Praesidia.it
Nitinol Flexigrip Sternal Closure System and ChestWound Infections: Insight From a Comparative
Analysis of Complications and Costs
Jonida Bejko, MD, Vincenzo Tarzia, MD, Marco De Franceschi, BsD,
Roberto Bianco, MD, Massimo Castoro, MD, Tomaso Bottio, MD, PhD, and
Gino Gerosa, MD
Department of Cardiac Surgery, University of Padua, Medical School of Padua, Padua, Italy
Background. We sought to assess the efficiency of two
was significantly higher in group A (4.1% versus 1.7%;
different sternal closure techniques in preventing sternal
p ⴝ 0.03). Sternal surgical revision to treat a thoracic
wound complications (SWC). A cost analysis was also
instability was required in a significantly higher number
of patients in group A (9 patients, 1.9%) and in none of
Methods. Between January 2008 and April 2010, 1,644
group B (p ⴝ 0.004). The incidence of sternal instability,
consecutive cardiac surgery patients who underwent car-
secondary to wound infection, was significantly lower in
diac surgery in our institute were prospectively collected.
group B (p ⴝ 0.05). Overall costs were €7,407,296 and
A total of 1,072 patients received a standard parasternal
€6,896,432 in group A and group B, respectively. Thus,
wiring technique (group A), and 572 patients received a
nitinol clip closure technique offered a €510,864 cost
new method of sternal closure based on the use of
saving compared with standard steel wiring technique.
thermoreactive nitillium clips (Flexigrip; Praesidia SRL,
Conclusions. The Flexigrip assured a lower incidence
Bologna, Italy [group B]). We investigated, by a propen-
of SWC. The use of the nitinol clip favored an improved
sity matched analysis, whether the use of standard or
sternal closure technique preventing mediastinitis. Ad-
nitinol clip closure would impact on sternal wound
ditionally, the nitinol clip system proved to be cost
effective in cardiac surgery.
Results. In all, 464 patients of each group were matched
(Ann Thorac Surg 2012;94:1848 –53)
for 17 available risk factors. Overall incidence of SWC
2012 by The Society of Thoracic Surgeons
Despite the many advancements made in bone fixa- Material and Methods
tion and healing technology, the same method of
Ethics approval was granted by the University of Padova
sternal closure has been used for more than 100 years
Research Ethics Board, and individual patient consent
and is still the most common [1]. The use of sternal wire
was obtained. Between January 2008 and April 2010, 1,644
closure has been associated with various healing compli-
consecutive patients who underwent cardiac surgery and
cations, such as instability, nonunion, and infections
were prospectively entered into our Institutional data-
[2, 3]. Thus, despite the modern progress in postoperative
base were selected. No patient was excluded from the
management, the incidence of this complication has
remained stable over time, ranging from 2% to 5% [4 – 8].
The classical sternal closure technique using five or six
The Flexigrip (Praesidia SRL, Bologna, Italy) is a sternal
steel wires was applied in 1,072 patients (group A),
closure system composed of nitillium, a thermoreactive
whereas in 572 patients (group B), the sternal reapproxi-
alloy of nickel and titanium, commonly known as nitinol,
mation was obtained with the use of two to four nitillium
with a memory effect that acts as a brace holding together
clips. Demographics of both groups are summarized in
the sternal osteotomy (Fig 1).
Table 1. Coronary artery disease, bilateral internal tho-
The study aim was to evaluate, by propensity score
racic artery harvesting, chronic obstructive pulmonary
matching, whether the use of thermoreactive nitillium
disease, renal insufficiency, and long duration of total
clips, instead of standard sternal wiring, impacted on the
operative time—well-known risk factors for SWC—were
incidence of deep and superficial sternal wound compli-
significantly more frequent in group B. A superficial or
cations (SWC), completing the study with a detailed cost
deep SWC was observed in 46 patients from both group A
and group B. Univariate regression analysis showed that
ischemic cardiomyopathy, bilateral internal thoracic har-
vesting, diabetes mellitus, cross-clamp time, and total op-
Accepted for publication Aug 10, 2012.
erative time are significant risk factors for SWC (Table 2).
