Rbccv.org


Braz J Cardiovasc Surg 2016;31(2):106-14
Clopidogrel use After Myocardial Revascularization:
Prevalence, Predictors, and One-Year Survival Rate
Paulo Roberto L. Prates1,2, MD; Judson B. Williams3,4, MD; Rajendra H. Mehta4,5, MD, MSc; Susanna R. Stevens5, MSc; Laine Thomas5, PhD; Peter K. Smith3, MD; L. Kristin Newby4,5, MD; Renato A. K. Kalil1,2, MD, PhD; John H. Alexander4,5, MD, MHS; Renato D. Lopes4,5, MD, PhD
Abstract
Introduction: Antiplatelet therapy after coronary artery
arterial disease and cerebrovascular disease. Patients who
bypass graft (CABG) has been used. Little is known about the
received aspirin during hospitalization were less likely to receive
predictors and efficacy of clopidogrel in this scenario.
clopidogrel at discharge (P≤0.0001). Clopidogrel was associated
Objective: Identify predictors of clopidogrel following CABG.
with similar 1-year mortality compared with those who did not
Methods: We evaluated 5404 patients who underwent
use clopidogrel (4.4% vs. 4.5%, P=0.72). There was, however,
CABG between 2000 and 2009 at Duke University Medical
an interaction between the use of cardiopulmonary bypass and
Center. We excluded patients undergoing concomitant valve
clopidogrel, with lower 1-year mortality in patients undergoing
surgery, those who had postoperative bleeding or death before
off-pump CABG who received clopidogrel, but not those
discharge. Postoperative clopidogrel was left to the discretion
undergoing conventional CABG (2.6% vs 5.6%, P Interaction = 0.032).
of the attending physician. Adjusted risk for 1-year mortality
Conclusion: Clopidogrel was used in nearly one-fifth of
was compared between patients receiving and not receiving
patients after CABG. Its use was not associated with lower
clopidogrel during hospitalization after undergoing CABG.
mortality after 1 year in general, but lower mortality rate in those
Results: At hospital discharge, 931 (17.2%) patients were
undergoing off-pump CABG. Randomized clinical trials are needed
receiving clopidogrel. Comparing patients not receiving
to determine the benefit of routine use of clopidogrel in CABG.
clopidogrel at discharge, users had more comorbidities,
Keywords: Myocardial Revascularization. Coronary Artery
including hyperlipidemia, hypertension, heart failure, peripheral
Bypass. Blood Platelets.
Abbreviations, acronyms & symbols
Antiplatelet therapy is beneficial in secondary prevention
= Coronary artery bypass graft
following coronary artery bypass graft (CABG) surgery; however,
= Confidence interval
there is no consensus about when to initiate therapy, how to
= Clopidogrel in unstable angina to prevent
dose, or the optimal combination of agents[1-4]. Clopidogrel also
recurrent ischemic Events
reduces ischemic events and mortality in patients with coronary and peripheral arterial disease[5-8]. While the use of aspirin
= Hazard risk
after CABG surgery is widespread[2,4,9,10], clopidogrel, the most
= Percutaneous coronary intervention
commonly used P2Y inhibitor, in addition to aspirin, has been
PREVENT IV
= Project of Ex-vivo Vein graft ENgineering via
used less often than aspirin alone[11].
Transfection IV
Although it has been shown that antiplatelet therapy
improves the patency of venous grafts[2,4,12], little is known about
1Department of Cardiovascular Surgery, Instituto de Cardiologia–Fundação Uni-
acquisition, analysis, and interpretation of data; preparation, review, or approval
versitária de Cardiologia, Porto Alegre, RS, Brazil.
of the manuscript.
2Clinical Research Center- Instituto de Cardiologia–Fundação Universitária de Car-diologia, Porto Alegre, RS, Brazil.
Drs. Williams, Smith, and Alexander are supported in part by grant U01-HL088953
3Department of Surgery, Division of Cardiovascular and Thoracic Surgery, Duke
from the National Institutes of Health Cardiothoracic Surgical Trials Network.
University Medical Center, Durham, NC.
None of the other authors have any conflict of interest to report related to this study.
4Department of Medicine, Division of Cardiology, Duke University Medical Center, Durham, NC.
Correspondence Address:
5Duke Clinical Research Institute, Durham, NC.
Renato D. Lopes Duke Clinical Research Institute, Box 3850, 2400 Pratt Street, Room 0311 Terrace
This study was carried out at the Instituto de Cardiologia do Rio Grande do Sul -
Level, Durham, NC 27705.
Fundação Universitária de Cardiologia, Porto Alegre, RS, Brazil.
This work was supported by the Duke Clinical Research Institute (DCRI). The
Article received on December 8th, 2015
DCRI provided funding for the design, conception, and conduct of the study;
Article accepted on March 8th, 2016
Brazilian Journal of Cardiovascular Surgery
Prates PRL, et al. - Clopidogrel use After Myocardial Revascularization
Braz J Cardiovasc Surg 2016;31(2):106-14
which patients are receiving clopidogrel after CABG surgery or
for categorical variables. Baseline and in-hospital patient
about its association with patient outcomes. In this large single-
characteristics for those who did and did not receive in-hospital
center study we described the clinical and surgical characteristics
clopidogrel following CABG surgery were compared using
and predictors of patients receiving clopidogrel following CABG
the Wilcoxon rank sum test for continuous variables and chi-
surgery, determined the rates of clopidogrel use after 1 year, and
square or Fisher's exact tests for categorical variables. Because
compared the 1-year risk-adjusted mortality in patients receiving
of recent findings demonstrating differences between patients
and not receiving clopidogrel.
undergoing on- and off-pump CABG surgery[13], unadjusted Kaplan-Meier rates for 1-year survival are shown for the 4-level
stratification of patients who did and did not receive clopidogrel and had on-pump versus off-pump CABG surgery.
