Msif 06 pp1-28 • english

MS in Focus Issue One • 2003
Issue One • 2002
MS in focus
Issue 6 • 2005
Intimacy and
Sexuality
The Magazine of the Multiple Sclerosis International Federation
MS in focus Issue 6 • 2005
Executive Editor Nancy Holland, EdD, RN, MSCN, Vice
Multiple Sclerosis
President, Clinical Programs and Professional Resource
Centre, National Multiple Sclerosis Society USA.
Editor and Project Leader Michele Messmer Uccelli, BA,
MSIF is a unique collaboration of national MS
MSCS, Department of Social and Health Research, Italian
societies and the international scientific
Multiple Sclerosis Society, Genoa, Italy.
Managing Editor Helle Elisabeth Lyngborg, Information
and Communications Manager, Multiple Sclerosis
It leads the global MS movement in sharingbest practice to significantly improve the
quality of life of people affected by MS and in
Editorial Assistant Chiara Provasi, MA, Project Co-
stimulating research into the understanding
ordinator, Department of Social and Health Research, Italian
and treatment of the condition.
Multiple Sclerosis Society, Genoa, Italy.
MSIF Responsible Board Member
Our priorities are:
Prof Dr Jürg Kesselring, Chair of MSIF International Medical
• Stimulating global research• Stimulating the active exchange of
and Scientific Board, Head of the Department of Neurology,
Rehabilitation Centre, Valens, Switzerland.
• Providing support for the development of
Editorial Board Members
new and existing MS societies
Guy Ganty, Head of the Speech and Language Pathology
Department, National Multiple Sclerosis Centre, Melsbroek,
All of our work is carried out with thecomplete involvement of people living
Katrin Gross-Paju, PhD, Estonian Multiple Sclerosis Centre,
West Tallinn Central Hospital, Tallinn, Estonia.
Marco Heerings, RN, MA, MSCN, Nurse Practitioner,
Groningen University Hospital, Groningen, The Netherlands.
Designed and produced by
Kaye Hooper, BA, RN, RM, MPH, MSCN, Nurse Consultant
Cambridge Publishers Ltd
275 Newmarket Road Cambridge
Martha King, Director of Publications, National Multiple
Sclerosis Society, USA.
Elizabeth McDonald, MBBS, FAFRM, RACP, Medical
Director, MS Society of Victoria, Australia.
Elsa Teilimo, RN, UN Linguist, Finnish Representative,
Persons with MS International Committee.
Chloe Neild, Information Management Coordinator, MS
Cover image courtesy of Honoria Starbuck, PhD,
Society of Great Britain and Northern Ireland.
Life Drawing Instructor, Art Institute Online
Copy Editor
Emma Mason, BA, Essex, UK.

MS in focus Issue 6 • 2005
Letter from the Editor
Sexuality and intimate relationships are a
significant part of life and well-being. For mostpeople, sexuality and its expression are a natural
Introduction to Intimacy and
and important component of self-concept,
emotional well-being, and overall quality of life.
Sexual dysfunction in
Factors such as culture, religion and self-esteem
contribute to how a person experiences sexuality. While MS mayalter functioning, the desire for a sexual identity, love, affection
Sexual dysfunction in men
and intimacy remains. Given this, sexuality may be a source of
significant frustration for many people with MS.
Secondary causes of
This issue of MS in focus presents a discussion of intimacy and
sexuality. Often these topics are not easy to discuss. This is truefor people with MS as well as for many healthcare professionals.
Tertiary causes of
For some individuals and couples living with MS, intimacy and
sexuality receive little or no priority, and instead their focus andemotional resources are concentrated on dealing with other
Your questions answered
problems related to the disease.
Interview with Rolande Cutner
Whether a person is in an intimate relationship or not, it is achallenge to maintain a sexual identity and take care of one's
MS Society of Norway: Support
sexual self-esteem (how one feels about oneself as a sexual
group for lesbians and gay men
being) while dealing with a chronic illness such as MS. It is
with multiple sclerosis
particularly challenging in cultures where society placesimportance on qualities that are not always consistent with
Results of the online survey
chronic illness, such as beauty, health and independence.
Quality of Life Principles
With this issue of MS in focus we hope to increase awarenessof the fact that sexual problems are a direct result of
demyelination, can be a result of other MS symptoms and that
Subscription details
psychological, social and cultural aspects influence anindividual's sexuality.
The next issue of MS in focus will be on
We also hope that this issue will serve as a resource for
Rehabilitation. Send questions and
professionals who encounter difficulties in discussing intimacy
letters to [email protected] or marked for
and sexuality issues with people with MS.
the attention of Michele Messmer
Michele Messmer Uccelli, Editor
Uccelli at the Italian MS Society, ViaOperai 40, Genoa, Italy 16149.
Editorial Statement
The content of MS in focus is based on professional knowledge and experience. The editor andauthors endeavour to provide relevant and up-to-date information. Information provided through MSin focus is not intended to substitute for advice, prescription or recommendation from a physician orother healthcare professional. For specific, personalised information, consult your healthcareprovider. MSIF does not approve, endorse or recommend specific products or services, butprovides information to assist people in making their own decisions.

MS in focus Issue 6 • 2005
Introduction to
intimacy and
sexuality in MS
By Fred Foley, PhD, Bernard Gimbel MS Center, New Jersey and Albert Einstein
College of Medicine, New York, USA
Multiple sclerosis can cause changes that affect
Sexual changes in MS:
one's usual ways of expressing sexuality. Everyone
frequency and characteristics
with MS retains the capacity to give and receive love
Studies have been completed on the prevalence of
and pleasure, although creative problem-solving is
sexual and relationship problems in MS in a number
sometimes necessary to find avenues for intimate
of countries. Although normal sexual function
expression. Understanding how MS symptoms
changes throughout the lifespan, MS can affect an
might affect intimacy and sexuality represents a
individual's sexual experience in a variety of ways.
crucial step towards overcoming obstacles
Studies on the prevalence of sexual problems in MS
effectively. Whether one is newly diagnosed,
indicate that 40-80 per cent of women and 50-90
physically disabled, young, mature, single or in a
per cent of men have sexual complaints or concerns.
committed relationship, MS does not diminish the
The most frequently reported changes in men are a
universal human need to give and receive love and
diminished capacity to attain or maintain an erection,
intimate pleasure.
and difficulty having an orgasm. The most frequentchanges that women report are a partial or total lossof libido (sexual desire), vaginal dryness/irritation,diminished orgasm, and uncomfortable sensorychanges in the genitals.
Sexual changes in MS can best be characterised asprimary, secondary, or tertiary in nature. Primarysexual dysfunction stems from changes to thenervous system that directly impair the sexualresponse and/or sexual feelings. Primarydisturbances can include partial or total loss of libido(sexual desire), unpleasant or decreased sensationsin the genitals, decreased vaginal lubrication orerectile capacity, and decreased frequency and/orintensity of orgasm. Secondary sexual dysfunctionrefers to MS-related physical changes that indirectlyaffect the sexual response. Bladder and/or boweldysfunction, fatigue, spasticity, muscle weakness,
MS in focus Issue 6 • 2005
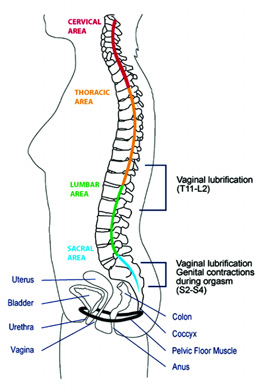
problems with attention and concentration, hand
(middle) and sacral (lower) spinal cord and genitals
tremors, and non-genital changes in sensation are
throughout the sexual response cycle. Since MS can
amongst the most common MS symptoms that can
result in randomly distributed lesions along many of
cause secondary sexual dysfunction. Tertiary sexual
these myelinated pathways, it is not surprising that
dysfunction results from psychosocial and cultural
changes in sexual function are reported so
issues that can interfere with sexual feelings and
frequently. The good news is that there are likely to
sexual response. Depression, performance anxiety,
be neurologic pathways that mediate aspects of
changes in family roles, lowered self-esteem, body-
sexual feelings and response that are widely
image concerns, loss of confidence, and internalised
distributed and therefore unaffected by MS lesions.
beliefs and expectations about what defines a"sexual man" or a "sexual woman" in the context of
The subsequent articles in this issue of MS in focus
having a disability, can all be expressions of, or
will discuss in greater detail the important aspects of
contribute to, tertiary sexual dysfunction.
sexual functioning as related to MS, includingstrategies for enhancing sexual desire,
The central nervous system
communicating with a sexual partner and managing
and sexual response
other symptoms of the disease that can inhibit
Sexual response is mediated by the central nervous
sexual expression.
system – the brain and spinal cord. There is nosingle sexual centre in the central nervous system.