To compare similar populations affected by similar
Address correspondence to Dr Bottio, Cardiac Surgery Institute, Via
Giustiniani 2, Padova, Italy; e-mail: [email protected].
comorbidities, propensity scores were calculated. The 17
2012 by The Society of Thoracic Surgeons
Published by Elsevier Inc
Ann Thorac Surg
BEJKO ET AL
STERNAL NITINOL FLEXIGRIP AND WOUND INFECTIONS
descriptive and inferential statistical methods. Categori-
cal variables were expressed as absolute frequency dis-
tribution and percentage; continuous variables with a
normal distribution (assessed by the Shapiro-Wilk nor-
mality test) were expressed as mean ⫾ 1 SD. To deter-
mine the significant preoperative risk factors for infec-
tion, the relationship between SWC and risk factors was
analyzed in the unmatched population of this study by
using a regression univariate analysis. Propensity score
matching analysis (one-to-one matching based on pro-
pensity scores) was used to adjust for baseline character-
istic differences between the two groups. The propensity
score was estimated by a logistic regression model for
each patient. The comparison between groups was done
using the 2 test or Fisher's exact test, as appropriate.
Student's t test for unpaired data was used to compare
continuous variables. Statistical findings were considered
significant if the critical level was less than 5% (p ⬍ 0.05).
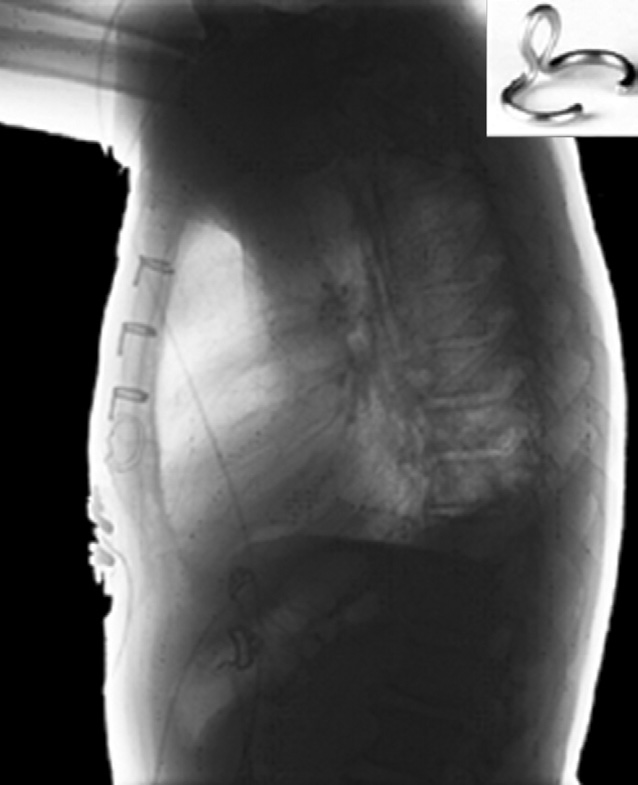
Nitillium Thermoreactive Clips
The nitinol clip is a sternal closure system with specific
indication in cardiothoracic surgery. The system is com-
posed of nitinol staples and an instrumentation kit. The
staple acts as a brace holding together the sternal osteot-
omy (Fig 1). The nitinol clip is composed of thermoreac-
tive alloy of nickel and titanium with a memory effect.