Multivariable logistic regression was used to determine the
We evaluated 6588 patients undergoing CABG surgery
association between baseline and in-hospital demographics and
between 2000 and 2007 at Duke University Medical Center
clinical factors with in-hospital clopidogrel use following CABG
(Durham, NC, USA). A total of 815 patients were excluded for
surgery. All variables as well as their interactions with on- and
concomitant valve surgery, 177 were excluded for in-hospital
off-pump CABG surgery were considered for inclusion using
reoperation for bleeding or anticoagulation complications,
backward elimination with a requirement of alpha <0.05 for
188 died prior to discharge, and 4 additional patients who had
retention (Tables 1 and 2).
undergone CABG surgery within 9 days were excluded, resulting
Cox proportional hazards analysis was performed to evaluate
in a final sample size of 5404. Patients undergoing urgent or
the association between post-CABG clopidogrel use and 1-year
elective procedures were included. This study was approved by
mortality. We adjusted for covariates identified in the PRoject of
the Duke University Health System Institutional Review Board.
Ex-vivo Vein graft ENgineering via Transfection IV (PREVENT IV)
The requirement for individual consent was waived. All patients
trial mortality model[13], developed in a similar CABG population,
undergoing surgical procedures signed an informed consent
and included the most closely related variables available in our
form according to the data collected during hospitalization
dataset. In addition, we also adjusted for aspirin use after CABG
which can be used in research.
surgery, warfarin use at discharge, on- and off-pump CABG-surgery, in-hospital cerebrovascular accident and renal failure.
Adjusted survival curves are shown for the clopidogrel effect in
On- and off-pump CABG procedures were performed during
the multivariable Cox mortality model. The model was repeated
the study period, including both urgent and elective procedures.
with the inclusion of the interaction of clopidogrel with on-
All patients were operated by the same group of surgeons that
and off-pump CABG surgery; adjusted survival curves for this
consists of 19 professionals. After median sternotomy, patients
interaction are shown.
underwent conventional CABG surgery with the use of internal
For the multivariable logistic and Cox models, continuous
mammary arteries whenever possible. When performed on
and ordinal variables were tested for linearity over the log hazard
pump CABG, standard cardiopulmonary bypass was used,
and were transformed as necessary to meet this modeling
typically with both anterograde and retrograde cold blood
assumption. The proportional hazards assumption was checked
for each variable in the mortality model and there were no deviations of concern. Statistical analyses were performed using
SAS version 9.1 (SAS Institute, Inc., Cary, NC, USA).
Discharge clopidogrel use was determined by in-hospital
medication records, that was found in the electronic medical
record, and was defined as administration at any time the day after surgery through the date of discharge. The files were
Study Population and Baseline Characteristics
accessed by the institution's research group. In addition to
Total of 5404 patients who underwent CABG surgery from
clinical data collected during patient visits, medication use
2000–2007 where evaluated. Among these patients, 931 (17.2%)
and survival were determined using self-administered mailed
received clopidogrel after CABG surgery. Patients who received
questionnaires and telephone follow-up for those who did
clopidogrel, 789 were alive with complete medication information
not return questionnaires. Deaths reported by Duke hospitals,
after 1 year and 314 (39.8%) were still taking clopidogrel. Among
the National Death Index, and the Social Security Death Index
the patients not taking clopidogrel after surgery, 8.9% (345/3868)
were used to confirm or supplement the follow-up surveys for
were taking it after 1 year. One-year mortality was related to the
mortality information. These actions were also performed by the
use of clopidogrel at any time in hospital postoperative evolution.
institution's research group. Operative mortality was defined as
The above data add information about using this medication
death occurring within 30 days of the index procedure or before
after discharge.
Patient baseline characteristics are shown in Table 1. When
compared with patients who did not receive clopidogrel, those
who did were younger and had more comorbidities including
Summary statistics were expressed as medians (25th, 75th
hyperlipidemia, hypertension, peripheral arterial disease, and
percentiles) for continuous variables and numbers (percentage)
cerebrovascular disease but less heart failure in the prior 2
Brazilian Journal of Cardiovascular Surgery
Prates PRL, et al. - Clopidogrel Use After Myocardial Revascularization
Braz J Cardiovasc Surg 2016;31(2):106-14
Table 1. Baseline characteristics according to clopidogrel use after CABG.