Unfortunately, healthcare providers rarely bring up
Many different areas of the brain are involved in
the subject of sexuality, because of personal
various aspects of sexual functioning, including sex
discomfort, lack of professional training in this area,
drive, perception of sexual stimuli and pleasure,
or fears of being overly intrusive. It is critical to
movement, sensation, cognition, and attention.
discuss changes in sexual feelings and strategies
Sexual messages are communicated between
and treatments that are available to enhance
various sections of the brain, thoracic (upper), lumbar
Body Mapping
Developing a "sensory body map" to explore the exact locations of pleasant, decreased, or altered
sensations can improve intimate communication and set the stage for increasing pleasure.
Conduct a "sensory body mapping" exercise
Next, inform your partner of your "body map"
(15 – 20 minutes):
information and instruct him/her in touching
Begin by systematically touching the body
you in a similar fashion.
from head to toe (or all those places you cancomfortably reach).
Have your partner provide the sameinformation for you (about his or her "body
Conduct this exercise without your clothes on,
map"). Take turns providing pleasure to each
in a place that is private, relaxing, and a
other, without engaging in sex or trying to
Vary the rate, rhythm, and pressure of your touch.
Remember, the emphasis is on communication
Note areas of sensual pleasure, discomfort, or
and pleasure, not sex or orgasm. This exercise
sensory change. Alter your pattern of touch to
sets the stage to rediscover pleasure in the face
maximise the pleasure you feel (without trying
of reduced desire.
to obtain sexual satisfaction or orgasm).
MS in focus Issue 6 • 2005
Sexual dysfunction
in women with MS
By Farida Sharon van Rey, MD,
Female sexual dysfunction is very common inwomen with neurological conditions, including MS.
Neuro-urology Research Fellow,
The majority of women with MS suffer from sexualdysfunction at some stage of the disease. Compared
University Medical Centre St.
to a general female population, in which 20-50 per
Radboud, Nijmegen, The Netherlands
cent of women are affected, the prevalence ofsexual dysfunction is estimated to be as high as 80per cent in women with MS. Sexual dysfunction hasa major impact on quality of life and interpersonalrelationships. For many women it is a physicallydisquieting, emotionally disturbing and sociallydisruptive disorder. In spite of its high prevalence,these aspects of an individual's well-being havebeen considerably neglected until recently, makingfemale sexual dysfunction a very important but oftenoverlooked symptom of MS.
How the body behaves during the sexual
response
Two basic physical processes that occur during the
sexual response: vasocongestion and myotonia.
Vasocongestion refers to the concentration of bloodin the blood vessels and the tissues of the genitalsand breasts. In women, this inflow of blood causesthe clitoris to enlarge, the labia to swell, and thevagina to lubricate.
Myotonia, or neuromuscular tension, refers to theincrease of energy in the nerves and muscles.
During sexual activity, myotonia takes placethroughout the body, not only in the genital region,but throughout the trunk, particularly in the breastand chest wall.
For women, vasocongestion in the vaginal walls
The sexual response centres in women
causes vaginal secretion to seep through the vaginal
MS in focus Issue 6 • 2005
lining, moistening the inner surface of the vagina.
reduced vaginal lubrication and difficulty with arousal
The amount of lubrication or "wetness" present in
(35 per cent), and difficulty or inability reaching
the vagina does not necessarily coincide with a
orgasm (72 per cent). Pain during intercourse is also
woman's degree of arousal or desire for intercourse.
a frequently reported symptom in women with MS,
Swelling of the clitoris and of the labia also occurs in
which may be due to vaginal dryness, spasticity or
response to vasocongestion during the excitement
hypersensitivity.
phase. In addition, the inner two-thirds of the vaginalengthens and expands, the cervix and uterus
elevate, and the outer lips of the vagina flatten and
Since the sexual response in women with MS is
separate. Nipples may become erect, breasts slightly
related to many different factors, a
enlarged, and the veins in the breasts may appear
comprehensive assessment of all these aspects
more visible.
must be taken into account. An evaluation shouldconsist of a full medical history, physical
How and why MS can affect sexual
examination and pelvic examination. Although
sexual dysfunction in women with MS often has a
Sexual dysfunction in women has many causes and
neurological cause, its evaluation is not always
effects. Abnormalities in blood circulation, hormonal
included in routine clinical practice. Often it is
state, nerve functioning and mental well-being may
possible for a clinician to become aware of a
influence sexual functioning. Therefore, one or more
problem and begin to evaluate it based on
of these factors can result in sexual dysfunction.
information provided by the individual during the
Lesions in the brain can interfere with the inter-
visit, in response to a few relevant questions.
pretation of sexual stimuli as arousing, while lesions
Initiating these questions is not always part of the
of the spinal cord can interfere in the transmission
healthcare professionals' routine, with the result
of arousing nerve signals to the genitals. Lesions in
that important information is missed by the
the sacral (lower) spinal cord can also cause
professional and problems experienced by the
primary sexual dysfunction, by inhibiting or
person with MS are left unaddressed.
preventing vasocongestion, resulting in diminishedor absent clitoral swelling and/or vaginal lubrication.
Possible treatments
Oestrogen creams may be useful for women
In primary sexual dysfunction, MS lesions in the
experiencing vaginal dryness, pain or burning.
spinal cord may make it difficult to sustain
Another treatment for these symptoms is a vaginal
clitoral/vaginal engorgement during the plateau
suppository, although this form may not be available
phase (between arousal and orgasm). In addition,
in all countries. Unfortunately, many of the
sensory changes in the genitals can interrupt or
medications that appear to be effective for the
diminish nerve signals that initiate and/or maintain
treatment of male sexual dysfunction related to MS
vasocongestion at both the spinal cord and cerebral
have proved either to be ineffective for other
cortex (brain) levels.
symptoms of female sexual dysfunction or have notbeen studied fully at this time.
Types and frequencies
Approximately 80 per cent of women with MS
experience sexual dysfunction at some time during
Sexual dysfunction is highly prevalent among
the course of the disease. Some women stop
women with MS. Assessment and treatment of
engaging in sexual relations while others
these problems is complicated. Addressing sexual
(approximately 40 per cent) have reported that
problems during routine visits is important in
participating in sexual relations is significantly
identifying and managing symptoms that can have
unsatisfactory. Symptoms most commonly reported
a negative impact on an individual's personal life as
include reduced genital sensation (48 per cent),
well as on the life of the couple.
MS in focus Issue 6 • 2005
Sexual dysfunction
in men with MS
By Douglas W. Lording, Medical Director, Melbourne Andrology Centre, Victoria, Australia
Sexual activity for men usually requires the co-ordinationof arousal, penile erection and orgasm includingejaculation, along with the many other emotional andrelationship components that are integral for satisfaction.
