filling. Amongst
1993a, Gutmann 1993). In support of its removal are:
important factors affecting the prognosis of root canal
It has an unpredictable thickness and volume,
treatment is the seal created by the filling against the
because a great portion of it consists of water (Cerg-
walls of the canal. Considerable effort has been made to
neux et al. 1987).
understand the effect of the smear layer on the apical
2. It contains bacteria, their by-products and necrotic
and coronal seal (Madison & Krell 1984, Goldberg et al.
tissue (McComb & Smith 1975, Goldberg & Abramo-
1985, 1995, Evans & Simon 1986, Kennedy et al.
vich 1977, Wayman et al. 1979, Cunningham &
1986, Cergneux et al. 1987, Saunders & Saunders
Martin 1982, Yamada et al. 1983). Bacteria may
1992, 1994, Genc¸og˘lu et al. 1993a, Karago¨z-Ku
survive and multiply (Bra¨nnstro¨m & Nyborg 1973)
& Bayirli 1994, Tidswell et al. 1994, Lloyd et al. 1995,
and can proliferate into the dentinal tubules (Olgart
Behrend et al. 1996, Chailertvanitkul et al. 1996,
et al. 1974, Akpata & Blechman 1982, Williams &
International Endodontic Journal, 43, 2–15, 2010
ª 2010 International Endodontic Journal
Violich & Chandler Smear layer in endodontics
Goldman 1985, Meryon et al. 1986, Meryon & Brook
filling materials into dentinal tubules, whilst the basis
1990), which may serve as a reservoir of microbial
of leakage studies remains questionable. Pashley et al.
irritants (Pashley 1984).
(1989) observed an extensive network of microchan-
3. It may act as a substrate for bacteria, allowing their
nels around restorations that had been placed in
deeper penetration in the dentinal tubules (George et al.
cavities with smear layer. The thickness of these
channels was 1–10 lm. Smear layer may thus present
4. It may limit the optimum penetration of disinfecting
a passage for substances to leak around or through its
agents (McComb & Smith 1975, Outhwaite et al. 1976,
particles at the interface between the filling material
Goldberg & Abramovich 1977, Wayman et al. 1979,
and the tooth structure. Pashley & Depew (1986)
Yamada et al. 1983). Bacteria may be found deep
reported that, when experimenting with class 1 cavi-
within dentinal tubules (Bystro¨m & Sundqvist 1981,
ties, microleakage decreased after the removal of smear
1983, 1985) and smear layer may block the effects of
layer, but dentinal permeability increased. Saunders &
disinfectants in them (Goldberg & Abramovich 1977,
Saunders (1992) concluded that coronal leakage of
Wayman et al. 1979, Yamada et al. 1983, Baumgart-
root canal fillings was less in smear-free groups than
ner & Mader 1987). Haapasalo & Ørstavik (1987)
those with a smear layer.
found that in the absence of smear layer, liquid
6. It is a loosely adherent structure and a potential
camphorated monochlorophenol disinfected the den-
avenue for leakage and bacterial contaminant passage
tinal tubules rapidly and completely, but calcium
between the root canal filling and the dentinal walls
hydroxide failed to eliminate Enterococcus faecalis even
(Mader et al. 1984, Cameron 1987b, Meryon & Brook
after 7 days of incubation. A subsequent study con-
1990). Its removal would facilitate canal filling
cluded that the smear layer delayed but did not abolish
(McComb & Smith 1975, Goldman et al. 1981, Cam-
the action of the disinfectant (Ørstavik & Haapasalo
1990). Bra¨nnstro¨m (1984) had previously stated that
Conversely, some investigators believe in retaining
following the removal of the smear layer, bacteria in
the smear layer during canal preparation, because it
the dentinal tubules can easily be destroyed.
can block the dentinal tubules, preventing the ex-
5. It can act as a barrier between filling materials and
change of bacteria and other irritants by altering
the canal wall and therefore compromise the formation
permeability (Michelich et al. 1980, Pashley et al.
of a satisfactory seal (Lester & Boyde 1977, White et al.
1981, Safavi et al. 1990, Drake et al. 1994, Galvan
1984, Cergneux et al. 1987, Czonstkowsky et al. 1990,
et al. 1994). The smear layer serves as a barrier to
Foster et al. 1993, Yang & Bae 2002). Lester & Boyde
prevent bacterial migration into the dentinal tubules
(1977) found that zinc oxide – eugenol based root
(Drake et al. 1994, Galvan et al. 1994, Love et al.
canal sealers failed to enter dentinal tubules in the
1996, Perez et al. 1996). Pashley (1985) suggested
presence of smear. In two consecutive studies, White
that if the canals were inadequately disinfected, or if
et al. observed that plastic filling materials and sealers
bacterial contamination occurred after canal prepara-
penetrated dentinal tubules after removal of smear
tion, the presence of a smear layer might stop bacterial
layer (White et al. 1984, 1987). Oks¸an et al. (1993)
invasion of the dentinal tubules. Bacteria remaining
also found that smear prevented the penetration of
after canal preparation are sealed into the tubules by
sealers into dentinal tubules, whilst no penetration of
the smear layer and subsequent filling materials. Some
sealer was observed in control groups. Penetration in
studies provide evidence to support the hypothesis that
their smear-free groups ranged from 40 to 60 lm. It
the smear layer inhibits bacterial penetration (Pashley
may be concluded that such tubular penetration
et al. 1981, Safavi et al. 1989). A major limitation is
increases the interface between the filling and the
that the experiments were undertaken with dentine
dentinal structures, which may improve the ability of a
discs or root cross-sections, models with little relevance
filling material to prevent leakage (White et al. 1984).
in terms of simulating the clinical conditions of root
If the aim is maximum penetration into the dentinal
canal treatment. Drake et al. (1994) developed a more
tubules to prevent microleakage, root canal filling
clinically relevant model to determine the effect of the
materials should be applied to a surface free of smear
presence or absence of the smear layer on bacterial
and either a low surface activity or, alternatively, an
colonization of root canals.
adequate surface-active reagent must be added to them
Williams & Goldman (1985) reported that the smear
(Aktener et al. 1989). However, there are no reports of
layer was not a complete barrier and could only delay
a correlation between microleakage and penetration of
bacterial penetration. In their experiment, using the
ª 2010 International Endodontic Journal
International Endodontic Journal, 43, 2–15, 2010
Smear layer in endodontics Violich & Chandler
motile, swarming bacterium Proteus vulgaris, the smear
tubule penetration, increased sealer to dentine bond
layer delayed the passage of the organisms through the
strength and enhanced fluid-tight seal, a recent report
tubules. Madison & Krell (1984) using ethylenedi-
concluded that smear layer removal did not necessarily
aminetetraacetic acid (EDTA) solution in a dye pene-
equate to improved resistance to bacterial penetration
tration study found that the smear layer made no
along these and older types of sealers (Saleh et al.