Age, median (25th, 75th), yrs*
Female sex, no. (%)*
White race, no. (%)
Weight, median (25th, 75th), kg
Medical history, no. (%)
Diabetes mellitus*
Chronic lung disease*
Recent MI (30 days)
Prior valve procedure
CHF within prior 2 weeks*
History of cerebrovascular disease*
History of peripheral vascular disease*
Patient currently on dialysis
Cardiogenic shock during the procedure
Presenting features
Creatinine (most recent in past 60 days), median (25th, 75th)*
GFR (most recent in past 60 days), median (25th, 75th)*
EF (most recent in past 60 days), median (25th, 75th)*
Number of vessels ≥ 50% stenosed, no. (%)
Left main disease ≥ 50%, no. (%)
Preoperative antiplatelet agents, no. (%)
Aspirin administered prior to CABG
Clopidogrel administered prior to CABG
*Included in multivariable model for mortality. CABG=coronary artery bypass grafting; CHF=congestive heart failure; EF=ejection fraction; GFR=glomerular filtration rate; MI=myocardial infarction; PCI=percutaneous coronary intervention
Brazilian Journal of Cardiovascular Surgery
Prates PRL, et al. - Clopidogrel Use After Myocardial Revascularization
Braz J Cardiovasc Surg 2016;31(2):106-14
Table 2. Operative and postoperative characteristics according to clopidogrel use after CABG.
Surgery type, no. (%)
Left or right IMA, no. (%)*
SVG harvested endoscopically, no. (%)*
On-pump surgery, no. (%)*
Cross-clamp time, median (25th, 75th)*
Perfusion time, median (25th, 75th)*
Number of grafts, no. (%)
Worst target artery quality, no. (%)*
Worst graft quality, no. (%)*
Type of graft, no. (%)
Left saphenous vein
Right saphenous vein
Both left & right saphenous veins
Left internal thoracic artery
Right internal thoracic artery
Both left & right internal thoracic arteries
Left radial artery
Right radial artery
Both left & right radial arteries
Length of stay, median (25th, 75th)*
Patient discharged on warfarin, no. (%)*
Aspirin after surgery and before discharge, no. (%)*
MI occurs after surgery and before discharge, no. (%)*
Cerebrovascular accident after surgery and before
discharge, no. (%)*Atrial fibrillation before discharge, no. (%)*
*Included in multivariable model for mortality. IMA=internal mammary artery; MI=myocardial infarction; SVG=saphenous vein graft
Brazilian Journal of Cardiovascular Surgery
Prates PRL, et al. - Clopidogrel Use After Myocardial Revascularization
Braz J Cardiovasc Surg 2016;31(2):106-14
Table 3. Multivariable associations with clopidogrel use after CABG (N=4887).
Worst target artery quality, OR for 1 category increase
1.70 (1.50, 1.94)
Left or right IMA
0.55 (0.42, 0.72)
Worst graft quality, OR for 1 category increase
1.36 (1.17, 1.58)
Age, OR for 10-year increase
0.86 (0.79, 0.93)
Left main disease
1.40 (1.16, 1.69)
MI before discharge
10.85 (2.75, 42.82)
Surgery type (reference is elective)
1.33 (0.88, 1.99)
1.52 (1.21, 1.92)
Ejection fraction, OR for 10% increase
Linear spline ≥67, OR for off pump
4.10 (2.48, 6.77)
Linear spline ≥67, OR for on pump
1.75 (1.23, 2.49)
Linear spline ≤67
0.92 (0.85, 0.99)
Number of grafts, OR for off pump
1.08 (0.88, 1.32)
Number of grafts, OR for on pump
0.75 (0.66, 0.86)
Aspirin at discharge
0.46 (0.27, 0.78)
Pre-CABG clopidogrel
1.52 (1.13, 2.04)
Perfusion time, OR for 30-minute increase
1.13 (1.04, 1.24)
SVG harvested endoscopically, OR for off pump
4.66 (1.33, 16.33)
SVG harvested endoscopically, OR for on pump
0.67 (0.36, 1.26)
Congestive heart failure
0.71 (0.55, 0.91)
0.77 (0.63, 0.93)
History of hypertension
1.32 (1.05, 1.65)
1.31 (1.05, 1.63)
Cross-clamp time, OR for 30-minute increase
1.18 (1.03, 1.35)
Cerebrovascular accident before discharge, OR for off pump
0.24 (0.05, 1.16)
Cerebrovascular accident before discharge, OR for on pump
1.68 (0.96, 2.94)
Atrial fibrillation before discharge
0.76 (0.59, 0.96)
Discharge warfarin, OR for off pump
1.63 (0.60, 4.43)
Discharge warfarin, OR for on pump
0.50 (0.28, 0.90)
History of cerebrovascular disease
1.28 (1.01, 1.62)
*P value for interaction term of variable with on/off-pump. CI=confidence interval; IMA=internal mammary artery; MI=myocardial infarction; OR=odds ratio; PCI=percutaneous coronary intervention; SVG=saphenous vein graft
weeks. They were also more likely to have undergone prior
percutaneous coronary intervention (PCI) or CABG surgery. Post-
The main surgical procedure characteristics are shown in
CABG clopidogrel users were also more likely to have received
Table 2. Patients who did not receive clopidogrel more often
clopidogrel in the preoperative period. Overall, aspirin was used
underwent elective surgery (29.2% vs. 19.4%) while those
in 98.1% of patients after CABG surgery (96.7% with and 98.4%
receiving clopidogrel more often underwent urgent procedures
without clopidogrel after CABG surgery).
(65.3% vs. 74.9%). Clopidogrel users were more likely to have bad
Brazilian Journal of Cardiovascular Surgery

Prates PRL, et al. - Clopidogrel Use After Myocardial Revascularization
Braz J Cardiovasc Surg 2016;31(2):106-14
Table 4. Kaplan-Meier rates for 1-year mortality according clopidogrel use versus not stratified by off and on pump surgeries.