Direct disruption of nerve pathways controlling erectionand ejaculation are common.
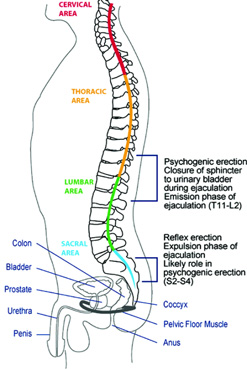
Erectile dysfunction
An erection occurs when there is relaxation of the
muscle cells in the wall of the penile blood vessels
and the erectile tissue, leading to the penis filling
with blood. Relaxation of these muscle cells is
initiated by nitric oxide (NO) release from nerves
coming from the lower spinal cord. The messages
transmitted by these nerves usually arise in the
brain and pass down to the lower spinal cord.
Erectile dysfunction (ED) is the commonest sexual
dysfunction in men and usually is due to disease of
the vascular or neurological systems, but
psychosexual influences are also important. ED
can have a major impact on self-esteem,
relationships and general well-being.
In men with MS, lesions in the spinal cord thatinterfere with the passage of nerve impulses fromthe brain may cause ED. The limited studies of
The sexual response centres in men
men with MS indicate that ED is a frequentsymptom, often affecting younger men and
These responses are also triggered by nerve
sometimes affecting fertility.
impulses that traverse the spinal cord fromimportant brain centres.
Ejaculatory dysfunction
At ejaculation there is widespread muscle
Often, delayed ejaculation and complete failure of
contraction in the pelvic area that leads to
ejaculation (anejaculation) are caused by disruption
expulsion of the semen and much of the sensation
of the nerve pathways and may be part of a
associated with the broader response of orgasm.
broader orgasmic failure.
MS in focus Issue 6 • 2005
Ejaculatory disturbances also occur in MS,
underlying disorder. However, consideration
although there is less information about the
should always be given to improving potentially
prevalence. Anti-depressant medications (see
reversible aspects. Drugs used to modify MS
page 16) that may be used in MS often cause
progression also could help.
ejaculatory problems as a side-effect. Some menwith MS may develop premature ejaculation
The most commonly used medications act to
because of anxiety about their disease.
enhance the relaxation of muscle cells in thepenis. Sildenafil, tadalafil and vardenafil all act in
this way through a similar mechanism. They are
Testosterone is active in several brain centres
safe, well-tolerated medications and observation
important for sexual thoughts and desire (libido)
of their use in MS and spinal cord injury confirm a
and low levels are associated with depression
high efficacy, with about three-quarters of men
and obesity, both of which can relate to MS.
experiencing satisfactory outcomes.
Frequently, desire is affected by factors otherthan the direct physical component of the
Education about how to achieve the best results
disease, and this is particularly so in MS where
is the most important aspect of the use of these
other physical and psychological factors, such as
medications. They need to be taken at least half
fatigue, may play a major role.
an hour before sex, but some couples find theidea of premeditating their sexual experience off-
putting, and this often interferes with treatment.
Not all men with ED (or even health
Normal sexual stimulation is required to initiate
professionals) find it easy to talk about sex, and
the erection, therefore the couple needs to be in
they may not raise this distressing issue. It is
the mood for sex. Apprehension about the
important to note that sexual dysfunction is
outcome may result in less than optimal results
diagnosed by taking a careful history; there are
for the first few doses. Persistence, medical
no diagnostic tests. Men with MS may have other
review and re-instruction are important for
causes of sexual dysfunction and the assessment
successful results.
should take this into account. Simple blood teststo exclude diabetes, high cholesterol and
testosterone deficiency are recommended.
These drugs can cause mild headaches, flushing,
Careful assessment of the impact of medications
nasal congestion, indigestion and muscle aches,
and substance use is important.
but these adverse effects usually do not precludetheir use. When sildenafil was launched, much
The importance of assessing both the man with
was said of possible adverse cardiac effects and
MS and his partner cannot be over-emphasised,particularly if initial treatment is not successful.
Tips for successful treatment
This will require more developed skills that not alldoctors will have.
• Discuss sexual dysfunction
• Involve both partners
Treating erectile dysfunction
The neurologist or MS nurse should ask men with
Go through the history carefully
MS if they are having erectile dysfunction. If they
• Do not forget non-MS causes
do, the impact of this important disorder needs to
• Use medications properly
be assessed and, if it is considered significant, afull range of treatment options should be
• Consider sex in broad terms
discussed. Treatment is usually erection-
• Be prepared to experiment
promoting medications rather than treating the
MS in focus Issue 6 • 2005
this still worries some men and their partners.
There is a potentially harmful reaction with allthese drugs when used with nitrates (mainly usedto treat angina), and men with active heartdisease, for whom the level of physical activityduring sexual intercourse is potentiallydangerous, should use these drugs with caution.
Alternative ED treatments
If these drugs do not work or cannot be safely
used, injecting drugs into the penis or the use of
mechanical aides may be helpful. Prostaglandin
E1 can be injected directly into the penis. This
relaxes the muscle cells and usually induces a
hard, lasting erection. Significant dexterity and
common sense are essential for self-injection.
Penile pain, nodular scarring within the erectile
bodies and unduly prolonged erection may occur.
The dosing regimen prescribed must be followed
strictly.
Some men with partial ED can obtain a gooderection using a penile ring, usually combinedwith a vacuum device. The latter draws moreblood into the penis while the ring, applied afterblood flow into the penis is sufficient, reduces
prosthesis can be implanted so that cylinders
blood flow out of the penis. If all else fails, a penile
implanted into the shaft of the penis can be filledfrom a fluid reservoir placed in the scrotum.
Getting the best
Treatment of ejaculatory disorders and low
from ED medications
1. Ensure mechanism of action is
Unlike ED, there is no medication that acts
understood, in particular:
directly to improve ejaculatory problems or lowdesire. Emphasis will be on optimising physical
a. Timing of dosing
and emotional well-being. The ED drugs are often
b. Need for normal sexual stimulation
tried where there is difficulty achieving ejaculation
c. Effect of food and alcohol
and orgasm, as there is often a degree of ED as
2. Allow at least four attempts at using the
well. In addition, there is usually heightened
stimulation with a harder erection. Different
3. Address secondary and tertiary sexual
positions help some men to be more stimulated
and some benefit from mechanical assistance, forexample using a vibrator.
4. Review outcome of treatment after
Couples should be reassured that satisfying sex
5. Remember support and understanding
can be achieved without full erection and
penetration, and that partner satisfaction can beachieved by a variety of stimulating techniques.
MS in focus Issue 6 • 2005
Secondary causes
of sexual problems
By Dorothea C. Pfohl, RN MSCN, MS Center Clinical Co-ordinator,
University of Pennsylvania, Philadelphia, USA
MS changes can affect sexual response by making
find creative ways to keep the physical expressions
sexual activity difficult physically and emotionally.