This means that the nitinol clip becomes malleable at less
Fig 1. Chest radiograph (lateral-lateral view). Note how the nitinol
than 10°C and recovers its shape when placed at more
clip staples brace, holding together the sternal halves.
than 25°C. The nitinol clip is applied through a hole
created bilaterally into the second, third, and forth or fifth
predictor variables collected for the analysis were as
intercostal space, according to the sternal length. Two
follows: age, sex, diabetes mellitus (defined as a history of
diabetes regardless of the duration of disease or need for
Table 1. Demographics Before Matching
antidiabetic agents), congestive heart failure (defined as
an ejection fraction of ⬍30%), type of cardiac procedure
(according to cardiac pathology: ischemic, valvular, and
(n ⫽ 1,072)
(n ⫽ 572)
others), severe chronic obstructive pulmonary disease
Age, years
67.53 ⫾ 11.61
67.06 ⫾ 12.23
according to The Society of Thoracic Surgeons scoring
766 (71.4%)
409 (71.5%)
(defined as a history of emphysema, chronic bronchitis,
and bronchiectasis, requiring long-term use of broncho-
444 (41.4%)
280 (48.9%)
dilators, or need for corticosteroid therapies), renal insuf-
400 (37.3%)
139 (24.3%)
ficiency (renal function was estimated by the serum
228 (21.3%)
153 (26.7%)
creatinine level of 1.5 mg/dL or greater), obesity (defined
as body mass index of 30 and above), body mass index,
43 (4.0%)
120 (21.0%)
bilateral internal thoracic arteries harvesting in coronary
108 (10.0%)
118 (20.6%)
artery bypass graft surgery, reintervention, urgency (due
228 (21.3%)
169 (29.5%)
to the hemodynamic instability), cross-clamp time, car-
291 (27.1%)
161 (28.1%)
diopulmonay by-pass time, and total operative time
187 (17.4)
83 (14.5%)
(Table 3).
106 (9.9%)
117 (20.4%)
The propensity score matching generated a matched
55 (5.1%)
44 (7.6%)
cohort in which the baseline prognostic variables were
Body mass index
18.50 ⫾ 0.34
18.40 ⫾ 0.29
well balanced. Of the entire population, 56.4% of the
250 (23.3%)
107 (18.7%)
patients (928 of 1,644) were perfectly matched for the
available risk factors with an equal distribution of risk
90.32 ⫾ 40.30
74.56 ⫾ 38,70
115.70 ⫾ 55.80
101.80 ⫾ 50,35
280.00 ⫾ 72.00
320.00 ⫾ 75.00
Data were processed using Excel, Access (Office 2007;
Microsoft Corp, Redmond, WA) and Stata version 10.0
BITA ⫽ bilateral internal thoracic artery;
CHF ⫽ congestive heart failure;
COPD ⫽ chronic obstructive pulmonary disease;
CPB ⫽ cardiopulmo-
for Windows (StataCorp, College Station, TX), using
nary by-pass time.
BEJKO ET AL
Ann Thorac Surg
STERNAL NITINOL FLEXIGRIP AND WOUND INFECTIONS
Table 2. Univariate Regression Analysis Before Matching of
fashion. Group A received conventional sternal closure
Patients With Sternal Wound Complication Versus Patients
using six or more transverse stainless steel wires. In cases
Without Sternal Wound Complication
of double thoracic artery harvesting or sternal friability, a
parasternal reinforcement was routinely applied. Group
B received two steel wires, one on the manubrium and
one on the xyphoid process for the sternal approxima-
Age, years
67.30 ⫾ 11.90
68.80 ⫾ 8.70
tion, and two to four nitillium thermoreactive clips ac-
38 (82.6%)
cording to the sternal length into the intercostals spaces.
Regardless of group, muscular fascia, subcutaneous tis-
697 (43.6%)
27 (58.7%)
sue, and skin were closed with running, interlaced fila-
531 (33.2%)
8 (17.4%)
ment, absorbable sutures. Both these sternal closure
370 (23.1%)
11 (23.9%)
techniques were adopted indifferently by each surgeon of
151 (9.4%)
12 (26.1%)
our cardiac unit, including the residents.
216 (13.5%)
10 (21.7%)
383 (24.0%)
14 (30.4%)
428 (26.8%)
24 (52.2%)
Surgical wounds were first inspected on the third post-
259 (16.2%)
11 (23.9%)
operative day, and if no complication occurred, addition-
216 (13.5%)
7 (15.2%)
ally changed on the fifth postoperative day. The previous
dressings were removed. The wounds were cleaned with
97 (6.1%)
iodine solution and were sterile dressed. Patients were
Body mass index
18.30 ⫾ 0.52
18.45 ⫾ 0.41
discharged electively on the fifth to seventh postopera-
314 (19.6%)
10 (21.7%)
tive day.