Off pumpNo clopidogrel, no. (%)
Clopidogrel, no. (%)
On pump*No clopidogrel, no. (%)
Clopidogrel, no. (%)
*One on-pump patient without and one on-pump patient with clopidogrel after CABG were censored before the 1-year follow-up period. These patients are not included in the alive counts after 1 year but are reflected in the Kaplan-Meier rate.
quality grafts than patients who did not receive clopidogrel. The hospital length of stay was similar among the 2 groups.
In the overall population, 4716 (87.3%) patients had left
saphenous vein grafts harvested, 1161 (21.5%) had right
saphenous vein grafts harvested, and 785 (14.5%) had saphenous vein grafts from both left and right legs harvested (Table 2). A
total of 4875 (90.2%) patients had a left internal thoracic artery graft, 188 (3.5%) had a right internal thoracic artery graft, and
123 (2.3%) had both internal thoracic artery grafts. Left radial
grafts were used in 305 (5.6%) patients, 50 (0.9%) patients had
a right radial artery graft, and 17 (0.3%) had both a right and left radial artery graft. While right saphenous vein grafts and left radial artery grafts were more commonly used in patients discharged with clopidogrel, left saphenous vein grafts and left internal thoracic artery grafts were more often used in patients
Days after hospital discharge
discharged without clopidogrel (Table 2).
Predictors of Clopidogrel Use
The predictors of clopidogrel use are shown in Table 3.
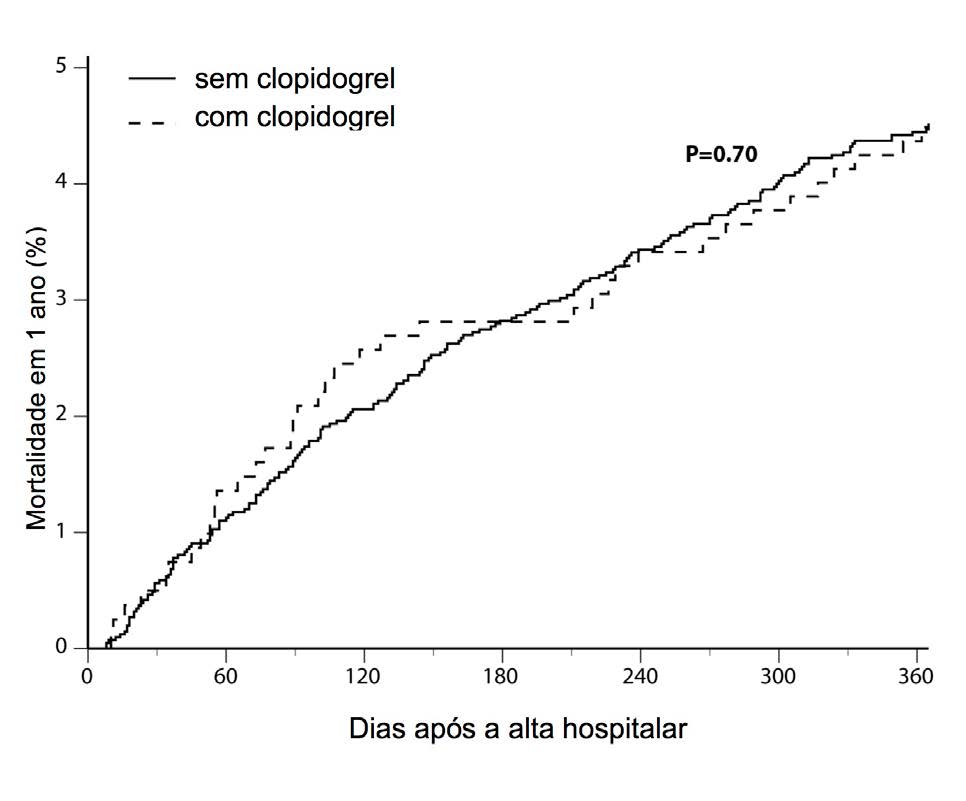
Fig. 1 – One-year mortality according to the clopidrogel use after
Patients who had worse target artery or graft quality, left main
disease, prolonged perfusion time, clopidogrel before surgery, or prior PCI were more likely to receive clopidogrel after CABG surgery. Advanced age, internal mammary artery graft, elective surgery, and aspirin use before surgery or at discharge were
associated with a lower probability of clopidogrel use following
Our study has 2 main findings. First, at Duke University
CABG surgery.