Symptoms common to MS, such as fatigue orchanges in muscle tone, lack of coordination or pain,
A person who does not feel well or thinks of himself
can frustrate sexual expression and extinguish
or herself as unattractive because of a less-than-
desire. Bowel and bladder dysfunction can inhibit
perfect body may shun sex or find their love life
and cause embarrassment. Cognitive changes
deteriorating. People who are not in a relationship
challenge the most devoted couple, yet in the
may be reluctant to date and develop new love
presence of any of these symptoms, it is possible to
interests. Secondary sexual dysfunction often
MS in focus Issue 6 • 2005
indirectly affects sexual response and ability to
available help can lessen anxiety. Planning for rest
perform in both men and women with MS.
time together can lessen fatigue and
Sexual complaints are common in the general
simultaneously meet the need for additional time
population and are capable of having a profound
impact on quality of life and relationships. Addingchronic illness to the picture makes problems more
Medications are available which can be used to
likely, yet such concerns and complaints are not
counteract fatigue, but others actually contribute to
always shared with partners or healthcare
it. If medication side-effects are suspected to be
professionals. Nevertheless, strategies exist which
worsening the fatigue, a schedule adjustment
can be employed to cope with and manage
could provide respite. A dose can be timed to allow
symptoms, promote intimacy, strengthen
for more energy when intimacy is planned.
relationships and encourage sexual pleasure and
Disease-modifying therapy schedules, like other
medications, should be reviewed with a healthcareprovider who can advise and educate about
adjustments that minimise untoward effects. At
Fatigue is perhaps the most common symptom
times, a dose can be skipped or postponed to avoid
reported by people with MS, and it can be the most
the side-effect that is getting in the way of sexual
disabling. For a complete discussion on the different
performance or interest.
types and causes of fatigue, see Issue 1 of MS infocus (January 2003). Regardless of the type orcause of fatigue, it can have a negative affect on
Both the person with MS and the
interest in sex and lead to a reluctance to initiate
partner deserve to have their
lovemaking, or even an avoidance of intimacy. The
sensitivities and willingness to accept
well partner may misunderstand this "disinterest"and loss of pleasure and resent the person with MS.
or reject various forms of sexual
This may come at a time when they are assuming
additional responsibilities, coping with changingroles or it may be perceived as a personal rejection.
Often, partners fear hurting the person with MS.
Effective communication requires that feelings beshared and dealt with openly and honestly, thusmaking it possible to explore options for maintaininga satisfactory sexual relationship despite physicalchanges.
Energy conservation measures can be employed tomanage fatigue. These techniques can be appliedto sexual issues as well. Time for intimacy may needto be prioritised, perhaps for the time of day whenthe person with MS has the most energy. Onecouple set up a weekly "date" when both could takea long lunch. Planning and anticipating their timetogether during the day when the children were atschool became a pleasure in itself. Lifestylechanges may need to be made when there are notenough hours in the day to accomplish all thatneeds to be done. Simplifying tasks and accepting
MS in focus Issue 6 • 2005
go hand in hand with sexual dysfunction, since
Muscle weakness may necessitate alterations in
nerve pathways are shared or close to each other.
sexual practices. Comfort measures, such as
Incontinence, or even fear of having an accident,
properly placed pillows, provide additional support
can cause a person to avoid sex entirely, thus
and can be playfully used to "set the scene" for
depriving them of the closeness it brings.
romance. Discussing new positions and variousexpressions of sexuality, such as massage or oral
There are many ways to deal with involuntary
sex, can add excitement to the relationship and
elimination, but discussing the possibility of losing
boost, rather than diminish, self-image. Partners
urine or stool during sex, and having a plan should it
may or may not be comfortable with such variations
occur defuses the situation and can allow the
or may be unwilling to engage in "sex play". Both the
couple to manage their concerns without spoiling
person with MS and the partner deserve to have
the moment. Bowel and bladder rehabilitation plans
their sensitivities and willingness to accept or reject
can include toileting regimens designed for the
various forms of sexual pleasuring respected.
unique needs of individuals and couples. For
Rejecting an alternative that compensates for
example, steps such as limiting fluid intake for a few
limitations imposed by MS symptoms need not be a
hours before sexual activity can be effective. For
rejection of the person, and other ideas can be
men, leakage of small amounts of urine can be
managed by wearing a condom. For both sexes,simply padding the bed well can help everyone
De-conditioning (weakness from inactivity) can be
relax. Another strategy is performing intermittent
helped by a fitness programme modified to work
self-catheterisation prior to intimacy. This technique
with the person's physical limitations. Kegel
serves to empty the bladder completely, giving the
exercises are a type of exercise that can improve
person more confidence that he or she will not be
decreased vaginal tone by strengthening the pelvic
embarrassed by an accident during sexual
floor muscles. See Issue 2 of MS in focus (July
2003) for information on how pelvic floor exercisesare performed.
Urinary tract infections are common in MS and aresometimes aggravated by sexual activity. Proper
Lack of coordination and tremor
evaluation and treatment of bladder problems can
Lack of coordination may make sex and sexual
go far to maintaining quality of life and
expression feel clumsy, as can tremor. But besides
independence. In-dwelling catheters make the
being awkward, these symptoms may also interfere
logistics of intercourse difficult but not impossible.
with the couple's style of having sex. It must be
With advice from a healthcare provider, often the
remembered that persons with MS still have needs
bag can be emptied and then clamped for a period
for contraception and protection from sexually
of time. Taping a long drainage tube to a woman's
transmitted disease, but previously-used methods
abdomen can avoid pulling and will place the
may no longer be practical. A partner may need to
catheter well out of the way. Similarly, a catheter in
help with the condom or insert the diaphragm and it
the penis can be folded back on itself, clamped and
may be difficult to change from being a care partner
taped and a condom placed over it all.
to being a lover. Again, good communicationbetween partners and advice from professionals
can minimise embarrassment and maximise
Pain can impact significantly on interest in sex as
closeness and pleasure.
well as performance ability. Medications used torelieve pain may add to sleepiness or fatigue.
Bowel and bladder problems
Understanding the type of pain can influence the
Another source of anxiety and distress can be
best way to manage it. Muscle tightness, intense
bowel and bladder disturbances. These problems
itching and spasticity may all be called "pain".
MS in focus Issue 6 • 2005
Medications that bring relief must be well chosen
expectations from performance-oriented sex, where
for the type of pain they treat and used in just the
intercourse is seen as the only desirable outcome,
right dose and frequency to give relief with the least
can be liberating and allows for pleasuring and
disadvantageous side-effects. An extra or well-
sexual satisfaction despite the limitations of
timed dose before intimacy can often provide
impaired mobility.
effective symptom management and reassure thepartner that he/she is not adding to discomfort. It is
also important that a symptom such as adductor
Cognitive changes can be amongst the most
spasms (which cause involuntary pulling together of
potentially damaging to the relationship, since they
the legs) is not seen as an indication of the person's
can undermine the person's sense of who he/she
interest or willingness to have sex. Again,
is. A partner may feel this is no longer the person
communication is the key to avoiding
they once knew. Changes in attention and
misunderstanding and hurt feelings. Water soluble
concentration may be perceived as lack of interest
lubricants can make intercourse more comfortable,
or love, and may irreparably strain the relationship.
without predisposing to urinary tract infection.
Changes in mood, memory loss and depression canbe frightening, frustrating and sometimes
infuriating. All interfere with intimacy. Individual or
Changes in sensation can also interfere with sexual
couples counselling may be advised.
pleasure (see page 5 on body mapping). Non-genitalsymptoms such as numbness and tingling can distract
Successful management of cognitive symptoms
and discourage either partner. Impaired genital
includes creating a stimuli-saturated, minimally-
sensations can diminish pleasure, while heightened
distracting environment. Partners can share what
sensitivity may make even the lightest touch
will and will not be seen as exciting and what
unbearable. What feels good at one time may be
promotes passion and interest.
excruciatingly painful on another occasion. Frankdiscussion of needs and limitations can avoid problems,
Many symptoms of MS are invisible while others are
and simple solutions as well as medications can be
painfully obvious. All can impact on quality of life
used to enhance pleasure. Something as easy as a
and sense of well-being. While life changes affect
bag of frozen peas gently rubbed on a woman's
everyone, changes from MS can directly and
perineum (genital area) can increase sensitivity and
indirectly affect sexuality. Successful management
pleasure and can be used as foreplay. Special oils are
requires creativity, communication, patience and
available which encourage touch and also increase
resource management so that a person is able to
pleasure when sensation is impaired. Vibrators can beused alone or with a partner.