Febrile reactions were treated with paracetamol/
indomethacin unless a clear infective focus was isolated
70.32 ⫾ 39.40
82.40 ⫾ 40.30
in cultures (blood, urine, wound). Diabetic patients re-
99.30 ⫾ 42.50
105.70 ⫾ 52.80
ceived insulin till they returned to normal activity, ther-
290.00 ⫾ 88.00
340.00 ⫾ 90.00
apy, and diet. Patients with superficial wound infection
BITA ⫽ bilateral internal thoracic artery;
CHF ⫽ congestive heart failure;
were treated with local iodine solution and sterile dress-
COPD ⫽ chronic obstructive pulmonary disease;
CPB ⫽ cardiopulmo-
ing, with regular daily inspection of the wound.
nary by-pass time;
SWC ⫽ sternal wound complication.
steel wires are placed for the manubrium and the xy-
Table 3. Matched Population Characteristics and
phoid process approximation.
Distribution of Preoperative Risk Factors
(n ⫽ 464)
(n ⫽ 464)
All the patients, except the urgent cases, were showered
Age, years
66.50 ⫾ 12.32
67.00 ⫾ 12.73
and shaved the day before operation. The operative field
was painted with iodine solution. All skin surfaces of the
operative field were dressed with adhesive drapes.
Antibiotic prophylaxis was started at the call to the
operating room, in accordance with the protocol of the
center, starting immediately before the skin incision
and then with 1 to 2 repetitions during surgery, with
single endovenous vancomycin or associated with en-
dovenous gentamycin if femoral cannulation or saphe-
nous grafting were performed, at the doses of 2 g and
1.5 mg/kg, respectively. Vancomycin was continued
every 6 hours for 24 to 48 hours postoperatively,
depending on whether the drainage tubes were re-
moved; gentamycin was continued every 8 hours for 24
Body mass index
18.90 ⫾ 0.23
18.50 ⫾ 0.21
hours. Patients with vancomycin intolerance received
teicoplanin 600 mg at similar intervals, with monitored
teicoplanin serum concentrations.
79.70 ⫾ 41.20
75.80 ⫾ 36.20
112.00 ⫾ 53.20
107.00 ⫾ 52.30
All patients underwent standard median sternotomy
280.00 ⫾ 72.00
282.00 ⫾ 70.00
with a standard technique. Bone wax was routinely used
in all patients for sternum hemostasis. Cardiopulmonary
bypass was performed in all patients. Internal mammary
BITA ⫽ bilateral internal thoracic artery;
CHF ⫽ congestive heart failure;
COPD ⫽ chronic obstructive pulmonary disease;
CPB ⫽ cardiopulmo-
arteries were harvested with a pedicle or skeletonized
nary by-pass time.
Ann Thorac Surg
BEJKO ET AL
STERNAL NITINOL FLEXIGRIP AND WOUND INFECTIONS
If sternal dehiscence occurred, the patients were
cost resource. The following items for each procedure
treated with appropriate systemic antibiotics, wound
were considered: cost of the nitinol clip (€80 each); cost of
irrigation with iodine solution and sodium hypochlorite
the steel wires (€20 for each pack with six wires); daily
once daily. However, if the wound was found to be deep
cost of the VAC therapy; cost of implanting a Titanium
and large with important exposure of the subcutaneous
Sternal Fixation System (Synthes, West Chester, PA);
tissues, minimally invasive vacuum-assisted closure
hourly cost of the urgent use of the operating room; cost
(VAC) was selected. Dressings were changed twice a
of a day's recovery in hospital; daily cost of the intensive
week under aseptic conditions if wound culture results
care unit; and cost of the entire cardiac procedure (ac-
were positive for infection, or alternatively, once a week.
cording to the granted data of the sanitary direction of
our center).