Medical Center, postoperative clopidogrel is used in almost one-fifth of the patients undergoing CABG surgery. These
patients tend to be sicker and have more comorbidities than
Clopidogrel use was associated with similar 1-year mortality
those who do not receive clopidogrel after surgery. We also
(4.7% vs. 4.5%, adjusted hazard ratio [HR] 1.08, 95% confidence
identified several key factors associated with clopidogrel use
interval [CI] 0.73–1.59; P=0.70) compared with those not using
after CABG surgery. Second, clopidogrel use was associated
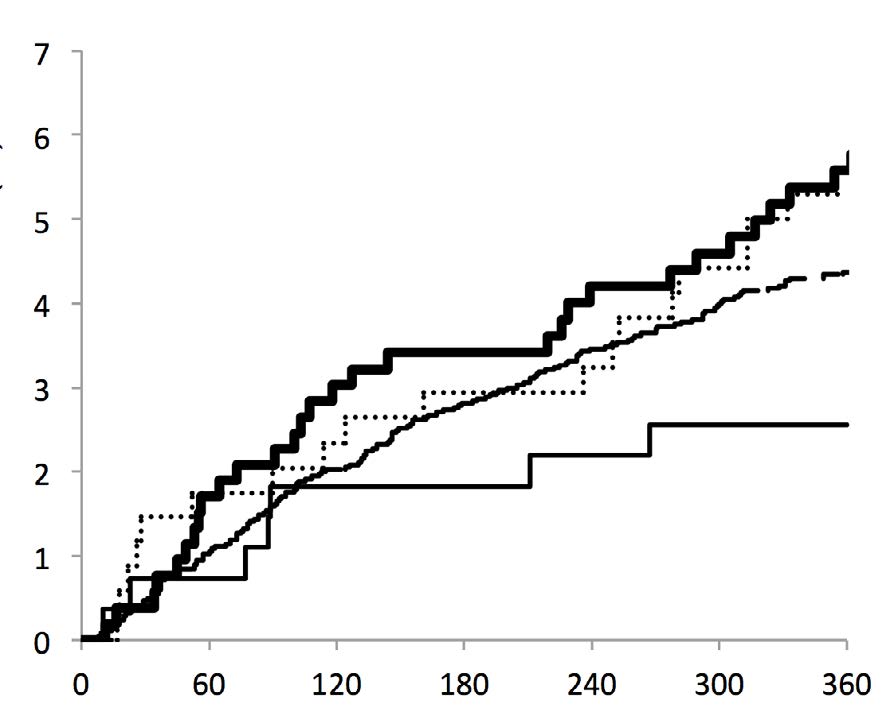
clopidogrel (Table 4, Figure 1). However, there was an interaction
with similar 1-year mortality compared with those patients not
between use of cardiopulmonary bypass and clopidogrel, with
using it. However, there was an interaction between the use
lower 1-year mortality with clopidogrel in patients undergoing
of cardiopulmonary bypass and clopidogrel, with lower 1-year
off-pump CABG surgery (adjusted HR 0.47, 95% CI 0.19–1.13), but
mortality with clopidogrel among patients undergoing off-
not in those undergoing on-pump CABG surgery (adjusted HR
pump CABG surgery and higher 1-year mortality with clopidogrel
1.35, 95% CI 0.89–2.05; P interaction=0.032) (Figure 2).
among those undergoing on-pump CABG surgery.
Brazilian Journal of Cardiovascular Surgery
Prates PRL, et al. - Clopidogrel Use After Myocardial Revascularization
Braz J Cardiovasc Surg 2016;31(2):106-14
significantly associated with less use of clopidogrel during the hospital stay. Whether the patients were treated on or off pump, it appears that clopidogrel was generally chosen for younger patients (perhaps balancing bleeding risks) with poor target artery quality, cerebrovascular disease, and previous coronary
interventions. Without randomized data on clopidogrel use
following CABG surgery, our study provides insights about potential factors associated with its use that might help physicians decide when to use clopidogrel in this clinical setting.
In a subgroup analysis from the PREVENT IV study, in which
all patients received aspirin at hospital discharge, clopidogrel use
was associated with a trend for higher rates of occluded vein grafts during 12–18 months (49% vs. 39%; adjusted odds ratio 1.26; P=0.08) and with similar composite rates of death, myocardial infarction, or revascularization (27% vs. 24%; adjusted HR 1.10;
Days after hospital discharge
P=0.38) in 5 years compared with those without it[13]. This study found a significant interaction between use of cardiopulmonary
on-pump /with clopidogrel
bypass and clopidogrel. Similarly, in our study, the administration
on-pump /without clopidogrel
of clopidogrel during the hospital stay was not associated with overall 1-year mortality in patients undergoing CABG surgery,
Fig. 2 – One-year mortality according to the clopidrogel use after
even in those cases where an emergency or urgent surgery was
on-pump and off-pump CABG.
needed. In patients undergoing off-pump surgery, we found that clopidogrel use was associated with higher 1-year survival; however, in patients undergoing on-pump surgery, clopidogrel
Previous studies have demonstrated the benefit of
use was associated with higher 1-year mortality.
antiplatelet agents, particularly aspirin, after CABG surgery,
Studies show different conclusions regarding the results
although there is no consensus on when to initiate and what
found when the techniques compared with and without
dose should be used. Moreover, these studies do not directly
cardiopulmonary bypass[21-23]. On the other hand, several
show the impact of therapy on mid- and long-term mortality[3,4,7].
investigators have indicated that off-pump CABG surgery may
There are published reports of controlled trials showing benefit
increase the risk of thrombosis due to augmented thrombotic
of different antiplatelet therapies, including aspirin alone[9,14],
activity[24,25]. There is a well-known phenomenon of thrombotic
aspirin plus dipyridamole[14-16], and aspirin plus sulfinpyrazone[17].