difference to leakage. Goldberg et al. (1995) studied the
sealing ability of Ketac Endo and Tubliseal in an Indiaink study with and without smear layer and found no
Methods to remove the smear layer
difference. Chailertvanitkul et al. (1996) found nodifference in leakage with or without smear layer,
however the time period was short. When the smearlayer is not removed, the durability of the apical seal
The quantity of smear layer removed by a material is
should be evaluated over a long period. Since the smear
related to its pH and the time of exposure (Morgan &
layer is nonhomogenous and may potentially be
Baumgartner 1997). A number of chemicals have
dislodged from the underlying tubules (Mader et al.
been investigated as irrigants to remove the smear
1984), it may slowly disintegrate, dissolving around a
layer. According to Kaufman & Greenberg (1986), a
leaking filling material to leave a void between the
working solution is the one which is used to clean the
canal wall and sealer. Meryon & Brook (1990) found
canal, and an irrigation solution the one which is
the presence of smear layer had no effect on the ability
essential to remove the debris and smear layer created
of three oral bacteria to penetrate dentine discs. All
by the instrumentation process. Chlorhexidine, whilst
were able to digest the layer, possibly stimulated by the
popular as an irrigant and having a long lasting
nutrient-rich medium below the discs.
antibacterial effect through adherence to dentine, does
The adaptation of root canal materials to canal walls
not dissolve organic material or remove the smear
has been studied. White et al. (1987) found that
pHEMA, silicone and Roth 801 and AH26 sealersextended into tubules consistently when smear layer
Sodium hypochlorite
was removed. Genc¸og˘lu et al. (1993b) found removingthe smear layer enhanced the adaptation of gutta-
The ability of NaOCl to dissolve organic tissues is well-
percha in both cold laterally compacted and thermo-
known (Rubin et al. 1979, Wayman et al. 1979,
plastic root fillings without sealer. Gutmann (1993)
Goldman et al. 1982) and increases with rising tem-
also showed that after removing the smear layer,
perature (Moorer & Wesselink 1982). However, its
themoplastic gutta-percha adapted with or without
capacity to remove smear layer from the instrumented
root canal walls has been found to be lacking. The
A systematic review and meta-analysis by Shahra-
conclusion reached by many authors is that the use of
van et al. (2007) set out to determine whether smear
NaOCl during or after instrumentation produces super-
layer removal reduced leakage of root filled teeth ex
ficially clean canal walls with the smear layer present
vivo. Using 26 eligible papers with 65 comparisons,
(Baker et al. 1975, Goldman et al. 1981, Berg et al.
54% of the comparisons reported no significant differ-
1986, Baumgartner & Mader 1987).
ence, 41% reported in favour of removing the smearlayer and 5% reported a difference in favour of keeping
it. They concluded that smear layer removal improvedthe fluid-tight seal of the root canal system, whereas
Smear layer components include very small particles
other factors such as filling technique or the type of
with a large surface : mass ratio, which makes them
sealer did not produce significant effects.
soluble in acids (Pashley 1992). The most common
Urethane dimethacrylate (UDMA) based root canal
chelating solutions are based on EDTA which reacts
sealers have been introduced. Their aim is to provide a
with the calcium ions in dentine and forms soluble
better bond to allow less microleakage and increase the
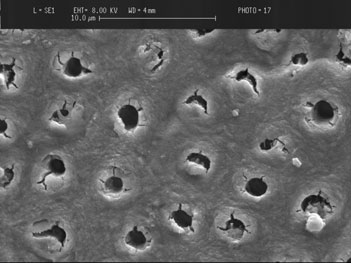
calcium chelates (Fig. 4). It has been reported that
fracture resistance of root filled teeth through the
EDTA decalcified dentine to a depth of 20–30 lm in
creation of monoblocks, when a core material such as
5 min (von der Fehr & Nygaard-O
¨ stby 1963); however,
Resilon replaces gutta-percha. Whilst some studies
Fraser (1974) stated that the chelating effect was
indicate that smear layer removal leads to higher
almost negligible in the apical third of root canals.
International Endodontic Journal, 43, 2–15, 2010
ª 2010 International Endodontic Journal
Violich & Chandler Smear layer in endodontics
of EDTAC (EDTA and cetavlon). The optimal workingtime of EDTAC was suggested to be 15 min in the rootcanal and no further chelating action could be expectedafter this (Goldberg & Spielberg 1982). This study alsoshowed that REDTA was the most efficient irrigatingsolution for removing smear layer. In a study using acombination of 0.2% EDTA and a surface-activeantibacterial solution, Bra¨nnstro¨m et al. (1980) ob-served that this mixture removed most of the smearlayer without opening many dentinal tubules orremoving peritubular dentine. Bis-dequalinium-acetate(BDA), a dequalinium compound and an oxine deriv-ative has been shown to remove the smear layerthroughout the canal, even in the apical third (Kauf-man et al. 1978, Kaufman 1981). BDA is well tolerated
Figure 4 Scanning electron micrograph of dentine following
60 s exposure to 18% ethylenediaminetetraacetic acid solu-
by periodontal tissues and has a low surface tension
tion (Ultradent Products Inc., South Jordan, UT, USA).
allowing good penetration. It is considered less toxicthat NaOCl and can be used as a root canal dressing. Acommercial form of BDA called Solvidont (De Trey,
Different formulations of EDTA have been used as
A.G., Zurich, Switzerland) was available in the 1980s
root canal irrigants. In a combination, urea peroxide is
and its use as an alternative to NaOCl was supported
added to encourage debris to float out of the root canal
experimentally (Kaufman 1983a,b, Chandler & Lilley
(Stewart et al. 1969). This product (RC-Prep, Premier
1987, Lilley et al. 1988, Mohd Sulong 1989). Salvizol
Dental Products, Plymouth Meeting, PA, USA) also
(Ravens Gmbh, Konstanz, Germany) is a commercial
includes a wax that left a residue on the root canal
brand of 0.5% BDA and possesses the combined actions
walls despite further instrumentation and irrigation
of chelation and organic debridement. Kaufman et al.
and which may compromise the ability to obtain a
(1978) reported that Salvizol had better cleaning
hermetic seal (Biesterfeld & Taintor 1980). Many
properties than EDTAC. When comparing Salvizol with
studies have shown that paste-type chelating agents,
5.25% NaOCl, both were found comparable in their
whilst having a lubricating effect, do not remove the
ability to remove organic debris, but only Salvizol
smear layer effectively when compared to liquid EDTA.
opened dentinal tubules (Kaufman & Greenberg 1986).
A recent experiment examining the addition of two
Berg et al. (1986) found that Salvizol was less effective
surfactants to liquid EDTA did not result in better smear
at opening dentinal tubules than REDTA.
layer removal (Lui et al. 2007).
