Untitled
Common and Unique Therapeutic Mechanismsof Stimulant and Nonstimulant Treatments
for Attention-Deficit/Hyperactivity Disorder
Kurt P. Schulz, PhD; Jin Fan, PhD; Anne-Claude V. Be´dard, PhD; Suzanne M. Clerkin, PhD; Iliyan Ivanov, MD;Cheuk Y. Tang, PhD; Jeffrey M. Halperin, PhD; Jeffrey H. Newcorn, MD Context: Attention-deficit/hyperactivity disorder (ADHD)
vestigator-completed ratings on the ADHD Rating Scale- is a highly prevalent and impairing psychiatric disorder IV-Parent Version.
that affects both children and adults. There are Food andDrug Administration–approved stimulant and nonstimu- Results: Treatment with methylphenidate vs atomox-
lant medications for treating ADHD; however, little is etine was associated with comparable improvements in both known about the mechanisms by which these different response inhibition on the go/no-go test and mean (SD) treatments exert their therapeutic effects.
improvements in ratings of ADHD symptoms (55% [30%]vs 57% [25%]). Improvement in ADHD symptoms was as- Objective: To contrast changes in brain activation re-
sociated with common reductions in bilateral motor cor- lated to symptomatic improvement with use of the stimu- tex activation for both treatments. Symptomatic improve- lant methylphenidate hydrochloride vs the nonstimu- ment was also differentially related to gains in task-related lant atomoxetine hydrochloride.
activation for atomoxetine and reductions in activation formethylphenidate in the right inferior frontal gyrus, left an- Design: Functional magnetic resonance imaging be-
terior cingulate/supplementary motor area, and bilateral pos- fore and after 6 to 8 weeks of treatment with methylphe-nidate (n = 18) or atomoxetine (n = 18) using a parallel- terior cingulate cortex. These findings were not attribut- groups design.
able to baseline differences in activation.
Setting: Specialized ADHD clinical research program at
Conclusions: Treatment with methylphenidate and ato-
Mount Sinai School of Medicine, New York, New York.
moxetine produces symptomatic improvement via bothcommon and divergent neurophysiologic actions in fron- Participants: Thirty-six youth with ADHD (mean [SD]
toparietal regions that have been implicated in the patho- age, 11.2 [2.7] years; 27 boys) recruited from random- physiology of ADHD. These results represent a first step in ized clinical trials.
delineating the neurobiological basis of differential responseto stimulant and nonstimulant medications for ADHD.
Main Outcome Measures: Changes in brain activa-
tion during a go/no-go test of response inhibition and in-
Arch Gen Psychiatry. 2012;69(9):952-961 activity disorder (ADHD) is a selective NET inhibitor that has little af- a highly prevalent and im- finity for DAT.3 The partially overlapping pairing psychiatric disor- pharmacologic profiles of these medica- der that affects both chil- tions suggest both similarities and differ- dren and adults and accounts for an outsized ences in their therapeutic mechanisms of ac- portion of psychotropic medication use in tion, consistent with reports that many youth.1 Yet, the mechanisms by which Food children with ADHD respond to both treat- Departments of Psychiatry(Drs Schulz, Fan, Be´dard, and Drug Administration–approved stimu- ments but that approximately one-third re- Clerkin, Ivanov, Tang, Halperin, lant and nonstimulant medications for spond preferentially to one or the other.4 and Newcorn), Neuroscience ADHD exert their therapeutic effects are The acute pharmacologic actions of (Dr Fan), Radiology (Dr Tang), poorly understood, and there are almost no single challenge doses of methylphenidate and Pediatrics (Dr Newcorn), data to guide treatment selection. The psy- and atomoxetine provide preliminary evi- Mount Sinai School of chostimulant methylphenidate hydrochlo- dence about the results of comparative treat- Medicine, New York, New York; ride, a mainstay of ADHD treatment, is an ment efficacy studies.4 Positive responses to and Department of Psychology, indirect catecholamine agonist that blocks both medications may reflect similar acute Queens College of the City both dopamine transporter (DAT) and nor- actions on inhibitory and executive func- University of New York,Flushing, New York (Drs Fan epinephrine transporter (NET),2 whereas tions of the prefrontal cortex5-11 and, pos- and Halperin).