To calculate the total cost for each patient, we multi-
According to the Centers for Disease Control and classi-
plied the unit cost of the various components of care by
fications, the infection of surgical wounds of sternoto-
the documented use and then summed the product.
mies should be considered as superficial if only the skin
Medical, nursing, and technical staff salaries were con-
and subcutaneous tissue are involved, deep when the
sidered in the total cost of the procedure for every
infection reaches the sternum but does not involve it, and
organ/space when sternal osteomyelitis or mediastinitis
occurs. For the benefit of consistency in comparing data,
SWC were subdivided into two groups. Superficial, when
it is confined to the subcutaneous tissue, and deep when
Totally, 464 patients for each group were matched, with
the bone or the mediastinum, or both, are involved.
balanced characteristics, providing unbiased estimation
Additionally, both superficial and deep complications
of the treatment, with similar patient comorbidities, and
were further subdivided into infected and not infected. A
procedure-related variables (Table 3).
wound complicated was retained infected in presence of
fever, leukocytosis, microbiological positive cultures and
Sternal Wound Complications
need of antibiotic therapy, or with local signs such as
wound drainage, redness, skin discharge or dehiscence,
OVERALL INCIDENCE. The overall incidence of SWC was
and fat necrosis. In absence of these clinical signs, the
2.9% (27 of 928; Table 4), becoming significantly higher in
wound, even if dehiscent, was considered not infected.
group A than in group B (19 patients in group A [4.1%]
versus 8 patients in group B [1.7%]; p ⫽ 0.03).
SUPERFICIAL INCIDENCE. The superficial chest wound com-
Actual hospital costs were calculated for every patient
plication incidence was similar in both groups. We ob-
who underwent either of the two sternal closing methods
served 17 cases of superficial chest wound complication,
(Table 3). Our cost-effectiveness analysis compared the
and in the majority of patients, the tissue shifting (skin
direct costs (patient care related) including the human
and subcutaneous dehiscence) was secondary to an in-
Table 4. Incidence of Sternal Wound Complications
Sternal Wound Complication Incidence
Group A (n ⫽ 464)
Group B (n ⫽ 464)
19 (4.1%)
Not infected
10 (2.1%)
Not infected
Not infected
9 (47.4%)
VAC therapy
9 (47.4%)
4 (50.0%)
24 (5.2%)
32 (6.9%)
Intensive care unit stay, days
2.38 ⫾ 3.89
2.09 ⫾ 5.28
Hospital stay, days
10.50 ⫾ 8.90
8.70 ⫾ 6.80
Hospital stay, days, patients with no SWC
8.00 ⫾ 4.60
7.90 ⫾ 3.90
Mean patient cost
€15,964 ⫾ €2,500
€14,863 ⫾ €1,100
SWC ⫽ sternal wound complication;
VAC ⫽ vacuum-assisted closure.
BEJKO ET AL
Ann Thorac Surg
STERNAL NITINOL FLEXIGRIP AND WOUND INFECTIONS
fection (11 patients). The infected cases were equally
Table 5. Items Included in the Total Cost Analysis
distributed between the groups: 5 in group 1 and 6 in
Total Cost Analysis
group B. Gram-positive bacteria were the most common
organisms involved; in 10 patients, Staphylococcus aureus
Nitillium clips and steel wires cost
was cultured. In the remaining case, methicillin-resistant
Medications, materials, and daily cost of vacuum-assisted
S aureus (MRSA) was isolated. The superficial wound
complication, when aseptic, occurred more frequently in
Synthes titanium sternal fixation
group A, although not significantly so (p ⫽ 0.22).