activity following major general surgery and it is expected after
More recent studies have demonstrated improved graft patency
major procedures[25]. In fact, Mariani et al.[25] demonstrated that
with the use of clopidogrel[7,12]. While the success of the surgical
thrombotic activity is increased in the first 24 hours after off-
procedure is most critical to the patency of a graft, understanding
pump surgery. Clopidogrel appeared to have a role in decreasing
the relationship between clopidogrel use and mortality and
clotting and protecting the patency of anastomoses. In on-
other hard clinical outcomes is critical.
pump surgery, there is a well described decrease in platelet
Clopidogrel use in patients with acute coronary syndromes
function that could bring benefits for graft patency[26,27]. This
demonstrates benefit[5,6,18]. Treatment with clopidogrel reduced
benefit does not occur in off-pump surgery where platelet
the risk of myocardial infarction and recurrent ischemia, with a
function tends to be closer to normal, leaving more room for
trend toward lower rates of cerebrovascular accident and death
benefit of an antiplatelet agent such as clopidogrel. It is known
from cardiovascular causes[5,6,19]. Antiplatelet therapy with aspirin
that extracorporeal circulation leads to a decrease in blood
has led to improvements in vein graft patency when started
coagulation activity, mainly due to consumption of factors and
early after CABG[4,7,20]. The combination of clopidogrel and aspirin
reduction of platelet activity[26]. This could have a protective
after off-pump CABG surgery was previously suggested to
impact on patients undergoing on-pump CABG surgery. In this
reduce cardiac events and mortality[12] as well as improve graft
situation, the pharmacological activity of clopidogrel may not
patency in a single-center trial of 249 patients (91.6% for aspirin
have as much of a role and this may have contributed to our
plus clopidogrel vs. 85.7% for aspirin alone; P=0.043) [7].
While it remains unknown why some patients received
In the Clopidogrel in Unstable angina to prevent Recurrent
clopidogrel and others did not, our study identified several
ischemic Events (CURE) trial, patients randomized to clopidogrel
factors associated with clopidogrel use following CABG surgery:
in addition to aspirin had a 20% reduction in cardiovascular death,
target vessel quality, graft quality, age, congestive heart failure,
myocardial infarction, or cerebrovascular accident in the 9th
cerebrovascular accident, prior myocardial infarction, prior PCI,
month in the follow-up period. Among patients who underwent
prior CABG surgery, and aspirin use at hospital discharge. The
CABG surgery, the apparent benefit of clopidogrel was tempered
strongest predictor of clopidogrel use after CABG surgery was
by a higher major bleeding rate among clopidogrel-treated
worse target artery quality. Importantly, almost every patient
patients (9.6% vs. 7.5%, respectively). Importantly, these patients
(98.1%) received aspirin after the CABG surgery and this was
were already on clopidogrel when undergoing CABG surgery
Brazilian Journal of Cardiovascular Surgery
Prates PRL, et al. - Clopidogrel Use After Myocardial Revascularization
Braz J Cardiovasc Surg 2016;31(2):106-14
and did not start clopidogrel for the first time after surgery. Based
Authors' roles & responsibilities
in large part on the CURE trial data, the current American College of Cardiology/American Heart Association/Society of Thoracic
Analysis and/or data interpretation; manuscript redaction
Surgeons guidelines recommend withholding therapy for 5
or critical review of its content; final manuscript approval
days among acute coronary syndrome patients requiring CABG
Analysis and/or data interpretation; manuscript redaction
or critical review of its content; final manuscript approval
At the present time, there are not adequate randomized
Analysis and/or data interpretation; manuscript redaction
clinical trial data to determine whether adding clopidogrel to
or critical review of its content; final manuscript approval
aspirin prevents adverse clinical outcomes (death, myocardial
Statistical analysis; manuscript redaction or critical review
infarction, cerebrovascular accident, unstable angina, or
of its content; final manuscript approval
recurrence of angina) after CABG surgery. Despite this, clopidogrel
Statistical analysis; manuscript redaction or critical review
is widely but inconsistently prescribed in patients after CABG
of its content; final manuscript approval
surgery with stable coronary disease[18], a practice supported
Analysis and/or data interpretation; manuscript redaction
primarily by subgroup analyses and observational data[12,29-31].
or critical review of its content; final manuscript approval
In our study, clopidogrel was used more often in patients with
Analysis and/or data interpretation; manuscript redaction
poor graft quality, which suggests that cardiologists and cardiac
or critical review of its content; final manuscript approval
surgeons might be using clopidogrel after CABG surgery in
RAKK Analysis and/or data interpretation; manuscript redaction
or critical review of its content; final manuscript approval
patients with worse coronary disease. While also observational, the data we present do not support a beneficial effect of dual
Conception and design study; analysis and/or data interpretation; manuscript redaction or critical review of
antiplatelet therapy following CABG surgery, although there may
its content; final manuscript approval
be some benefit in the off-pump setting.
Conception and design study; analysis and/or data interpretation; manuscript redaction or critical review of
its content; final manuscript approval
Our study has several limitations to consider. First, this is an
observational study and one cannot account for unmeasured confounders. Thus, a cause and effect relationship between clopidogrel use and mortality cannot be assessed. Second, this is a single-center study and caution should be taken when generalizing our results to other institutions or settings. Third, while target artery quality was measured, other intraoperative technical factors were not measured and may play a role in identifying candidates for dual antiplatelet therapy after CABG
surgery. Fourth, discharge clopidogrel was determined using in-
1. Motwani JG, Topol EJ. Aortocoronary saphenous vein graft
hospital medication records and it was defined as administration
disease: pathogenesis, predisposition, and prevention. Circulation.
at any time the day after surgery through the date of discharge.