¸ alt & Serper (2000) compared the effects of ethylene
A quaternary ammonium bromide (cetrimide) has
glycol-bis (ß-aminoethyl ether)-N,N,N¢, N¢-tetraacetic
been added to EDTA solutions to reduce surface tension
acid (EGTA) with EDTA. The smear layer was com-
and increase penetrability of the solution (von der Fehr
pletely removed by EDTA, but it caused erosion of the
¨ stby 1963). McComb & Smith (1975)
peritubular and intertubular dentine, whilst EGTA was
reported that when this combination (REDTA) was
not as effective in the apical third of root canals. EGTA
used during instrumentation, there was no smear layer
is reported to bind calcium more specifically (Schmid &
remaining except in the apical part of the canal. After
Reilley 1957).
using REDTA in vivo, it was shown that the root canal
Tetracylines (including tetracycline hydrochloride,
surfaces were uniformly occupied by patent dentinal
minocycline and doxycycline) are antibiotics effective
tubules with very little superficial debris (McComb et al.
against a wide range of microorganisms. Tetracyclines
1976). When used during and after instrumentation, it
have unique properties in addition to their antimicro-
was possible to still see remnants of odontoblastic
bial aspect. They have low pH in concentrated solution,
processes within the tubules even though there was no
and because of this can act as a calcium chelator and
smear layer present (Goldman et al. 1981). Goldberg &
cause enamel and root surface demineralization (Bjor-
Abramovich (1977) observed that the circumpulpal
vatn 1982). The surface demineralization of dentine is
surface had a smooth structure and that the dentinal
comparable with that of citric acid (Wikesjo¨ et al.
tubules had a regular circular appearance with the use
1986). Barkhordar et al. (1997) reported that doxycy-
ª 2010 International Endodontic Journal
International Endodontic Journal, 43, 2–15, 2010
Smear layer in endodontics Violich & Chandler
cline hydrochloride (100 mg mL-1) was effective in
(1989) introduced 25% tannic acid solution as a root
removing the smear layer from the surface of instru-
canal irrigant and cleanser. Canal walls irrigated with
mented canals and root-end cavity preparations. They
speculated that a reservoir of active antibacterial agents
smoother than walls treated with a combination of
might remain, because doxycycline readily attaches to
hydrogen peroxide and NaOCl, and the smear layer was
dentine and can be subsequently released (Baker et al.
removed. Sabbak & Hassanin (1998) refuted these
1983, Wikesjo¨ et al. 1986). Haznedaroglu & Ersev
findings and explained that tannic acid increased the
(2001) showed that 1% tetracycline hydrochloride or
cross-linking of exposed collagen with the smear layer
50% citric acid can be used to remove the smear layer
and within the matrix of the underlying dentine,
from surfaces of root canals. Although they reported no
therefore increasing organic cohesion to the tubules.
difference between the two groups, it appeared that the
McComb & Smith (1975) compared the efficacy of
tetracycline demineralized less peritubular dentine than
20% polyacrylic acid with REDTA and found that it
the citric acid.
was no better than REDTA in removing or preventing
In an effort to produce an irrigant capable of both
the build up of smear layer, thought to be as a result of
removing the smear layer and disinfecting the root
its higher viscosity. McComb et al. (1976) also used 5%
canal system, Torabinejad et al. (2003) developed a
and 10% polyacrylic acid as an irrigant and observed
new irrigating solution containing a mixture of a
that it could remove smear layer in accessible regions.
tetracycline isomer, an acid, and a detergent (MTAD).
Polyacrylic acid (Durelon liquid and Fuji II liquid) at
Their work concluded MTAD to be an effective solution
40% has been reported to be very effective, and because
for the removal of the smear layer. It does not
of its potency users should not exceed a 30 s applica-
significantly change the structure of the dentinal
tion (Berry et al. 1987).
tubules when the canals are irrigated with sodiumhypochlorite and followed with a final rinse of MTAD.
Sodium hypochlorite and EDTA
This irrigant demineralizes dentine faster than 17%EDTA (De-Deus et al. 2007) and bacterial penetration
When irrigating a root canal the purpose is twofold: to
into filled canals is similar with both solutions (Ghod-
remove the organic component, the debris originating
dusi et al. 2007).
from pulp tissue and microorganisms, and the mostlyinorganic component, the smear layer. As there is nosingle solution which has the ability to dissolve organic
tissues and to demineralize the smear layer, the
The effectiveness of citric acid as a root canal irrigant
sequential use of organic and inorganic solvents has
has been demonstrated (Loel 1975, Tidmarsh 1978)
been recommended (Koskinen et al. 1980, Yamada
and confirmed to be more effective than NaOCl alone in
et al. 1983, Baumgartner et al. 1984). Numerous
removing the smear layer (Baumgartner et al. 1984).
authors have agreed that the removal of smear layer
Citric acid removed smear layer better than polyacrylic
as well as soft tissue and debris can be achieved by the
acid, lactic acid and phosphoric acid but not EDTA
alternate use of EDTA and NaOCl (Yamada et al. 1983,
(Meryon et al. 1987). Wayman et al. (1979) showed
White et al. 1984, Baumgartner & Mader 1987, Cengiz
that canal walls treated with 10%, 25% and 50% citric
et al. 1990). Goldman et al. (1982) examined the effect
acid solution were generally free of the smeared
of various combinations of EDTA and NaOCl, and the
appearance, but they had the best results in removing
most effective final rinse was 10 mL of 17% EDTA
smear layer with sequential use of 10% citric acid
followed by 10 mL of 5.25% NaOCl, a finding con-
solution and 2.5% NaOCl solution, then again followed
firmed by Yamada et al. (1983). Used in combination
by a 10% solution of citric acid. However, Yamada
with EDTA, NaOCl is inactivated with the EDTA
et al. (1983) observed that the 25% citric acid–NaOCl
remaining functional for several minutes.
group was not as effective as a 17% EDTA–NaOClcombination. To its detriment, citric acid left precipi-
Ultrasonic smear removal
tated crystals in the root canal which might bedisadvantageous to the root canal filling. With 50%
Following the introduction of dental ultrasonic devices
lactic acid, the canal walls were generally clean, but
in the 1950s, ultrasound was investigated in end-
with openings of dentinal tubules that did not appear to
odontics (Martin et al. 1980, Cunningham & Martin
be completely patent (Wayman et al. 1979). Bitter
1982, Cunningham et al. 1982). A continuous flow of
International Endodontic Journal, 43, 2–15, 2010
ª 2010 International Endodontic Journal
Violich & Chandler Smear layer in endodontics
NaOCl activated by an ultrasonic delivery system was
or 1% sodium hypochlorite to achieve the desired
used for the preparation and irrigation of canals.
Smear-free canal surfaces were observed using thismethod (Cameron 1983, 1987a,b, Griffiths & Stock
1986, Alac¸am 1987). Whilst concentrations of 2–4%sodium hypochlorite in combination with ultrasonic
Lasers can be used to vaporize tissues in the main
energy were able to remove smear layer, lower
canal, remove the smear layer and eliminate residual
concentrations of the solutions were unsatisfactory
tissue in the apical portion of root canals (Takeda et al.