Hourly cost of the urgency use of operating room
DEEP INCIDENCE. The association of wound dehiscence and
Length of intensive care unit stay (days)
concomitant sternal instability, namely, deep wound
Length of hospital recovery (days)
complication, was significantly more frequent in group A
Cardiac procedure cost, including human costs
(9 patients [1.9%]) in comparison with group B (1 patient
[0.2%]; p ⫽ 0.01). In 5 patients (all group A), we observed
an infected deep wound complication associated with
sternal instability and dehiscence, whereas in another 5
clip cost was higher than the steel wire cost. The pur-
cases, the deep complication was due to an aseptic
chase price for nitinol clips overcharged group B
sternal mechanical instability (4 in group A and 1 in
€135,360. Mean government reimbursement for each
group B). The causative bacteria isolated were gram-
group was €11,136,000 (mean for patient €24,000, ranging
negative organisms: Pseudomonas sp were cultured in 2
between €15,000 and €120,000). Thus, considering the
patients, and Enterobacter sp were isolated in 3 patients.
general costs in both groups, the complications costs, and
Sternal surgical revision to treat thoracic instability
the costs related to the nitinol clip price, the calculated
was required in 9 of 19 patients of group A (47.4%) and in
hospital profit was €3,728,704 for group A and €4,239.568
none of group B, achieving a significantly different inci-
for group B.
dence (p ⫽ 0.004). The association of wound infection and
sternal instability was significantly lower in group B (0
cases) than in group A (5 cases; p ⫽ 0.05).
The aim of this study was to evaluate whether the sternal
closure with the nitinol Flexigrip system improves me-
Among all the patients who had SWC, none died in group
chanical stability and to investigate its influence on the
B whereas 1 patient died in group A (p ⫽ 1.00). Totally, 9 of
prevention of SWC. Moreover, we provided a detailed
19 patients in group A required a VAC dressing therapy for
cost analysis to verify whether the unrestricted use of this
delayed wound healing versus 4 of 8 patients in group B.
device may reduce the overall costs related to the pa-
The incidence was similar in both groups (p ⫽ 0.16).
Additionally, also the intensive care unit stay results were
Several strategies to prevent mediastinitis, sternal de-
similar (p ⫽ 0.34). Nine patients in group A underwent
hiscence, or both have been previously published [9 –11],
sternal surgical revision to reapproximate the sternum, to
but there is still a lot of controversy. Robicsek and
correct extensive bone disruption. In 2 of them, it was
coworkers [9] proposed a parasternal wire suture in the
necessary to use the Synthes titanium fixation system to
presence of a frail and osteoporotic sternum. Sutherland
treat a rib and sternum continuity loss. No patient in group
and colleagues [10] modified and simplified this sternal
B necessitated a similar treatment. In the single patient in
support technique. In both cases, the concept is to atten-
group B who had an aseptic sternal instability, the sternum
uate the transverse forces exercised on the bone by the
resynthesis was unnecessary because the instability was
transversal wires. A common belief is that wound infec-
limited to the manubrium. Patients in group A had a
tion is largely technique dependent, and therefore, both
significantly longer hospital stay than the patients in
closure method and materials should provide stable
group B (p ⫽ 0.0006). Excluding from the analysis patients
repair [11]. However, various conditions have been iden-
in whom a SWC occurred, the mean hospital stay was
tified as potential risk factors. The clinical experience and
similar in both groups (p ⫽ 0.72). The incidence of
the results reported in the literature suggest that the
postoperative respiratory failure was comparable for
etiology of sternal wound complications is multifactorial
both groups (p ⫽ 0.27); we observed 24 cases in group A
[12–15]. Furthermore, in the presence of sternal instabil-
and 32 cases in group B.
ity, the eventually associated infection may propagate
deeply in the mediastinum, involving the cardiac sutures
with consequent septic shock. The correlated mortality
The cost for cure was higher for group A than for group
ranges between 5% and 47% [6, 15] in spite of early
B, although the difference was not significant (p ⫽ 0.99).
diagnosis and appropriate treatment [16]. That increases
Overall costs, considering cardiac procedure costs, hos-
the costs and the length of hospital stay, and usually
pital stay, and complication treatments (Table 5), were
amounts to a large waste of resources.
€7,407,296 for group A and €6,896,432 for group B. The
We analyzed the results observed in two similar pop-
main differences in costs between the two groups con-
ulations of propensity matched patients, and different
sisted of the costs related to the complication treatments
from each other only for the sternal closing technique
and prolonged hospitalization, even though the nitinol
adopted: standard wiring technique versus nitinol clip.