atomoxetine hydrochloride, the first ap- sibly, the anterior cingulate cortex.7,8 Ato- ARCH GEN PSYCHIATRY/ VOL 69 (NO. 9), SEP 2012 2012 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a Mt Sinai School Of Medicine User on 09/05/2012
moxetine and methylphenidate act at promiscuous NETs parents were financially compensated for participation. Par- that clear both dopamine and norepinephrine in prefron- ticipants were recruited from 2 industry-sponsored trials (n=4) tal regions that lack DAT.12-14 Methylphenidate may also and from a National Institutes of Health–funded treatment study act via the abundant DAT expressed in striatum to en- (n = 32) conducted between 2004 and 2011. Thirty-six youth hance inhibitory functions6-8,15 and through the moderate (27 boys and 9 girls) with a mean (SD) age of 11.2 (2.7) years(age range, 7-17 years) completed the study procedures and levels of DAT in posterior cingulate cortex to suppress task- were included in the present analyses. Consent was addition- independent activity that has been linked to distractibil- ally obtained from 16 youth who did not complete the proce- ity.11,15-18 In contrast, atomoxetine has little effect on neu- dures, 3 for excessive motion or anxiety during baseline MRI ronal activity in striatum,12 where there is sparse expression and 13 because they dropped out of the study before complet- of NET,19 and the possible effects of atomoxetine on the ing posttreatment MRI (Figure 1). Seven of the latter 13 chil-
few NETs present in posterior cingulate cortex are poorly dren were never randomized to treatment, and 3 children each understood.11,19 The additional therapeutic actions of meth- discontinued treatment with atomoxetine and methylpheni- ylphenidate could account for the larger-effect size re- date owing to either nonresponse or adverse events. These youth ported for stimulants than for atomoxetine.4 However, there did not differ in age, sex, subtype, severity, or comorbidity from are likely important neuropharmacologic differences be- the 36 study completers.
Participants all met the DSM-IV criteria for ADHD, any sub- tween single-challenge doses of medication and treat- type, on the Kiddie Schedule for Affective Disorders and Schizo- ment administered over a more extended period. The rel- phrenia for School-Age Children–Present and Lifetime Ver- evance of the acute effects of single-challenge doses to the sion26 and were rated at least 1.5 SD above age and sex norms on symptomatic improvement produced by ADHD medica- the ADHD Rating Scale-IV-Parent Version (ADHD-RS-IV).27 The tions over the course of treatment is not clear, particularly exclusion criteria were poor response or tolerability to an ad- for atomoxetine, which takes several weeks to exert its clini- equate trial of either methylphenidate or atomoxetine; a sub- cal effects.20,21 stance abuse history or a positive urine screening test result; par- Little is known about how ongoing treatment of ADHD ticipation in a treatment study in the past 30 days; a past or affects neural activity, and, more important, how the neu- present primary diagnosis of mood, anxiety, or psychotic disor- rophysiologic changes produced by treatment relate to der; head injury; and any medical condition that could affectbrain function. Twenty-three participants were medication na- clinical improvement. Several weeks of methylpheni- ive. Of the remaining 13 participants, 5 had taken a stimulant date treatment for ADHD was found to downregulate stria- medication at some point before the study but not at study en- tal DAT,22 reduce striatal and prefrontal resting perfu- rollment. Eight participants were taking a stimulant medication sion,23,24 and enhance inhibitory-related activation in the when they enrolled in the study, and they completed a 2-week prefrontal cortex and anterior cingulate cortex,25 al- washout before the baseline visit. None of the participants were though only the last finding was tenuously linked to clini- receiving nonstimulant medications when they enrolled in the cal improvement.25 Similar information is not available for atomoxetine.
The lack of data linking pharmacologic actions to thera- peutic improvement represents a missed opportunity to bet- STUDY DESIGN
ter understand how medications work, an essential step indeveloping targeted approaches to treatment. Therefore, Thirty-six participants were randomly assigned to treatment withosmotically released methylphenidate hydrochloride (Concerta; we used event-related functional magnetic resonance McNeil-PPC Inc) (n=18) or atomoxetine hydrochloride (Strat- imaging (MRI) to compare the relationship between symp- tera; Eli Lilly & Co) (n=18) as part of the double-blind clinical tomatic improvement and changes in brain activation dur- trials in which they were enrolled. The mean (SD) length of treat- ing response inhibition produced by 6 to 8 weeks of treat- ment was 52 (16) days for methylphenidate and 54 (17) days for ment with methylphenidate vs atomoxetine in youth with atomoxetine (t34=0.78; P=.75). Medication was titrated to a stan- ADHD. Based on findings from single-dose challenge stud- dard of optimal response and tolerability using sequential dose- ies,5-10,12,13 we initially hypothesized that symptomatic im- escalating procedures, with an absolute dose schedule for meth- provement would be related to gains in neural activation ylphenidate and a weight-adjusted schedule for atomoxetine, as during response inhibition in the prefrontal cortex and an- per standard clinical practice. Methylphenidate hydrochloride ad- terior cingulate cortex for both medications but that im- ministration was initiated at 18 mg/d and was titrated upward in18-mg/d increments to a maximum daily dose of 72 mg. Ato- provement would be associated with increased striatal ac- moxetine hydrochloride therapy was started at a daily dose of 0.5 tivation for methylphenidate only. Findings from more or 0.8 mg/kg (depending on the trial) and was titrated to 1.8 mg/kg recent studies11,16-18 suggest that methylphenidate, and pos- using either a flexible (n = 4) or a stepped (n = 32) dose- sibly atomoxetine, could also decrease activation (ie, task- optimizing approach, with a maximum total daily dose of 120 mg.
related interference) in the posterior cingulate cortex.