(Cameron 1988). However, Ahmad et al. (1987a)
1998a,b, 1999). The effectiveness of lasers depends on
claimed that their technique of modified ultrasonic
many factors, including the power level, the duration of
instrumentation using 1% NaOCl removed the debris
exposure, the absorption of light in the tissues, the
and smear layer more effectively than the technique
geometry of the root canal and the tip-to-target
recommended by Martin & Cunningham (1983). The
distance (Dederich et al. 1984, O
¨ nal et al. 1993, Tewfik
apical region of the canals showed less debris and
et al. 1993, Moshonov et al. 1995).
smear layer than the coronal aspects, depending on
Dederich et al. (1984) and Tewfik et al. (1993) used
acoustic streaming, which was more intense in
variants of the neodymium–yttrium-aluminium-gar-
magnitude and velocity at the apical regions of the
net (Ne:YAG) laser and reported a range of findings
file. Cameron (1983) also compared the effect of
from no change or disruption of the smear layer to
different ultrasonic irrigation periods on removing
actual melting and recrystallization of the dentine.
smear layer and found that a 3- and 5-min irrigation
This pattern of dentine disruption was observed in
produced smear-free canal walls, whilst an 1-min
other studies with various lasers, including the carbon
irrigation was ineffective. In contrast to these results,
¨ nal et al. 1993), the argon fluoride
other investigators found ultrasonic preparation un-
excimer laser (Stabholz et al. 1993), and the argon
able to remove smear layer (Cymerman et al. 1983,
laser (Moshonov et al. 1995, Harashima et al. 1998).
Baker et al. 1988, Goldberg et al. 1988).
Takeda et al. (1998a,b, 1999) using the erbium-
Researchers who found the cleaning effects of
ultrasonics beneficial used the technique only for the
strated optimal removal of the smear layer without
final irrigation of root canal after completion of hand
melting, charring or recrystallization associated with
instrumentation (Ahmad et al. 1987a, Alac¸am 1987,
other laser types. Kimura et al. (2002) also demon-
Cameron 1988). This is given the term passive ultra-
strated the removal of the smear layer with an Er:YAG
sonic irrigation and has been the subject of a recent
laser. Although they showed removal of the smear
review (van der Sluis et al. 2007). Ahmad et al.
layer, photomicrographs showed destruction of peri-
(1987a,b) claimed that direct physical contact of the
file with the canal walls throughout instrumentation
removal of the smear layer is access to the small
reduced acoustic streaming. Acoustic streaming is
canal spaces with the relatively large probes that are
maximized when the tips of the smaller instruments
vibrate freely in a solution. Lumley et al. (1992)recommended that only size 15 files be used to
maximize microstreaming for the removal of debris.
Prati et al. (1994) also achieved smear layer removal
Contemporary methods of root canal instrumentation
with ultrasonics. Walker & del Rio (1989, 1991)
produce a layer of organic and inorganic material called
showed no significant difference between tap water and
the smear layer that may also contain bacteria and their
sodium hypochlorite when used with ultrasonics, but
by-products. This layer covers the instrumented walls
they reported that neither solution was effective at any
and may prevent the penetration of intracanal medica-
level in the canal to remove the smear layer ultrason-
ments into the dentinal tubules and interfere with the
ically. Baumgartner & Cuenin (1992) also observed
close adaptation of root filling materials to canal walls.
that ultrasonically energized NaOCl, even at full
The data presented indicate removal of the smear layer
strength, did not remove the smear layer from root
for more thorough disinfection of the root canal system
canal walls. Guerisoli et al. (2002) evaluated the use of
and better adaptation of materials to the canal walls.
ultrasonics to remove the smear layer and found it
There are, however, no clinical trials to demonstrate
necessary to use 15% EDTAC with either distilled water
this. Current methods of smear layer removal include
ª 2010 International Endodontic Journal
International Endodontic Journal, 43, 2–15, 2010
Smear layer in endodontics Violich & Chandler
chemical, ultrasonic and laser techniques – none of
Baumgartner JC, Mader CL (1987) A scanning electron
which are totally effective throughout the length of all
microscopic evaluation of four root canal irrigation regi-
canals or are used universally. However, if the smear
mens. Journal of Endodontics 13, 147–57.
layer is to be removed the method of choice seems to be
Baumgartner JC, Brown CM, Mader CL, Peters DD, Shulman
JD (1984) A scanning electron microscopic evaluation of
the alternate use of EDTA and sodium hypochlorite
root canal debridement using saline, sodium hypochlorite,
solutions. Whilst much is known about individual
and citric acid. Journal of Endodontics 10, 525–31.
irrigants, their use in combination and their interac-
Behrend GD, Cutler CW, Gutmann JL (1996) An in-vitro
tions (and in some cases precipitates) is less well
study of smear layer removal and microbial leakage along
understood. Conflicting reports exist regarding the
root-canal fillings. International Endodontic Journal 29, 99–
removal of the smear layer before filling root canals.
As several new sealer and core materials have recently
Berg MS, Jacobsen EL, BeGole EA, Remeikis NA (1986) A
been introduced, further investigations are required to
comparison of five irrigating solutions: a scanning electron
determine the role of the smear layer in the outcome of
microscopic study. Journal of Endodontics 12, 192–7.
Berry EA III, von der Lehr WN, Herrin HK (1987) Dentin
surface treatments for the removal of the smear layer: an
SEM study. Journal of the American Dental Association 115,
Biesterfeld RC, Taintor JF (1980) A comparison of periapical
Ahmad M, Pitt Ford TR, Crum LA (1987a) Ultrasonic
seals of root canals with RC-Prep or Salvizol. Oral Surgery,
debridement of root canals: acoustic streaming and its
Oral Medicine and Oral Pathology 49, 532–7.
possible role. Journal of Endodontics 13, 490–9.
Bitter NC (1989) A 25% tannic acid solution as a root canal
Ahmad M, Pitt Ford TR, Crum LA (1987b) Ultrasonic
irrigant cleanser: a scanning electron microscope study.
debridement of root canals: an insight into the mechanisms
Oral Surgery, Oral Medicine and Oral Pathology 67, 333–7.
involved. Journal of Endodontics 13, 93–101.
Bjorvatn K (1982) Antibiotic compounds and enamel demin-
Akpata ES, Blechman H (1982) Bacterial invasion of pulpal
eralization. An in vitro study. Acta Odontologica Scandinavica
dentin wall in vitro. Journal of Dental Research 61, 435–8.
40, 341–52.
Aktener BO, Cengiz T, Piskin B (1989) The penetration of
Bra¨nnstro¨m M (1984) Communication between the oral
smear material into dentinal tubules during instrumenta-
cavity and the dental pulp associated with restorative
tion with surface-active reagents: a scanning electron
treatment. Operative Dentistry 9, 57–68.
microscopic study. Journal of Endodontics 15, 588–90.
Bra¨nnstro¨m M, Johnson G (1974) Effects of various condi-
Alac¸am T (1987) Scanning electron microscope study com-
tioners and cleaning agents on prepared dentin surfaces: a
paring the efficacy of endodontic irrigating systems. Inter-
scanning electron microscopic investigation. Journal of
national Endodontic Journal 20, 287–94.
Prosthetic Dentistry 31, 422–30.
Baker NA, Eleazer PD, Averbach RE, Seltzer S (1975)
Bra¨nnstro¨m M, Nyborg H (1973) Cavity treatment with a
Scanning electron microscopic study of the efficacy of
microbicidal fluoride solution: growth of bacteria and effect
various irrigating solutions. Journal of Endodontics 1, 127–
on the pulp. Journal of Prosthetic Dentistry 30, 303–10.