Mobility
MS symptoms can indirectly affect the sexual
response. Devices used to compensate for loss of
function can also damage confidence and self-
image. They may be seen as less than sexy. Canes,
wheelchairs, braces and walkers are often identified
with being "sick" or "old". Spontaneity can be a
problem if great effort has to be made to get
around. Asking for help is often difficult. It can be
challenging to think of oneself as sexually desirable
when confronting a body that is less than perfect,
and requires extra care to maintain. Adjusting
MS in focus Issue 6 • 2005
Tertiary causes of
sexual problems
By Elizabeth McDonald, Medical Director, MS Society of Victoria, Australia,
Sexuality is an evolving, overall development of one's
The diagnosis of MS, combined with the
feelings of personal identity, well-being and self-
unpredictable nature of relapses and the uncertainty
esteem that involves both social and physical
of disease progression, often occurs at a time when
relationships. This is an individual lifelong process,
dreams and plans for the future are being
which is influenced significantly by personal
formulated and relationships and careers
perception, social conditioning, cultural and religious
established. The diagnosis of MS may well cloud an
individual's expectation of the future. This can resultin reactions of grief, anxiety and depression, lowering
The impact of MS on sexuality
self-esteem and reducing confidence. Such feelings
The onset of MS can alter a person's perception of
may cause reduced sexual interest and withdrawal
himself or herself as an individual, altering sexual
from sexual activity.
development and expressions of sexuality, and it canhave a negative impact on sexual and intimate
The fear of potential or actual disability can have a
functioning. These are known as the tertiary sexual
negative impact on the perception of body image.
problems of MS, derived from the resultant
People with MS may feel less sexual or sexually
psychological and social changes, as distinct from
attractive. This is particularly evident in cultures
the direct neurological dysfunction (primary sexual
where desirability is associated with beauty, fitness
problems) and the symptoms of MS (secondary
and health. Sexual feelings and sexual activity are
sexual problems).
not just for those who are young and able-bodied,yet this is the message continually transmitted by the
Whilst MS is not a disease of the whole person, it can
overwhelm and challenge the perception of "self" withnegative outcomes in relation to sexuality and sexual
Increasing disability can bring with it changes in
functioning. People with MS can find it difficult to see
domestic routines, reduction or cessation of
themselves as being "sexual", having sexual thoughts,
employment and reduced social interaction. This
desires and needs whilst at the same time identifying
can be very distressing for those who have seen
with the role of a person with a chronic illness.
their primary role as the wage earner or thehomemaker, for example. Disability can also lead
Individuals see themselves as complete persons in
to dependency on others for personal care. If
terms of their roles within families, friendship circles,
the partner provides this care it can be very
sporting clubs, activities and occupations. Any
difficult to separate the role of carer from that of
feelings of loss of control over events or unplanned
intimate lover. Visiting carers, nursing and
changes because of MS can affect one's confid-
domestic services intruding into the home can
ence and self-esteem and alter the dynamics of
leave people with MS feeling exposed in all
relationships, especially close and intimate ones.
areas of their life, with little private time.
MS in focus Issue 6 • 2005
DRUGS COMMONLY USED IN MS
THAT AFFECT SEXUAL FUNCTIONING
Although changes in sexual desire, performance and satisfaction often occur as a result of
MS, they may also be a consequence of some medications. (Currently, the vast majority of
the side-effects listed below are noted by manufacturers to be "infrequent" or "rare".)
Drug effect on sexual function
• Decreased libido
• Uncontrollable laughing or crying
• Delayed or absent ejaculation
• Inability to achieve orgasm (known as
• Persisting, painful erection of the penis
occurring without sexual stimulation (known as
Anyone experiencing this should seek medical
help immediately
• Menstrual irregularities
• Secretion of breast milk
(known as hyperprolactinaemia or
• Decreased libido
• Delayed or absent ejaculation
• Decreased libido
• Inability to achieve orgasm
• Menstrual irregularities
• Enlarged or painful breasts
• Irritation of the vaginal lining (vaginitis)
• Inflammation of the head of the penis and
• Secretion of breast milk
• Decreased libido
• Delayed or absent ejaculation
• Inability to achieve orgasm
• Secretion of breast milk
• Decreased libido
• Delayed or absent ejaculation
• Inability to achieve orgasm
MS in focus Issue 6 • 2005
Dealing with the impact of MS and symptoms can
relating to problems of sexuality from health
leave one neglecting the emotional and
professionals. Whilst bringing up the topic can be
psychological aspects of life in general. Simply
difficult and embarrassing for people with MS, this
attending to the physical needs of life's daily
can also be so for some doctors and health
activities can leave little time or energy for emotional
professionals. It is important to find an MS
contemplation and intimate relationships. This is
healthcare provider with whom one feels
particularly evident if fatigue is experienced as a
comfortable, or seek a referral to someone
symptom of the MS.
specialising in this area. Going together, and withpre-written questions, can be helpful and provide
It is important to remember that people with MS
the focus for initial consultation.
are not isolated and living in a vacuum; theirworries and concerns affect others. Conflict can
For health professionals the key to managing
become apparent in established relationships if
tertiary sexual problems in MS is firstly to identify
these factors are not recognised and addressed
what issues are having a negative impact on the
with ongoing and honest communication. Not
well-being and sexuality of the individual. This
uncommonly, resulting misunderstanding,
includes identification of primary and secondary
resentment and feelings of rejection by the partner
sexual problems, as well as the psychosocial
occur as they see MS becoming the dominant
factors and their complex interaction. Of prime
importance is to recognise the person with MS asa whole person in the context of lifestyle, values,
Management of tertiary sexual problems
roles, desires and relationships. Management
People with MS who experience problems with
depends on frank and open communication about
sexuality need to allow themselves time to assess
sexual issues. Treatment of any underlying
their overall situation and to feel confident about
depression and anxiety may require medication
communicating their difficulties to those close to
and psychological counselling and the provision of
them. Whilst this is not always easy, literature on MS
ongoing monitoring and support.
and sexuality can provide useful information andhelp transcend feelings of isolation and uniqueness.
Counselling can help individuals to explore feelings
There is also information on treatments and sexual
and facilitate discussion in a respectful and
aids that are available. Such information can be
professional way. Negative emotions such as guilt,
useful for partners to read and discuss together.
anger and resentment can be identified, seen in
Deciding on a time and a peaceful setting to talk
context, and worked through, in a non-judgemental
about problems of sexuality helps to create an
environment. Topics perhaps seen as too
atmosphere of mutual commitment. It is important to
embarrassing to discuss alone, can be discussed in
be gentle and express feelings without blame or
an open and supportive atmosphere. Strategies for
accusation. People with MS and their partners
improving the situation, or adopting new ways of
should explore the areas of concern slowly, listen to
considering and developing sexuality, can be
each other carefully, as frequently
misunderstandings and resentment are the result ofpoor or no communication, and respect each other's
Sexuality is an important aspect of human life
opinions. It is important to remember that sexuality is
and must not be neglected when considering
not just about physical intercourse. Sexual pleasure
the impact of MS on an individual. Increasing
can be gained, and given, by creating special times,
awareness and acknowledgement of the
places and rituals. This takes time, effort and
effects of MS on sexuality have greatly
improved the management and treatmentoptions available for people with MS
It may also be of benefit to seek further help
experiencing difficulties in this area.

MS in focus Issue 6 • 2005
TALKING ABOUT INTIMACY AND SEXUALITY IN THE HEALTHCARE SETTING
Sexual dysfunction often accompanies MS and
FOR HEALTHCARE PROFESSIONALS
may significantly affect the intimate relationships
• Silence on the subject of sexual problems does
and quality of life of people with MS and their
not mean that they do not exist.