Therefore, the term "clopidogrel at discharge" is not consistent
2. Goldman S, Copeland J, Moritz T, Henderson W, Zadina K, Ovitt T, et
and does not necessarily means clopidogrel use at the time of
al. Long-term graft patency (3 years) after coronary artery surgery.
discharge. In addition, we did not have information on 1-year
Effects of aspirin: results of a VA Cooperative study. Circulation.
medication use for all patients. We demonstrated that only
3. Goldman S, Copeland J, Moritz T, Henderson W, Zadina K, Ovitt T, et
around one-third of the patients who were discharged on
al. Improvement in early saphenous vein graft patency after coronary
clopidogrel were on it for 1 year, and less than 10% of patients
artery bypass surgery with antiplatelet therapy: results of a Veterans
who did not receive clopidogrel at discharge were on it for 1 year.
Administration Cooperative Study. Circulation. 1988;77(6):1324-32.
Unfortunately, we did not collect the reasons for stopping and
4. Ebrahimi R, Bakaeen FG, Uberoi A, Ardehali A, Baltz JH, Hattler B, et al.
starting clopidogrel following CABG surgery. Nonetheless, this is
Effect of clopidogrel use post coronary artery bypass surgery on graft
one of the few studies that was able to describe medication use
patency. Ann Thorac Surg. 2014;97(1):15-21.
in 1 year, which provides important insights about adherence
5. Yusuf S, Zhao F, Mehta SR, Chrolavicius S, Tognoni G, Fox KK;
and medication persistence.
Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N
Engl J Med. 2001;345(7):494-502.
6. CAPRIE Steering Committee. A randomised, blinded, trial of
At our institution, clopidogrel was used in almost one-fifth
clopidogrel versus aspirin in patients at risk of ischaemic events
of patients following CABG surgery. Its use was not associated
(CAPRIE). Lancet. 1996;348(9038):1329-39.
with improved overall 1-year survival, yet may have some benefit
7. Gao G, Zheng Z, Pi Y, Lu B, Lu J, Hu S. Aspirin plus clopidogrel therapy
among those receiving off-pump CABG. Adequately powered
increases early venous graft patency after coronary artery bypass
randomized clinical trials are needed to determine whether
surgery a single-center, randomized, controlled trial. J Am Coll
there is a role for routine or selected use of clopidogrel or newer
antiplatelet agents after CABG surgery.
8. Fitchett D, Eikelboom J, Fremes S, Mazer D, Singh S, Bittira B, et al.
Brazilian Journal of Cardiovascular Surgery
Prates PRL, et al. - Clopidogrel Use After Myocardial Revascularization
Braz J Cardiovasc Surg 2016;31(2):106-14
Dual antiplatelet therapy in patients requiring urgent coronary
21. Rodrigues AJ, Evora PR, Tubino PV. On-pumb versus off-pump
artery bypass grafting surgery: a position statement of the Canadian
coronary artery bypass graft surgery: what do the evidence show?
Cardiovascular Society. Can J Cardiol. 2009;25(12):683-9.
Rev Bras Cir Cardiovasc. 2013;28(4):531-7.
9. Lorenz RL, Schacky CV, Weber M, Meister W, Kotzur J, Reichardt B,
22. Cantero MA, Almeida RM, Galhardo R. Analysis of immediate results of
et al. Improved aortocoronary bypass patency by low-dose aspirin
on-pump versus off-pump coronary artery bypass grafting surgery.
(100 mg daily). Effects on platelet aggregation and thromboxane
Rev Bras Cir Cardiovasc. 2012;27(1):38-44.
formation. Lancet. 1984;1(8389):1261-4.
23. Gabriel EA, Locali RF, Matsuoka PK, Cherbo T, Buffolo E. On-pump
10. Collaborative overview of randomised trials of antiplatelet therapy. II:
coronary artery bypass graft surgery: biochemical, hormonal and
Maintenance of vascular graft or arterial patency by antiplatelet therapy.
cellular features. Rev Bras Cir Cardivasc. 2011;26(4):525-31.
Antiplatelet Trialists' Collaboration. BMJ. 1994;308(6922):159-68.
24. Kim KB, Lim C, Lee C, Chae IH, Oh BH, Lee MM, et al. Off-pump
11. Goyal A, Alexander JH, Hafley GE, Graham SH, Mehta RH, Mack MJ,
coronary artery bypass may decrease the patency of saphenous vein
et al. Outcomes associated with the use of secondary prevention
grafts. Ann Thorac Surg. 2001;72(3):S1033-7.
medications after coronary artery bypass graft surgery. Ann Thorac
25. Mariani MA, Gu YJ, Boonstra PW, Grandjean JG, van Oeveren W, Ebels T.
Procoagulant activity after off-pump coronary operation: is the current
12. Gurbuz AT, Zia AA, Vuran AC, Cui H, Aytac A. Postoperative clopidogrel
anticoagulation adequate? Ann Thorac Surg. 1999;67(5):1370-5.
improves mid-term outcome after off-pump coronary artery
26. Moller CH, Steinbrüchel DA. Platelet function after coronary
bypass graft surgery: a prospective study. Eur J Cardiothorac Surg.
artery bypass grafting: is there a procoagulant activity after off-
pump compared with on-pump surgery? Scand Cardiovasc J.