The mean (SE) daily dose at posttreatment MRI was 54.0 (3.6)mg for methylphenidate hydrochloride and 1.4 (0.1) mg/kg foratomoxetine hydrochloride. Posttreatment MRIs and assess- ments were conducted once participants had achieved a stableresponse at the optimal dose (the highest dose tolerated in rela- tion to room for clinical improvement and tolerability). Post-treatment MRIs were conducted a mean (SD) of 5.3 (2.4) hours This study was approved by the institutional review board of after the administration of methylphenidate and 5.0 (2.2) hours Mount Sinai School of Medicine, New York, New York. Writ- after atomoxetine administration (t34=0.45; P=.66), within the ten informed consent was obtained from the parents of all the window of activity for both treatments.28,29 Youth treated with participants. Verbal assent from all the participants was certi- methylphenidate vs atomoxetine did not differ on any charac- fied by a witness unaffiliated with the study. Youth and their teristics at baseline (Table 1).
ARCH GEN PSYCHIATRY/ VOL 69 (NO. 9), SEP 2012 2012 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a Mt Sinai School Of Medicine User on 09/05/2012
4 Youth with ADHD recruited 48 Youth with ADHD recruited from industry-sponsored trials from the NIMH-funded trial 52 Youth attempted baseline fMRI 3 Excluded for anxiety or motion 7 Discontinued before randomization 21 Assigned to receive methylphenidate 21 Assigned to receive atomoxetine 3 Discontinued the trial 3 Discontinued the trial 18 Completed 6-8 wk of treatment 18 Completed 6-8 wk of treatment 18 Completed posttreatment fMRI scan 18 Completed posttreatment fMRI scan Figure 1. Flow diagram of participant progress through the study. Shading denotes procedures performed as part of the present study. ADHD indicates
attention-deficit/hyperactivity disorder; fMRI, functional magnetic resonance imaging; and NIMH, National Institute of Mental Health.
Table 1. Baseline Demographic and Clinical Characteristics of the Study Sample
Age, mean (SD), y t34 = 0.39 ADHD subtype, No. (%) ADHD-RS-IV total score, mean (SD) t34 = 0.68 Previous stimulant treatment for ADHD, No. (%) Required washout, No. (%) Abbreviations: ADHD, attention-deficit/hyperactivity disorder; ADHD-RS-IV, ADHD Rating Scale-IV-Parent Version; ODD, oppositional defiant disorder.
Participants performed an established go/no-go task31-33 dur-ing functional MRIs. The task measured the ability to inhibit The ADHD-RS-IV total score served as the measure of clini- responses to rare nontargets (no-go trials) in the context of cal response. The ADHD-RS-IV is a validated scale with 18 responding to frequent targets (go trials). The task consisted items that correspond to each of the behavioral descriptors of 6 runs that each lasted 4 minutes. Each run began with 10 of ADHD in the DSM-IV.27,30 The frequency/severity of each seconds of fixation and contained 57 trials (43 go trials item in the past week was scored from 0 (never or rarely) to [75%] and 14 no-go trials [25%]). Stimuli were presented 3 (very often) after an interview with the parent(s) (and ado- for 500 milliseconds, with an interstimulus interval of 3500 lescent for youth aged ⱖ13 years). Percentage change in the milliseconds. Promotional images from the Spiderman movie ADHD-RS-IV total score was calculated by dividing the dif- were used as stimuli. Participants were instructed to respond ference of the baseline and posttreatment scores by the base- as quickly and accurately as possible with the right hand line score, and multiplying by 100.
using a fiberoptic button system. The percentage of correctly ARCH GEN PSYCHIATRY/ VOL 69 (NO. 9), SEP 2012 2012 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a Mt Sinai School Of Medicine User on 09/05/2012
Table 2. Motion and Task Performance During MRI and Clinical Outcomea
Main Effect of
Main Effect of
Time ⴛ Group
Correct inhibitions, % Correct responses, % RTSD, milliseconds Translational, mm Usable functional runs, No.