• Set the example of how intimacy and sexuality
should be discussed: openly and without
Discussion of intimacy and sexuality is very
important but can be difficult for both people with
• If you are not comfortable discussing this topic, it
MS and healthcare professionals. Often they avoid
is important to seek assistance in order to feel
bringing up the subject of sexuality. This may be
due to personal discomfort, lack of professional
• Make questions about intimacy and sexuality part
training in the area, or a fear of being overly
of every interview since symptoms and problems
intrusive. On the other hand, intimacy and sexuality
may change. The individual may become more
are difficult subjects for the person with MS as well.
comfortable to discuss them over time.
This may be because one is unaware that the
• Often providing basic MS information that relates
problem could be related to the disease,
to sexuality can be helpful. For example: that
embarrassment, fear of being judged or due to
sexual problems are common in MS, part of the
cultural barriers.
disease symptoms, can occur together withurinary problems, etc.
Below are key issues to bear in mind, in order to
• Obtain written material to offer to people with MS
discuss this important topic effectively while
and their partners.
minimising feelings of anxiety and embarrassment
• Become familiar with the referral process for
as much as possible.
people with MS needing information on sexuality,even though it may not be part of your regular
FOR PEOPLE WITH MS
• An unsatisfactory intimate and sexual life does
not have to be part of having MS.
• There are no rules for whose "job" it is to discuss
sexual problems, so talk to the healthcareprofessional with whom you feel mostcomfortable.
• You may be experiencing a problem for which
there is a solution.
• Do not wait until you reach a crisis to discuss
• Open communication with your partner is vital.
• Once the discussion has been initiated, write
down questions between visits so as not to forget
"In education courses for nurses newly working
with people with MS, role-playing provides the
• Keep an updated list of medications to review
opportunity for them to develop a personal
during each visit, since a number of medications
approach to discussing sexuality and intimacy
can negatively influence sexual functioning.
and helps them to become more comfortable
• Ask your healthcare provider for written material
with the topic." Roberta Litta, Dir. Professional
that you can read on your own and discuss later, if
Education, Italian MS Society
MS in focus Issue 6 • 2005
WHERE TO LOOK FOR ADVICE AND REFERRALS
• Health professionals
• Family planning centres
A number of discreet catalogue services are available
• Disability information advisors
that sell sexually oriented materials and promise
• Community gay rights organizations
anonymity. Their products may be helpful to both
• Newsletters – for example ABLED! (Active
disabled and non-disabled people. Some include:
Beautiful Loving Exquisite Disabled Woman).
Special Edition Catalog for Disabled People. A
Quarterly newsletter. Focuses on body image,
catalogue of sexual aids, books, resources, and
sexuality, family concerns, and other issues relevant
information. $4.00 each. Xandria Collection, P.O.
to women living with disabilities. To subscribe, send
Box 31039, San Francisco, CA 94131. Tel: 800-
a donation ($10.00/year suggested) to ABLED
Publications, 12211 Fondren, Suite 703, Houston,
Good Vibrations provides a mail-order and
TX 77035. Tel: 713-726-1132. Fax: 713-726-
Internet catalogue of sexual aids, books and
8006. Web site: http://abledwomen.org.
videos. Good Vibrations, 938 Howard Street,Suite 101, San Francisco, CA 94103. Tel: 800-
• Books
Sexuality and Multiple Sclerosis by MichaelBarrett. MS Society of Canada, 1991 (available
• Websites
in different languages).
The Sexual Health Network's web page has
Enabling Romance: A Guide to Love, Sex, and
information on sexuality for those with disabilities
Relationships for People with Disabilities by
and illnesses. It also provides links to other
Ken Kroll and Erica Levy Klein, No Limits
resources and offers live broadcasts. It has an
archive of mainly educational books and videos
The Joy of Solo Sex by Dr Harold Litten, Factor
Press, Paperback, 1996.
The Ann Summers web page has a catalogue of
Sex for One: The Joy of Self Loving by Betty
adult sex aids, books and videos
Dodson, Three Rivers Press, 1996.
www.annsummers.comThe youtopia web page has a catalogue of adult
• Research help
sex aids, books, DVDs, clothing and accessories
Sexuality Information and Education Council of the
United States (SIECUS) provides a bibliography of
The Sinclair Intimacy Institute has a catalogue of
print and audiovisual materials related to sexuality
adult sex education videos and DVDs
and disability for $3.00 Write: SIECUS, 130 West
42nd Street, Suite 350, New York, NY 10036. Tel:212-819-9770. The bibliography is also available
• Other resources
free on the Web at www.siecus.org.
The Multiple Sclerosis Intimacy and SexualityQuestionnaire-19 is a 19-item self-report
• Journals
instrument that measures primary, secondary,
Sexuality and Disability is a journal that
and tertiary sexual dysfunction in MS. It is used
publishes scholarly articles on rehabilitation,
to assess these aspects of sexuality, and can be
disability, and sexuality. It also publishes
utilized to educate healthcare providers about
guidelines for professional clinical practice, case
which aspects of sexuality require attention.
studies, and information for consumers. Kluwer
Many MS societies have advisors, toll-free lines,
Academic/Human Sciences Press, Inc., 233
publications and groups for specific sexual
Spring Street, New York, N.Y. 10013-1578 USA.
orientations (for example GLAMS in the UK and
LeHoMS in Norway).
MS in focus Issue 6 • 2005
Your questions answered
Readers of MS in focus pose questions to the Editor, Michele Messmer Uccelli.
Q. Excessive oral secretions (saliva) make
is. This means that the opportunities to
kissing unpleasant and unromantic for
spend intimate time together are very
both. Kissing is a cornerstone to intimacy
irregular and almost non-existent. I have
and sexual activity. I find this a real
always initiated sex and I'm sure that my
problem. While excessive saliva may not
husband feels that this should still be the
be a major issue itself, it adversely affects
case. I would like to share so much more,
intimacy and sexual activity. I would love
such as touching, talking and sharing.
to find a solution to this problem. Regards,
How can I let him know that I'm not just a
"medical problem", and let him see me as
a person who still needs a little titillation
A. Increased salivary flow, also known as
and excitement?
sialorrhea or ptyalism, has not been reported as a
Thanks, BA, Australia
symptom of MS. When excessive salivation isseen, it is usually related to swallowing difficulty,
A. It is important to separate the MS from the
causing some pooling of saliva in the mouth.
rest of the person. It sounds as if you already
Some medications can induce sialorrhea, so you
know this though. It is also important that the
may want to discuss any medications you are
other person is aware of your feelings. This is
taking with your physician to understand if one of
only accomplished through honest discussion.
them may be causing you to produce excessive
MS may require couples to revise their usual
saliva. It may also be a problem related to
ways of approaching sex and intimacy (in your
another medical condition. Having MS does not,
particular case you may not always be the
unfortunately, protect people from other
"initiator"). It is also important to agree, as a
illnesses. For this reason, it is important to
couple, that intimacy is not about intercourse
consult your primary care physician regarding
alone, but, as you mentioned, touching, talking
Q. I have heard that Viagra can help
What might happen in a couple is that one
women with sexual problems. Is it true?
member believes that, for the other person,
Thank you, A.
intercourse is the ultimate goal of intimacy. Butwhen it is discovered that this isn't the case,
A. Sildenafil (ViagraTM) is used in the treatment
both people feel less under pressure and they
of primary sexual dysfunction in men, particularly
are freer to talk about other ways of being
erectile dysfunction. When studied in females
with MS, sildenafil was not found to be useful,and so is not indicated for treating sexual
Finally, there are a lot of strategies on how
dysfunction in women.
fatigue can be managed so that it does notinterfere with sexual expression. See Issue 1 of
Q. I am tired nearly all the time, but when
MS in Focus (January 2003) on Fatigue for
I'm feeling less tired, my husband usually

MS in focus Issue 6 • 2005
Interview with
Rolande Cutner
Rolande Cutner is a successful, international lawyer in Paris and New York, a very
active member of the board of the French MS society "Ligue Francaise Contre la
Sclerose en Plaques", and the French representative on the People with MS
International Committee. Rolande also has primary progressive MS.