13. Williams JB, Lopes RD, Hafley GE, Ferguson Jr TB, Mack MJ, Gibson
CM, et al. Relationship between postoperative clopidogrel use and
27. Hyde JA, Chinn JA, Graham TR. Platelets and cardiopulmonary bypass.
subsequent angiographic and clinical outcomes following coronary
artery bypass grafting. J Thromb Thrombolysis. 2013;36(4):384-93.
28. Patel MR, Dehmer GJ, Hirshfeld JW, Smith PK, Spertus JA; American
14. Brown BG, Cukingnan RA, DeRouen T, Goede LV, Wong M, Fee HJ, et
College of Cardiology Foundation Appropriateness Criteria Task Force;
al. Improved graft patency in patients treated with platelet-inhibiting
Society for Cardiovascular Angiography and Interventions; Society
therapy after coronary bypass surgery. Circulation. 1985;72(1):138-46.
of Thoracic Surgeons; American Association for Thoracic Surgery;
15. Chesebro JH, Clements IP, Fuster V, Elveback LR, Smith HC, Bardsley
American Heart Association, and the American Society of Nuclear
WT, et al. A platelet-inhibitor-drug trial in coronary-artery bypass
Cardiology Endorsed by the American Society of Echocardiography;
operations: benefit of perioperative dipyridamole and aspirin
Heart Failure Society of America; Society of Cardiovascular Computed
therapy on early postoperative vein-graft patency. N Engl J Med.
Tomography. ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Appropriateness
Criteria for Coronary Revascularization: a report by the American
16. Chesebro JH, Fuster V, Elveback LR, Clements IP, Smith HC, Holmes DR
College of Cardiology Foundation Appropriateness Criteria Task Force,
Jr, et al. Effect of dipyridamole and aspirin on late vein-graft patency
Society for Cardiovascular Angiography and Interventions, Society
after coronary bypass operations. N Engl J Med. 1984;310(4):209-14.
of Thoracic Surgeons, American Association for Thoracic Surgery,
17. Baur HR, VanTassel RA, Pierach CA, Gobel FL. Effects of sulfinpyrazone
American Heart Association, and the American Society of Nuclear
on early graft closure after myocardial revascularization. Am J Cardiol.
Cardiology Endorsed by the American Society of Echocardiography,
the Heart Failure Society of America, and the Society of Cardiovascular
18. Tricoci P, Roe MT, Mulgund J, Newby LK, Smith SC Jr, Pollack CV Jr,
Computed Tomography. J Am Coll Cardiol. 2009;53(6):530-53.
et al. Clopidogrel to treat patients with non-ST-segment elevation
29. Patel JH, Stoner JA, Owora A, Mathew ST, Thadani U. Evidence for
acute coronary syndromes after hospital discharge. Arch Intern Med.
using clopidogrel alone or in addition to aspirin in post coronary
artery bypass surgery patients. Am J Cardiol. 2009;103(12):1687-93.
19. Dropinski J, Jakiela B, Sanak M, Wegrzyn W, Biernat M, Dziedzina S,
30. Bhatt DL, Chew DP, Hirsch AT, Ringleb PA, Hacke W, Topol EJ.
et al. The additive antiplatelet action of clopidogrel in patients with
Superiority of clopidogrel versus aspirin in patients with prior cardiac
coronary artery disease treated with aspirin. Thromb Haemost.
surgery. Circulation. 2001;103(3):363-8.
31. Fox KA, Mehta SR, Peters R, Zhao F, Lakkis N, Gersh BJ, et al. Benefits and
20. Kulik A, Le May MR, Voisine P, Tardif JC, Delarochelliere R, Naidoo S, et
risks of the combination of clopidogrel and aspirin in patients undergoing
al. Aspirin plus clopidogrel versus aspirin alone after coronary artery
surgical revascularization for non-ST-elevation acute coronary syndrome:
bypass grafting: the clopidogrel after surgery for coronary artery
the Clopidogrel in Unstable angina to prevent Recurrent ischemic Events
disease (CASCADE) Trial. Circulation. 2010;122(25):2680-7.
(CURE) Trial. Circulation. 2004;110(10):1202-8.
Brazilian Journal of Cardiovascular Surgery
Source: http://rbccv.org/pdf/2522/v31n2a06.pdf
Medication review tips and hints for cardiovascular medication
Medication review tips and hints for Graham Parsons and Mark Stone Copthorne Hotel 18th August 2014 • Anti-hypertensive agents • Nitrates • Statins • Anticoagulants • Antiplatelets Anti-hypertensive agents • Angiotensin-Converting Enzyme (ACE) inhibitors • Angiotensin-II receptor antagonists (ARB) • Calcium Channel Blockers (CCB) • Diuretics • and -blockers
li-orange.com.tw
Negative Pressure Wound Therapy: Experience in 45 Dogs Kathryn A. Pitt, BS, DVM, MS, and Bryden J. Stanley, BVMS, MVetSc, Diplomate ACVS Department of Small Animal Clinical Sciences, College of Veterinary Medicine, Michigan State University, East Lansing, Michigan Corresponding Author Objective: To report experience with negative pressure wound therapy (NPWT) in 45 Bryden Stanley, BVMS, MVetSc, Diplomate