Ann Thorac Surg
BEJKO ET AL
STERNAL NITINOL FLEXIGRIP AND WOUND INFECTIONS
According to our series, although the results obtained
literature. Currently, we are modifying our sternal closing
with the standard wiring technique replicate those ob-
technique favoring more frequently the use of the nitinol
served in the literature, reflecting the efforts made to
clip, with the aim to standardize a technique and to reduce
provide continuous and scrupulous patient care, the
the complications related to both the clinical and the sur-
outcomes obtained by using the nitinol clip were by far
gical and surgeon variables.
superior. According to our experience, the overall inci-
In conclusion, we believe that this method of sternal
dence of SWC was significantly higher among the pa-
closure guarantees better clinical outcomes. Additionally,
tients in whom was applied the classic steel wires closure
because the costs of SWC management can highly in-
technique. Superficial SWC had similar incidence in the
crease the primary cost of hospitalization, to nearly twice
two groups, with no difference for the infected and not
the costs related to the unrestricted use of the nitinol clip,
infected. The deep SWC incidence, either in presence or
our results show that Flexigrip clips are cost effective.
absence of infection, was significantly higher with the
standard steel wires closure. None of the patients of
group B had a deep wound complication with a septic
sternal dehiscence, whereas in 5 patients of group A, an
1. Milton AF, cited by Kirschner M. [Tratado de tecnica opera-
infected deep wound complication associated with a
toria general y especial.] Barcelona: Editorial Labor, 1942;4:
sternal instability and bone disruption was observed,
756 – 60.
requiring a thoracic revision. Additionally, 4 cases of
2. Taber RE, Madaras O. Prevention of sternotomy wound
aseptic deep wound complication with sternal instability,
disruptions by use of figure-of-eight pericostal sutures. Ann
Thorac Surg 1969;8:367–9.
which required a thoracic revision, were observed in
3. Grossi EA, Culliford AT, Krieger KH, et al. A survey of 77
group A. Similar results have been observed in a pro-
major infectious complications of median sternotomy: a
spective study published by Negri and colleagues [12] in
review of 7,949 consecutive operative procedures. Ann Tho-
which 1,000 patients were randomly allocated to either
rac Surg 1985;40:214 –23.
standard or nitinol clip sternal closure. The researchers
4. Cheng W, Cameron DE, Warden KE, Fonger JD, Gott VL.
Biomechanical study of sternal closure techniques. Ann
concluded there was a significant reduction of SWC in
Thorac Surg 1993;55:737– 40.
the group who received a sternal nitinol clip. However, in
5. Sirivella S, Zikria EA, Ford WB, Samadani SR, Miller WH,
our series, considering that we did not exclude any
Sullivan ME. Improved technique for closure of median
patient—whether urgent, emergent, or heart transplant
sternotomy incision: Mersilene taper versus standard wire
patient— our results appear even superior to those re-
closure. J Thorac Cardiovasc Surg 1987;94:591–5.
6. El Oakley RM, Wright JE. Postoperative mediastinitis: clas-
ported by Negri and coworkers [12], increasing the effec-
sification and management. Ann Thorac Surg 1996;61:
tiveness of nitinol clip use.
1030 – 6.
The staple of the nitinol clip acts as brace holding
7. Blanchard A, Hurni M, Ruchat P, Stumpe F, Fischer A,
together sternal halves, thus preserving sternal flexibil-
Sadeghi H. Incidence of deep and superficial sternal infec-
ity. Additionally, as the tension applied is standard, the
tion after open heart surgery. A ten years retrospective study
efficacy does not depend on users, avoiding the bias
from 1981 to 1991. Eur J Cardiothorac Surg 1995;9:153–7.