Bra¨nnstro¨m M, Nordenvall KJ, Glantz P-O (1980) The effect of
Baker PJ, Evans RT, Coburn RA, Genco RJ (1983) Tetracycline
EDTA-containing surface-active solutions on the morphol-
and its derivatives strongly bind to and are released from the
ogy of prepared dentin: an in vivo study. Journal of Dental
tooth surface in active form. Journal of Periodontology 54,
Research 59, 1127–31.
Bystro¨m A, Sundqvist G (1981) Bacteriologic evaluation of the
Baker MC, Ashrafi SH, Van Cura JE, Remeikis NA (1988)
efficacy of mechanical root canal instrumentation in end-
Ultrasonic compared with hand instrumentation: a scan-
odontic therapy. Scandinavian Journal of Dental Research 89,
ning electron microscope study. Journal of Endodontics 14,
Bystro¨m A, Sundqvist G (1983) Bacteriologic evaluation of the
Barkhordar RA, Watanabe LG, Marshall GW, Hussain MZ
effect of 0.5 percent sodium hypochlorite in endodontic
(1997) Removal of intracanal smear by doxycycline in vitro.
therapy. Oral Surgery, Oral Medicine and Oral Pathology 55,
Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology
and Endodontics 84, 420–3.
Bystro¨m A, Sundqvist G (1985) The antibacterial action of
Barnes IE (1974) The production of inlay cavity bevels. British
sodium hypochlorite and EDTA in 60 cases of endodontic
Dental Journal 137, 379–90.
therapy. International Endodontic Journal 18, 35–40.
Baumgartner JC, Cuenin PR (1992) Efficacy of several
¸ alt S, Serper A (2000) Smear layer removal by EGTA. Journal
concentrations of sodium hypochlorite for root canal
of Endodontics 26, 459–61.
irrigation. Journal of Endodontics 18, 605–12.
International Endodontic Journal, 43, 2–15, 2010
ª 2010 International Endodontic Journal
Violich & Chandler Smear layer in endodontics
Cameron JA (1983) The use of ultrasonics in the removal of
longitudinal and quantitative assessment. Journal of End-
the smear layer: a scanning electron microscope study.
odontics 33, 1364–1368.
Journal of Endodontics 9, 289–92.
Drake DR, Wiemann AH, Rivera EM, Walton RE (1994)
Cameron JA (1987a) The synergistic relationship between
Bacterial retention in canal walls in vitro: effect of smear
ultrasound and sodium hypochlorite: a scanning electron
layer. Journal of Endodontics 20, 78–82.
microscope evaluation. Journal of Endodontics 13, 541–5.
Economides N, Liolios E, Kolokuris I, Beltes P (1999) Long-
Cameron JA (1987b) The use of 4 per cent sodium hypochlo-
term evaluation of the influence of smear layer removal on
rite, with or without ultrasound, in cleansing of uninstru-
the sealing ability of different sealers. Journal of Endodontics
mented immature root canals; SEM study. Australian Dental
25, 123–5.
Journal 32, 204–13.
Economides N, Kokorikos I, Kolokouris I, Panagiotis B, Gogos
Cameron JA (1988) The use of ultrasound for the removal of
C (2004) Comparative study of apical sealing ability of a
the smear layer. The effect of sodium hypochlorite concen-
new resin-based root canal sealer. Journal of Endodontics 30,
tration; SEM study. Australian Dental Journal 33, 193–200.
Cengiz T, Aktener BO, Piskin B (1990) Effect of dentinal tubule
Eick JD, Wilko RA, Anderson CH, Sorensen SE (1970)
orientation on the removal of smear layer by root canal
Scanning electron microscopy of cut tooth surfaces and
irrigants. A scanning electron microscopic study. Interna-
identification of debris by use of the electron microprobe.
tional Endodontic Journal 23, 163–71.
Journal of Dental Research 49(Suppl), 1359–68.
Cergneux M, Ciucchi B, Dietschi JM, Holz J (1987) The
Evans JT, Simon JHS (1986) Evaluation of the apical seal
influence of the smear layer on the sealing ability of canal
produced by injected thermoplasticized gutta-percha in the
obturation. International Endodontic Journal 20, 228–32.
absence of smear layer and root canal sealer. Journal of
Chailertvanitkul P, Saunders WP, MacKenzie D (1996) The
Endodontics 12, 100–7.
effect of smear layer on microbial coronal leakage of gutta-
von der Fehr FR, Nygaard-O
¨ stby B (1963) Effect of EDTAC and
percha root fillings. International Endodontic Journal 29,
sulfuric acid on root canal dentine. Oral Surgery, Oral
Medicine and Oral Pathology 16, 199–205.
Chandler NP, Lilley JD (1987) Clinical trial of a bis-dequalin-
Foster KH, Kulild JC, Weller RN (1993) Effect of smear
ium-acetate solution as an endodontic irrigant. Journal of
layer removal on the diffusion of calcium hydroxide
Dental Research 66, 842.
through radicular dentin. Journal of Endodontics 19, 136–
Clark-Holke D, Drake D, Walton R, Rivera E, Guthmiller JM
(2003) Bacterial penetration through canals of endodonti-
Fraser JG (1974) Chelating agents: their softening effect on
cally treated teeth in the presence or absence of the smear
root canal dentin. Oral Surgery, Oral Medicine and Oral
layer. Journal of Dentistry 31, 275–81.
Pathology 37, 803–11.
Cobankara FK, Adanir N, Belli S (2004) Evaluation of the
von Fraunhofer JA, Fagundes DK, McDonald NJ, Dumsha TC
influence of smear layer on the apical and coronal sealing
(2000) The effect of root canal preparation on microleakage
ability of two sealers. Journal of Endodontics 30, 406–9.
within endodontically treated teeth: an in vitro study.
Cunningham WT, Martin H (1982) A scanning electron
International Endodontic Journal 33, 355–60.
microscope evaluation of root canal de´bridement with the
Froe´s JA, Horta HGP, da Silveira AB (2000) Smear layer
endosonic ultrasonic synergistic system. Oral Surgery, Oral
influence on the apical seal of four different obturation
Medicine and Oral Pathology 53, 527–31.
techniques. Journal of Endodontics 26, 351–4.
Cunningham WT, Martin H, Forrest WR (1982) Evaluation of
Galvan DA, Ciarlone AE, Pashley DH, Kulild JC, Primack PD,
root canal de´bridement by the endosonic ultrasonic syner-
Simpson MD (1994) Effect of smear layer removal on the
gistic system. Oral Surgery, Oral Medicine and Oral Pathology
diffusion permeability of human roots. Journal of Endodontics
53, 401–4.
Cymerman JJ, Jerome LA, Moodnik RM (1983) A scanning
Garberoglio R, Bra¨nnstro¨m M (1976) Scanning electron
electron microscope study comparing the efficacy of hand
microscopic investigation of human dentinal tubules.
instrumentation with ultrasonic instrumentation of the root
Archives of Oral Biology 21, 355–62.
canal. Journal of Endodontics 9, 327–31.