When were you diagnosed with MS?
In April 1992, with primary progressive MS, but the
first symptoms around 1986.
Were you in a relationship/married at that
time with children etc?
I did not have children. I was divorced and dating a lot.
Do you think that MS influences your
relationship with (potential) partners?
Absolutely, yes. Who wants to be stuck with a woman
who might become paralysed down the road?
Do you feel that your self-image or self-
esteem, as a woman/partner/sexual being
has changed due to MS?
Yes. During the period when I did not know what
was wrong with me and after being diagnosed, I
tried, unsuccessfully, to hide my condition. My self-
image and my self-esteem as a woman were
damaged as long as I tried to hide the diagnosis.
When I accepted the fact that I had MS, and when I
decided that I had to fight MS, I felt better and that
fact immediately improved my relationship with
men.
Rolande Cutner

MS in focus Issue 6 • 2005
Do you feel that others (e.g. partner,
healthcare professionals) see you
differently in terms of your role as a
woman, partner and sexual being,
because you have MS?
With a diagnosis of MS, people do not see youas a woman anymore, a woman who could goto bed, make love, and participate in sexualactivity. It is your responsibility to show othersthat you are still a woman and still a humanbeing with sexual desire, who wants toparticipate in sexual activity. You must takecharge of your sexual life – be a fun and sexywoman – even with MS, and perhaps evenmore so than before.
In your opinion/experience, do you feel
The Norwegian MS Society has a number of
that people with MS may have limited
members who are gay men and lesbians. Via an
opportunities to express themselves
article in "MS matters", Issue 47, 2003, the Society
sexually or to participate in relationships?
learned that the MS Society of Great Britain andNorthern Ireland had created a support group for gay
People with MS do not have to have limited
and lesbians affected by MS: "GLAMS". We thought
opportunities to participate in relationships. If you
this could be an interesting idea for our organisation
are caring, loving and giving, as well as a
in Norway. The idea was presented to the Board of
beautiful person, you can connect. It's important
the Norwegian MS Society, and received a very
to keep in mind that MS is not an excuse to sit
positive response. The first challenge was to find
around in flannel pyjamas, hair rollers and no
people interested in taking part in the support group.
make-up. The secret is taking control. In
Since only a few people responded to an article in our
searching out ways to attract a partner, you have
Society's newsletter, we contacted a magazine for
to change how you thought about yourself
gay people in Norway and asked them to publish an
before MS. You must reach out and try to
article about our initiative, and in February 2004, a
establish relationships.
two-page article was published. The article featured awoman with MS, the Norwegian MS Society and the
Have you made changes to your life-
aims of the new support group. This generated
style/way of thinking in order to maintain
greater interest and we heard from more people who
or enhance intimacy and sexuality since
wanted to participate.
being diagnosed with MS?
The Norwegian MS Society arranged the first
Yes, I made a lot of adjustments. I became
meeting for the support group in April 2004. The
unpretentious and generous and I am not afraid
meeting was held in a restaurant, and six people
of rejection anymore. And the level of what I am
attended. Last year we organised four meetings and
willing to give up for love is much greater. Now, I
membership has increased to 12 (two men and ten
would even sacrifice my fabulous job to be with
women). Finding a name for the network was simple:
the man I love if I were asked to. I think having
LeHoMS (Le (lesbian) – Ho (homosexual) – MS).
MS encourages you to make extraordinary
At the first meeting, we discussed why the creation of
changes in your life.
the group was important. Some people outside the
MS in focus Issue 6 • 2005
MS Society of Norway:
Support group for
lesbians and gay men
with multiple sclerosis
By Turid Hesselberg, Social Worker, Norwegian MS Society
group could not understand why we wanted to create
• Many people face the double stigma of being
it. Although the acceptance of homosexuality has
disabled and gay or lesbian.
improved in recent years, there are still a number ofsceptics. Since 1993, gay men and lesbians have
• Many gay men and lesbians with MS and other
been able to formalise their relationships legally in
impairments experience loneliness and social
Norway, but it is evident that some people are afraid
of diversity and may have irrational feelings.
Nevertheless, the group grew in strength and
• Negative attitudes of health professionals create
An article published in Norway in 2001 about
Members of LeHoMS agree that it is positive to
disabled and gay men and lesbians brought up
share these joint concerns. It is not necessary to
challenges for LeHoMS. It motivated the members of
talk about being gay, since this is one of the criteria
LeHoMS to formulate a list of arguments to support
for participation. This gives members the
the importance of a network that meets the diverse
opportunity to talk about MS and life without
needs of gay men and lesbians with MS. They are
sexuality as a predominating theme.
The group has a number of initiatives in the
• Physical impairment and fatigue make it difficult for
planning phase, including a brochure and seminars.
people with MS to go to public meeting places such
The hope is to plan a meeting with the GLAMS
as bars, clubs and restaurants.
group in England in the future so that we cancreate an international exchange of experience
• Often, typical meeting places are inaccessible for
people using wheelchairs.
LeHoMS would be interested in hearing from
• Access limitations make it difficult to initiate and
groups in other countries, or from individuals who
maintain friendships and intimate relationships.
are interested in starting a group in their owncountry. Contact Turid Hesselberg, tel +47 2296
• Negative feelings about one's own body image are
3586 Wednesdays and Fridays, or by email:
a barrier to meeting new people.
MS in focus Issue 6 • 2005
Results of the MSIF online
survey on relationships,
intimacy, sexuality
Responses to an online survey on the MSIF website (www.msif.org)
have revealed what some of our online readers think about sexuality
and MS. Three hundred and sixty-six people with MS responded, of
which 87 per cent currently have a sexual partner.
This is what we learned:
The results of the study confirm that for peoplewith MS, disease-related issues, such as
Impact of MS on the relationship
symptoms, have a relevant impact on relationships.
The results show that MS, or specific issues related
Intimate problems are common and open
to MS, have a significant influence on relationships.
communication is crucial to addressing sexuality
The box provides details on these MS-related
and intimacy concerns, although not many people
issues. Fatigue, loss of libido and altered
seek professional help or benefit from treatment
sensations were the most commonly reported
for specific problems.
factors influencing relationships.
MS-related issues influencing relationships
Changes in lifestyle/way of thinking
Over half of the respondents have made changes
to their lifestyle or their way of thinking to maintain
Altered sensations
or enhance intimacy and sexuality. The study
Feeling less confident
confirms that sexual difficulties are crucial in
determining the way a person feels about him or
Feeling less attractive
herself as a man or woman, with almost two-thirds
Sensory disturbances
of respondents reporting that sexual issues have
Erectile problems
an impact on their view of themselves.
Decreased vaginal
Too many other problems
Two-thirds of respondents experienced difficulty in
to think about sex
communicating with others (either a partner,
Bladder or bowel problems
healthcare professionals or others) on MS-related
Feeling socially isolated
sexual difficulties.
Poor concentration
Role changes/conflicts
The survey revealed that fewer than a third of the
Managing catheters
respondents have benefited from counselling,
Cultural values create
advice and therapy, and almost two-thirds have had
a negative experience with treatment for specific
MS in focus Issue 6 • 2005
Quality of Life
Principles By Paul Rompani, MSIF
The Principles to Promote the Quality of Life ofPeople with Multiple Sclerosis (Quality of LifePrinciples) is a new advocacy tool developed tohelp people affected by MS (eg MS societiesand organisations). The aim of the Principles isto improve the quality of life (QOL) of peoplewith MS.
The Principles are evidence-based internationalstandards that focus on the common issues thataffect the QOL of people with MS, for instancethe distress and disability caused by the manysymptoms of the disease, the inability in somecases to live at home, the loss of paidemployment, the loss of mobility, and the lack ofco-ordination between medical and social care.