8. Milano CA, Kesler K, Archibald N, Sexton D, Jones RH.
related to the surgeon. This is important especially for
Mediastinitis after coronary artery bypass graft surgery: risk
patients with chronic obstructive pulmonary disease in
factors and longterm survival. Circulation 1995;92:2245–51.
whom the cough appears particularly abundant and
9. Robicsek F, Daugherty HK, Cook JW. The prevention and
productive postoperatively. On the contrary, in the steel
treatment of sternum separation following open-heart sur-
wires closure technique, the physiologic sternal move-
gery. J Thorac Cardiovasc Surg 1977;73:267– 8.
10. Sutherland RD, Martinez HE, Guynes WA. A rapid, secure
ments during cough may stress the bone fixed by the
method of sternal closure. Cardiovascular disease. Bull
wires, provoking microfractures surrounding the sternal
Texas Heart Inst 1981;8:54 –5.
wires. These inevitably favor a reduced contact between
11. Bottio T, Rizzoli G, Vida, V, Casarotto D, Gerosa G. Double
the sternal halves, and consequently, a continuous flat-
crisscross sternal wiring and chest wound infections: a
tening of the bone and of the tissue placed above.
prospective randomized study. J Thorac Cardiovasc Surg
2003;126:1352– 6.
Because no patient in group B had a deep SWC requiring
12. Negri A, Manfredi J, Terrini A, et al. Prospective evaluation
a bone revision, the nitinol clip was demonstrated to be a
of a new sternal closure method with thermoreactive clips.
protective factor against sternal dehiscence even in case
Eur J Cardiothorac Surg 2002;571–5.
of infected wound.
13. Borger MA, Rao V, Weisel RD, et al. Deep sternal wound
Prolonged hospital stay and complication treatments
infection: risk factors and outcomes. Ann Thorac Surg 1998;
place a high demand on hospital resources. Strategies that
65:1050 – 6.
14. Kouchoukos NT, Wareing TH, Murphy SF, Pelate C, Mar-
can effectively reduce the incidence of those complications
shall WG. Risks of bilateral internal mammary artery bypass
might also potentially reduce resource use and costs. With
grafting. Ann Thorac Surg 1990;49:210 –9.
an unrestricted nitinol clip application for the sternal clo-
15. Liu JY, Birkmeyer NJ, Sanders JH, et al. Risks of morbidity
sure, we observed an overall cost reduction of €510.735. The
and mortality in dialysis patients undergoing coronary ar-
treatment of the complications dominated the cost differ-
tery bypass surgery. Northern New England Cardiovascular
Disease Study Group. Circulation 2000;102:2973–7.
ence. Therefore, the nitinol clip use favored a hospital profit
16. Bitkover CY, Gaerlund B. Mediastinitis after cardiovascular
of 13%. No previous similar cost analysis study regarding
operations: a case-control study for risk actors. Ann Thorac
the Flexigrip system in sternal closure was described in the
Surg 1998;65:36 – 40.
Source: http://www.praesidia.it/wp-content/uploads/2015/01/Flexigrip-Chest-Wound-Infections-_-Insight-From-a-Comparative-Analysis-of-Complications-and-Costs.pdf
Assessing the impact of pharmaceutical communication channels on general practitioners' drug prescribing intentions
Inzinerine Ekonomika-Engineering Economics, 2015, 26(5), 541–550 Revisiting the Role of Traditional, Electronic and Mobile-Based Communication Channels in the Pharmaceutical Industry of Lithuania Vilte Auruskeviciene1, Jovita Butkeviciene2, Laura Salciuviene3 1,2ISM University of Management and Economics Arkliu st. 18, LT-01305, Vilnius, Lithuania [email protected] 3Lancaster University Management School Lancaster, LA1 4YX, United Kingdom, E-mail
Postoperative pain and early quality of life after radiofrequency ablation and mechanochemical endovenous ablation of incompetent great saphenous veins
Postoperative pain and early quality of life afterradiofrequency ablation and mechanochemicalendovenous ablation of incompetent greatsaphenous veins Ramon R. J. P. van Eekeren, MD,a Doeke Boersma, MD,b Vincent Konijn, MD,aJean Paul P. M. de Vries, MD, PhD,b and Michel M. J. P. Reijnen, MP, PhD,a Arnhem and Nieuwegein,The Netherlands