Genc¸og˘lu N, Samani S, Gu
¨ nday M (1993a) Dentinal wall
Czonstkowsky M, Wilson EG, Holstein FA (1990) The smear
adaptation of thermoplasticized gutta-percha in the absence
layer in endodontics. Dental Clinics of North America 34, 13–
or presence of smear layer: a scanning electron microscopic
study. Journal of Endodontics 19, 558–62.
Dederich DN, Zakariasen KL, Tulip J (1984) Scanning electron
Genc¸og˘lu N, Samani S, Gu
¨ nday M (1993b) Evaluation of
microscopic analysis of canal wall dentin following neo-
sealing properties of Thermafil and Ultrafil techniques in the
dymium-yttrium-aluminum-garnet laser irradiation. Journal
absence or presence of smear layer. Journal of Endodontics
of Endodontics 10, 428–31.
19, 599–603.
De-Deus G, Reis C, Fidel S, Fidel R, Paciornik S (2007) Dentin
George S, Kishen A, Song KP (2005) The role of environmen-
demineralization when subjected to BioPure MTAD: a
tal changes on monospecies biofilm formation on root canal
ª 2010 International Endodontic Journal
International Endodontic Journal, 43, 2–15, 2010
Smear layer in endodontics Violich & Chandler
wall by Enterococcus faecalis. Journal of Endodontics 31, 867–
Haznedaroglu F, Ersev H (2001) Tetracycline HCl solution
as a root canal irrigant. Journal of Endodontics 27, 738–
Ghoddusi J, Rohani A, Rashed T, Ghaziani P, Akbari M (2007)
An evaluation of microbial leakage after using MTAD as a
Jodaikin A, Austin JC (1981) Smear layer removal with
final irrigation. Journal of Endodontics 33, 173–176.
chelating agents after cavity preparation. Journal of Pros-
Gilboe DB, Svare CW, Thayer KE, Drennon DG (1980)
thetic Dentistry 46, 171–4.
Dentinal smearing: an investigation of the phenomenon.
¨ kay I, Bayirli G (1994) An apical leakage study
Journal of Prosthetic Dentistry 44, 310–6.
in the presence and absence of the smear layer. International
Goldberg F, Abramovich A (1977) Analysis of the effect of
Endodontic Journal 27, 87–93.
EDTAC on the dentinal walls of the root canal. Journal of
Kaufman AY (1981) The use of dequalinium acetate as a
Endodontics 3, 101–5.
disinfectant and chemotherapeutic agent in endodontics.
Goldberg F, Spielberg C (1982) The effect of EDTAC and the
Oral Surgery, Oral Medicine and Oral Pathology 51, 434–
variation of its working time analyzed with scanning
electron microscopy. Oral Surgery, Oral Medicine and Oral
Kaufman AY (1983a) Solvidont – a new chemotherapeutic
Pathology 53, 74–7.
and bacteriocidal agent for endodontic use (I). Quintessence
Goldberg F, Bernat MI, Spielberg C, Massone EJ, Piovano SA
International 14, 71–9.
(1985) Analysis of the effect of ethylenediaminetetraacetic
Kaufman AY (1983b) Solvidont – a new chemotherapeutic
acid on the apical seal of root canal fillings. Journal of
and bacteriocidal agent for endodontic use (II). Quintessence
Endodontics 11, 544–7.
International 14, 235–44.
Goldberg F, Soares I, Massone EJ, Soares IM (1988) Compar-
Kaufman AY, Greenberg I (1986) Comparative study of the
ative debridement study between hand and sonic instru-
configuration and the cleanliness level of root canals
mentation of the root canal. Endodontics and Dental
prepared with the aid of sodium hypochlorite and bis-
Traumatology 4, 229–34.
dequalinium-acetate solutions. Oral Surgery, Oral Medicine
Goldberg F, Artaza LP, De Silvio A (1995) Apical sealing
and Oral Pathology 62, 191–7.
ability of a new glass ionomer root canal sealer. Journal of
Kaufman AY, Binderman I, Tal M, Gedalia I, Peretz G (1978)
Endodontics 21, 498–500.
New chemotherapeutic agent for root canal treatment. A
Goldman LB, Goldman M, Kronman JH, Lin PS (1981) The
preliminary electron microscopic study on an in vivo and in
efficacy of several irrigating solutions for endodontics: a
vitro endodontically treated tooth. Oral Surgery, Oral Med-
scanning electron microscopic study. Oral Surgery, Oral
icine and Oral Pathology 46, 283–95.
Medicine and Oral Pathology 52, 197–204.
Kennedy WA, Walker WA III, Gough RW (1986) Smear layer
Goldman M, Goldman LB, Cavaleri R, Bogis J, Lin PS (1982)
removal effects on apical leakage. Journal of Endodontics 12,
The efficacy of several endodontic irrigating solutions: a
scanning electron microscopic study: Part 2. Journal of
Kimura Y, Yonaga K, Yokoyama K, Kinoshita J, Ogata Y,
Endodontics 8, 487–92.
Matsumoto K (2002) Root surface temperature increase
Goya C, Yamazaki R, Tomita Y, Kimura Y, Matsumoto K
during Er:YAG laser irradiation of root canals. Journal of
(2000) Effects of pulsed Nd:YAG laser irradiation on smear
Endodontics 28, 76–8.
layer at the apical stop and apical leakage after obturation.
Koskinen KP, Meurman JH, Stenvall H (1980) Appearance of
International Endodontic Journal 33, 266–71.
chemically treated root canal walls in the scanning electron
Griffiths BM, Stock CJR (1986) The efficiency of irrigants in
microscope. Scandinavian Journal of Dental Research 88, 397–
removing root canal debris when used with ultrasonic
preparation technique. International Endodontic Journal 19,
Lester KS, Boyde A (1977) Scanning electron microscopy of
instrumented, irrigated and filled root canals. British Dental
Guerisoli DMZ, Marchesan MA, Walmsley AD, Lumley PJ,
Journal 143, 359–67.
Pecora JD (2002) Evaluation of smear layer removal by
Lilley JD, Russell C, Chandler NP (1988) Comparison of bis-
EDTAC and sodium hypochlorite with ultrasonic agitation.
dequalinium-acetate and sodium hypochlorite solutions as
International Endodontic Journal 35, 418–21.
endodontic irrigants. Journal of Dental Research 67, 300.
Gutmann JL (1993) Adaptation of injected thermoplasticized
Lloyd A, Thompson J, Gutmann JL, Dummer PMH (1995)
gutta-percha in the absence of the dentinal smear layer.
Sealability of the Trifecta technique in the presence or
International Endodontic Journal 26, 87–92.
absence of a smear layer. International Endodontic Journal 28,
Haapasalo M, Ørstavik D (1987) In vitro infection and
disinfection of dentinal tubules. Journal of Dental Research
Loel DA (1975) Use of acid cleanser in endodontic therapy.
66, 1375–9.
Journal of the American Dental Association 90, 148–51.