As a result, they are not linked to particulartypes or stages of MS.
The Principles are designed to be used by anyindividual, group or organisation involved inmaking decisions that will affect the QOL ofpeople with MS. They will guide thedevelopment and evaluation of existing andproposed services and programmes, irrespectiveof the provider, and will help to advocate forimprovements. Users include internationalorganisations, governments, non-profit and for-profit health, social care and continuing care
The development of the Principles was based on
service providers, employers, national MS
a series of interviews, a literature review, the
societies, researchers, businesses and, most
clinical, programmatic, and research experience
importantly, people affected by MS.
of the authors, and review by a Work Group anda technical Oversight Group organised by MSIF.
MSIF is preparing three practical guides
The interviews were conducted with a range of
describing how the Principles can support MS
international MS and QOL experts, MS clinical
Society programme planning, sharing best
providers and people with MS, many of whom
practice and influencing public policy.
were from the UK.
MS in focus Issue 6 • 2005
Book review: In sickness and in health:
convincing and complete. While there is no
Sex, love and chronic illness
"professional" opinion in the book, the diversity of
By Lucille Carlton
the contributions from real experience makes this
Review by Cristina Gómez Ortiz,
omission irrelevant.
AEDEM, Spain
The book is focused on people with a chronic
illness, single or living in a couple. I would say that
certain chapters of the book are pertinent for the
general public, since sexuality and chronic illness
inspire creativity
are topics that often arouse fear, and a better
understanding of people's experiences can
benefit everyone. I think it is one of the best
books that has been written for people with MS
because it speaks openly about a topic that
creates anxiety and apprehension for many, but
chronic illness. It
which is relevant to all people living with a chronic
the female pointof view since the
The writer's style is simple and clear, which
makes it very easy to read. The book had an
important influence on me and I am sure that it
could be useful to others.
disease patient. Lucille Carlton was married foralmost 50 years and had a very good marriage,
Publisher: Dell, 1997, ISBN: 0440508053,
maintaining sexual intimacy through two chronic
Price US$9.50
illnesses. Her husband cared for her when shewas debilitated for many years by a rare skin
Website review: The Sexual Health
disease, and she cared for him through 16 years
of Parkinson's disease. The information in the
Review by Tim Miller, Italy
book is, therefore, applicable to many peopledealing with various chronic illnesses.
The Sexual Health Network website is anAmerican commercial website covering a broad
The author gives examples of daily situations andfeelings that people affected by chronic illnessmay experience in relation to intimacy andsexuality. She also talks about her ownexperiences in her marriage, as well as theexperience she gained from working as aspeaker and a columnist for the NationalParkinson Foundation.
The ideas in this book are supplemented by theopinions and experiences of people with chronicdisease and their partners, which help to make it
MS in focus Issue 6 • 2005
range of illnesses and in the context of sexuality.
As a point of access it can be helpful to thoseinterested in aspects of MS and sexuality, withsome pages specifically tailored to MS.
The site's mission-statement clearly describes itsscope and purpose. It is an English-languagewebsite, access is free, no special software isrequired to view the information, and navigation isstraightforward, although it would be helped bythe inclusion of a site map. Information on thesite's experts and their backgrounds are included,as well their photographs. Contributions to thesite are fairly recent, although the frequency ofupdates is not clear. It is intended as a starting
issues are covered with up-to-date information,
point from which to move on to counsellors and
and the website is useful both for people with MS
therapists and to other sites through web links,
and specialists.
banners and pop-ups (see review below).
The audio/video sections are informative and can
As a gateway to further information it contains
improve knowledge on management in clinical
links through to the Healthology website from
care for physicians, and also for other MS
where audio and video clips can be downloaded,
professionals. Some of the interactive options
as well as related texts.
include courses that present various topics. Thisis a useful approach to get a quick readout about
It can be useful and an immediately available
the state-of-the art on different MS issues. The
point of information. The validity of the help
contributions are from opinion-leaders in the MS
available and the links contained are a matter for
field, whose knowledge and expertise is
the visitor to judge, as with all Internet resources.
internationally acknowledged, lending a high level
It is a valuable starting point.
of authority to the site content.
While the site is very interactive, it is not possibleto print some of the sections. A caveat regardingthis site is that many sections need an audio
Website review: Healthology
system support programme (and audio speakers)
Review by Claudio Solaro, MD, Department of
that may not be easily accessible to all users.
Neurology, Micone Hospital, Genoa, Italy
Moreover, the website is based on video sectionsthat are not manageable in a simple way by
This website is not MS-specific, although there is
an MS section. It also covers neurologicaldiseases and symptoms such as headache and
Overall the site is user-friendly and very
dementia and non-neurological diseases such as
informative. I would recommend it to healthcare
tumours. Access to all parts of the site is free-of-
professionals and anyone interested in learning
more about MS and its treatment andmanagement.
With regard to the MS section, the site design isuser-friendly and is easy to navigate, both within
the main sections and between links. Many MS
MS in focus
+44 (0)207 620 1911
+44(0)207 620 1922
MSIF is a non-profit charitableorganization 501(c)(3) IRC chartered inthe State of Delaware, USA, in 1967. UKregistered charity 1105321.
Subscriptions
The Multiple Sclerosis International Federation
produces MS in focus twice a year. With an
international cross-cultural board, easily
accessible language and free subscription,
MS in focus is available to all those affected
by MS worldwide. To subscribe, log on to
www.msif.org
With many thanks
MSIF would like to thank Serono for their
unrestricted grant which made the production of
MS in focus possible
A new chapter has been added to
• patient appropriateness for and readiness to initiate
the International MS Nurse Care
Plan – a comprehensive and
• treatment efficacy
practical guide to the specialised
• monitoring and management of possible side effects
field of MS nursing.
• benefit-to-risk profile
• the patient's physical, cognitive, and psychosocial status
A group of world-renowned MSnurses convened in October 2004
Since nurses are the main healthcare professionals to
to finalise it and ensure that it was
have day-to-day contact with patients, they play a pivotal
developed in accordance with
role in identifying and overcoming problems and, thereby,
continuing medical education (CME)
help ensure optimal treatment outcomes. The new
regulations and free of commercial bias.
chapter outlines an evidence-based nursing approachthat is designed to guide and assist nurses through this
This new chapter is focused on Treatment Optimisation.
demanding and long-term process of treatment
The introduction of the newer disease-modifying
therapies have heralded a new era in the management ofrelapsing MS. However, ensuring optimal medical and
Maria Grazia Calì
health outcomes for patients using these therapies
Serono Symposia International
depends on various factors, including:
Source: http://www.e-cooline.de/assets/Documents/MS-in-focus-6-Intimacy-and-sexuality-English.pdf
The effect of subclinical ketosis in early lactation on reproductive performance of postpartum dairy cows
J. Dairy Sci. 90:2788–2796doi:10.3168/jds.2006-560© American Dairy Science Association, 2007. The Effect of Subclinical Ketosis in Early Lactation on ReproductivePerformance of Postpartum Dairy Cows R. B. Walsh,*1 J. S. Walton,† D. F. Kelton,* S. J. LeBlanc,* K. E. Leslie,* and T. F. Duffield**Department of Population Medicine, and†Department of Animal and Poultry Science, University of Guelph, Ontario, Canada, N1G 2W1
Regulation of pharmaceutical markets in germany: improving efficiency and controlling expenditures
Managing pharmaceutical regulation in Germany: overview and economic assessment Jonas Schreyögg, Klaus-Dirk Henke, Reinhard Busse Abstract Rising costs in pharmaceutical expenditure have become a major concern for policy makers in Germany over the last years. Therefore the pharmaceutical market in Germany has been increasingly targeted by different kinds of regulations, focussing