Harashima T, Takeda FH, Zhang C, Kimura Y, Matsumoto K
Love RM, Chandler NP, Jenkinson HF (1996) Penetration of
(1998) Effect of argon laser irradiation on instrumented root
smeared or nonsmeared dentine by Streptococcus gordonii.
canal walls. Endodontics and Dental Traumatology 14, 26–30.
International Endodontic Journal 29, 2–12.
International Endodontic Journal, 43, 2–15, 2010
ª 2010 International Endodontic Journal
Violich & Chandler Smear layer in endodontics
Lui J-N, Kuah H-G, Chen N-N (2007) Effects of EDTA with and
Morgan LA, Baumgartner JC (1997) Demineralization of
without surfactants or ultrasonics on removal of smear
resected root-ends with methylene blue dye. Oral Surgery,
layer. Journal of Endodontics 33, 472–5.
Oral Medicine, Oral Pathology, Oral Radiology and Endodontics
Lumley PJ, Walmsley AD, Walton RE, Rippin JW (1992) Effect
of precurving endosonic files on the amount of debris and
Moshonov J, Sion A, Kasirer J, Rotstein I, Stabholz A (1995)
smear layer remaining in curved root canals. Journal of
Efficacy of argon laser irradiation in removing intracanal
Endodontics 18, 616–9.
debris. Oral Surgery, Oral Medicine, Oral Pathology, Oral
Lussi A, Nussba¨cher U, Grosrey J (1993) A novel noninstru-
Radiology and Endodontics 79, 221–5.
mented technique for cleansing the root canal system.
Oks¸an T, Aktener BO, S¸en BH, Tezel H (1993) The penetration
Journal of Endodontics 19, 549–53.
of root canal sealers into dentinal tubules. A scanning
Mader CL, Baumgartner JC, Peters DD (1984) Scanning
electron microscopic study. International Endodontic Journal
electron microscopic investigation of the smeared layer on
26, 301–5.
root canal walls. Journal of Endodontics 10, 477–83.
Olgart L, Bra¨nnstro¨m M, Johnson G (1974) Invasion of
Madison S, Krell KV (1984) Comparison of ethylenediamine
bacteria into dentinal tubules. Experiments in vivo and in
tetraacetic acid and sodium hypochlorite on the apical seal
vitro. Acta Odontologica Scandinavica 32, 61–70.
of endodontically treated teeth. Journal of Endodontics 10,
¨ nal B, Ertl T, Siebert G, Mu¨ller G (1993) Preliminary report
on the application of pulsed CO2 laser radiation on root
Martin H, Cunningham MJ (1983) Endosonic endodontics, the
canals with AgCl fibers: a scanning and transmission
ultrasonic synergistic system. In: Gerstein H, ed. Techniques
electron microscopic study. Journal of Endodontics 19,
in Clinical Endodontics. Philadelphia, PA, USA: WB Saunders,
Ørstavik D, Haapasalo M (1990) Disinfection by endodontic
Martin H, Cunningham WT, Norris JP, Cotton WR (1980)
irrigants and dressings of experimentally infected dentinal
Ultrasonic versus hand filing of dentin: a quantitative
tubules. Endodontics and Dental Traumatology 6, 142–9.
study. Oral Surgery, Oral Medicine and Oral Pathology 49,
Outhwaite WC, Livingston MJ, Pashley DH (1976) Effects of
changes in surface area, thickness, temperature and post-
McComb D, Smith DC (1975) A preliminary scanning electron
extraction time on human dentine permeability. Archives of
microscopic study of root canals after endodontic proce-
Oral Biology 21, 599–603.
dures. Journal of Endodontics 1, 238–42.
Park DS, Torabinejad M, Shabahang S (2004) The effect of
McComb D, Smith DC, Beagrie GS (1976) The results of in vivo
MTAD on the coronal leakage of obturated root canals.
endodontic chemomechanical instrumentation-a scanning
Journal of Endodontics 30, 890–2.
electron microscopic study. Journal of the British Endodontic
Pashley DH (1984) Smear layer: physiological considerations.
Society 9, 11–8.
Operative Dentistry Supplement 3, 13–29.
Meryon SD, Brook AM (1990) Penetration of dentine by three
Pashley DH (1985) Dentin-predentin complex and its perme-
oral bacteria in vitro and their associated cytotoxicity.
ability: physiologic overview. Journal of Dental Research 64
International Endodontic Journal 23, 196–202.
Spec Iss, 613–20.
Meryon SD, Jakeman KJ, Browne RM (1986) Penetration
Pashley DH (1992) Smear layer: overview of structure and
in vitro of human and ferret dentine by three bacterial
function. Proceedings of the Finnish Dental Society 88(Suppl
species in relation to their potential role in pulpal inflam-
1), 215–24.
mation. International Endodontic Journal 19, 213–20.
Pashley DH, Depew DD (1986) Effects of the smear layer,
Meryon SD, Tobias RS, Jakeman KJ (1987) Smear removal
Copalite, and oxalate on microleakage. Operative Dentistry
agents: a quantitative study in vivo and in vitro. Journal of
11, 95–102.
Prosthetic Dentistry 57, 174–9.
Pashley DH, Michelich V, Kehl T (1981) Dentin permeability:
Michelich VJ, Schuster GS, Pashley DH (1980) Bacterial
effects of smear layer removal. Journal of Prosthetic Dentistry
penetration of human dentin in vitro. Journal of Dental
46, 531–7.
Research 59, 1398–403.
Pashley DH, Tao L, Boyd L, King GE, Horner JA (1988)
Mohd Sulong MZA (1989) The incidence of postoperative pain
Scanning electron microscopy of the substructure of smear
after canal preparation of open teeth using two irrigation
layers in human dentine. Archives of Oral Biology 33, 265–
regimes. International Endodontic Journal 22, 248–51.
Moodnik RM, Dorn SO, Feldman MJ, Levey M, Borden BG
Pashley DH, Depew DD, Galloway SE (1989) Microleakage
(1976) Efficacy of biomechanical instrumentation: a scan-
channels: scanning electron microscopic observation. Oper-
ning electron microscopic study. Journal of Endodontics 2,
ative Dentistry 14, 68–72.
Perez F, Calas P, Rochd T (1996) Effect of dentin treatment on
Moorer WR, Wesselink PR (1982) Factors promoting the
in vitro root tubule bacterial invasion. Oral Surgery, Oral
tissue dissolving capability of sodium hypochlorite. Interna-
Medicine, Oral Pathology, Oral Radiology and Endodontics 82,
tional Endodontic Journal 15, 187–96.
ª 2010 International Endodontic Journal
International Endodontic Journal, 43, 2–15, 2010
Smear layer in endodontics Violich & Chandler
Prati C, Selighini M, Ferrieri P, Mongiorgi R (1994) Scanning
smear layer on root canal walls. Journal of Endodontics 24,
electron microscopic evaluation of different endodontic
procedures on dentin morphology of human teeth. Journal
Takeda FH, Harashima T, Kimura Y, Matsumoto K (1999) A
of Endodontics 20, 174–9.
comparative study of the removal of smear layer by three
Rubin LM, Skobe Z, Krakow AA, Gron P (1979) The effect of
endodontic irrigants and two types of laser. International
instrumentation and flushing of freshly extracted teeth in
Endodontic Journal 32, 32–9.
endodontic therapy: a scanning electron microscope study.
Taylor JK, Jeansonne BG, Lemon RR (1997) Coronal leakage:
Journal of Endodontics 5, 328–35.
effects of smear layer, obturation technique, and sealer.
Ruddle CJ (2007) Hydrodynamic disinfection: tsunami end-
Journal of Endodontics 23, 508–12.
odontics. Dentistry Today 26(5), 114–7.
Tewfik HM, Pashley DH, Horner JA, Sharawy MM (1993)
Sabbak SA, Hassanin MB (1998) A scanning electron micro-
Structural and functional changes in root dentin following
scopic study of tooth surface changes induced by tannic
exposure to KTP/532 laser. Journal of Endodontics 19, 492–
acid. Journal of Prosthetic Dentistry 79, 169–74.
Safavi KE, Spa˚ngberg LSW, Costa NS Jr, Sapounas G (1989)
Tidmarsh BG (1978) Acid-cleansed and resin-sealed root
An in vitro method for longitudinal evaluation of toxicity of
canals. Journal of Endodontics 4, 117–21.
endodontic sealers. Journal of Endodontics 15, 484–6.
Tidswell HE, Saunders EM, Saunders WP (1994) Assessment
Safavi KE, Spa˚ngberg LSW, Langeland K (1990) Root canal
of coronal leakage in teeth root filled with gutta-percha and
dentinal tubule disinfection. Journal of Endodontics 16, 207–
a glass of ionomer root canal sealer. International Endodontic
Journal 27, 208–12.
Saleh IM, Ruyter IE, Haapasolo M, Ørstavik D (2008) Bacterial
Timpawat S, Sripanaratanakul S (1998) Apical sealing ability
penetration along different root canal filling materials in the
of glass ionomer sealer with and without smear layer.
presence or absence of smear layer. International Endodontic
Journal of Endodontics 24, 343–5.
Journal 41, 32–40.
Timpawat S, Vongsavan N, Messer HH (2001) Effect of
Saunders WP, Saunders EM (1992) The effect of smear layer
removal of the smear layer on apical microleakage. Journal
upon the coronal leakage of gutta-percha root fillings and a
of Endodontics 27, 351–3.
glass ionomer sealer. International Endodontic Journal 25,
Torabinejad M, Khademi AA, Babagoli J et al. (2003) A new
solution for the removal of the smear layer. Journal of
Saunders WP, Saunders EM (1994) Influence of smear layer
Endodontics 29, 170–5.
on the coronal leakage of Thermafil and laterally condensed
Vassiliadis L, Liolios E, Kouvas V, Economides N (1996) Effect
gutta-percha root fillings with a glass ionomer sealer.
of smear layer on coronal microleakage. Oral Surgery, Oral
Journal of Endodontics 20, 155–8.
Medicine, Oral Pathology, Oral Radiology and Endodontics 82,
Schmid R, Reilley C (1957) New complexion for titration of
calcium in the presence of magnesium. Annals of Chemistry
Walker TL, del Rio CE (1989) Histological evaluation of
29, 264–8.
ultrasonic and sonic instrumentation of curved root canals.
Shahravan A, Haghdoost AA, Adl A, Rahimi H, Shadifar F
Journal of Endodontics 15, 49–59.
(2007) Effect of smear layer on sealing ability of canal
Walker TL, del Rio CE (1991) Histological evaluation of
obturation: a systematic review and meta-analysis. Journal
ultrasonic debridement comparing sodium hypochlorite and
of Endodontics 33, 96–105.
water. Journal of Endodontics 17, 66–71.
van der Sluis LWM, Versluis M, Wu MK, Wesselink PR (2007)
Wayman BE, Kopp WM, Pinero GJ, Lazzari EP (1979) Citric
Passive ultrasonic irrigation of the root canal: a review of
and lactic acids as root canal irrigants in vitro. Journal of
the literature. International Endodontic Journal 40, 415–26.
Endodontics 5, 258–65.
Stabholz A, Neev J, Liaw LH, Stabholz A, Khayat A,
White RR, Goldman M, Lin PS (1984) The influence of the
Torabinejad M (1993) Effect of ArF-193 nm excimer laser
smeared layer upon dentinal tubule penetration by plastic
on human dentinal tubules. A scanning electron micro-
filling materials. Journal of Endodontics 10, 558–62.
scopic study. Oral Surgery, Oral Medicine and Oral Pathology
White RR, Goldman M, Lin PS (1987) The influence of the
smeared layer upon dentinal tubule penetration by end-
Stewart GG, Kapsimalas P, Rappaport H (1969) EDTA and
odontic filling materials. Part II. Journal of Endodontics 13,
urea peroxide for root canal preparation. Journal of the
American Dental Association 78, 335–8.
Wikesjo¨ UM, Baker PJ, Christersson LA et al. (1986) A
Takeda FH, Harashima T, Kimura Y, Matsumoto K (1998a)
biochemical approach to periodontal regeneration: tetracy-
Comparative study about the removal of smear layer by
cline treatment conditions dentin surfaces. Journal of Peri-
three types of laser devices. Journal of Clinical and Laser
odontal Research 21, 322–9.
Medical Surgery 16, 117–22.
Williams S, Goldman M (1985) Penetrability of the smeared
Takeda FH, Harashima T, Kimura Y, Matsumoto K (1998b)
layer by a strain of Proteus vulgaris. Journal of Endodontics
Efficacy of Er:YAG laser irradiation in removing debris and
11, 385–8.
International Endodontic Journal, 43, 2–15, 2010
ª 2010 International Endodontic Journal
Violich & Chandler Smear layer in endodontics
Yamada RS, Armas A, Goldman M, Lin PS (1983) A scanning
Yang SE, Bae KS (2002) Scanning electron microscopy
electron microscopic comparison of a high volume final
study of the adhesion of Prevotella nigrescens to the
flush with several irrigating solutions: Part 3. Journal of
dentin of prepared root canals. Journal of Endodontics 28,
Endodontics 9, 137–42.
ª 2010 International Endodontic Journal
International Endodontic Journal, 43, 2–15, 2010
Source: http://www.endodonticcentre.ca/Sites/EndodonticCentre/uploads/documents/28110413093400.pdf
nysdental.org
Be on the Giving End of Mercy New York Mission of Mercy is opportunity to make a difference and show you care. access to care is a big problem in the united and care to those in need. mid-level providers could states. many people go without needed dental care provide palliative care until the patient can secure for a variety of reasons. there are no dentists in
Gaafar_f_rev
STIMULATION AND CONTROL OF E. COLI BY USING AN EXTREMELY LOW FREQUENCY MAGNETIC FIELD EL-SAYED A. GAAFAR*, MAGDA S. HANAFY**, EMAN Y. TOHAMY***, MONA H. IBRAHIM** * Biophysics Department, Faculty of Science, Cairo University, Egypt ** Physics Department, Faculty of Science, Zagazig University, Egypt *** Botany Department, Faculty of Science, Zagazig University, Egypt