ADHD-RS-IV total score Abbreviations: ADHD, attention-deficit hyperactivty disorder; ADHD-RS-IV, ADHD Rating Scale-IV-Parent Version; MRI, magnetic resonance imaging; post-Tx, posttreatment; RT, reaction time; RTSD, RT standard deviation.
a Data are given as mean (SD). Performance, motion, and clinical outcome were tested with separate 2 (time: baseline vs post-Tx) ⫻ 2 (group: methylphenidate vs atomoxetine) repeated-measures analyses of variance.
b P = .02.
c P ⬍ .01.
d P ⬍ .001.
inhibited responses on no-go trials served as the measure of sociation of age with improvement in the entire sample and for differences in this association between treatment groups, re-spectively. Behavioral results are reported at a 2-tailed signifi- cance level of P ⬍.05.
Brain activation during response inhibition was measured usingevent-related functional MRI. Participants underwent MRI twiceusing the same 3.0-T head-dedicated MRI machine (Siemens FUNCTIONAL MRI DATA ANALYSES
Allegra; Siemens Medical Systems). Six series of 120 func-tional T2*-weighted images depicting the blood oxygenation level–dependent signal were acquired in the axial plane usinggradient-echo echo-planar imaging (repetition time, 2 sec- Functional images were processed using statistical parametric map- onds; echo time, 40 milliseconds; section thickness, 3 mm; gap, ping software (SPM8; Wellcome Trust Center for Neuroimag- 1 mm; resolution, 3.28 mm2; and 28 sections). A high- ing). Each participant's baseline and posttreatment functional time resolution T2-weighted anatomic volume of the brain was ac- series were separately motion corrected, and functional series with quired at the same 28 section locations using a turbo spin- more than 1 voxel (4 mm) of motion were discarded. The meth- echo pulse sequence (section thickness, 4 mm with no gap; and ylphenidate and atomoxetine groups did not differ in mean (SD) in-plane resolution, 0.41 mm2).
translational movement, rotational displacement, or number of
functional series included in the analysis (Table 2). The remain-
ing baseline and posttreatment functional time series were co-registered to their respective high-resolution T2-weighted im- The effects of treatment on response inhibition and ADHD symp- ages (section thickness, 4 mm; 28 sections) and then to each other.
toms were analyzed using separate 2-way repeated-measures The functional images were subsequently spatially normalized to analyses of variance, in which the percentage of correct inhi- a standard template (Montreal Neurological Institute) using nor- bitions and the ADHD-RS-IV total score served as dependent malization parameters estimated from the baseline high- measures. Medication (methylphenidate vs atomoxetine) served resolution T2-weighted image and were then resampled using a as the between-group factor and time (baseline vs posttreat- sinc interpolation, resulting in a voxel size of 2⫻2⫻2 mm. Co- ment) as the within-group factor. Additional analyses of vari- registered and spatially normalized functional images were checked ance tested the percentage of correct responses, reaction time manually by 2 of us (K.P.S. and J.F.). Finally, the functional im- (RT), and the standard deviation of RT on go trials.
ages were smoothed using an 8⫻8⫻16-mm full-width at half The relationship of age to symptomatic improvement for maximum gaussian kernel.
methylphenidate vs atomoxetine treatment was examined using First-level analyses used a within-subjects design to contrast stepwise linear regression, in which the ADHD-RS-IV change activation in baseline vs posttreatment MRIs for each partici- score served as the dependent measure. Age was entered as a pant. A general linear model was conducted to determine the re- continuous variable in the first step of the regression. The sec- lationship between observed event-related blood oxygenation ond step consisted of the dichotomous medication variable, level–dependent signals and 4 regressors that represented ex- which was entered as a prelude to testing the interaction (ie, pected neural responses to correct and incorrect no-go and go product) of the dichotomous medication variable with the age events.34 Six motion parameters were entered as covariates of no variable in the third step. The age and medication variables were interest.35 The neural effect of response inhibition and the im- centered on zero. The F tests of the change in R2 for the first pact of treatment on this activation were modeled by applying and third steps of the regression were used to test for the as- appropriate linear contrasts to parameter estimates for correct ARCH GEN PSYCHIATRY/ VOL 69 (NO. 9), SEP 2012 2012 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a Mt Sinai School Of Medicine User on 09/05/2012
activated voxel was set at P ⬍ .005, and the extent (cluster)threshold was fixed at ⬎100 voxels. A Monte Carlo simula- tion (procedure described by Slotnick and Schacter37) that ac-counted for image resolution and smoothing parameters es- tablished that a cluster extent of 100 contiguous resampled voxels (2 mm3) corrected for multiple voxel comparisons at P ⬍.01. To illustrate significant findings, parameter estimates for hemodynamic signal change were extracted from volumesof interest that were defined as 8-mm-radius spheres centered at the peaks of maximal activation.
Mean Correct Inhibitions, % CLINICAL AND BEHAVIORAL IMPROVEMENT
Treatment with methylphenidate vs atomoxetine was as- sociated with comparable improvements in both ADHDsymptoms and response inhibition on the go/no-go task Figure 2. Treatment improved ratings of attention-deficit/hyperactivity
(Figure 2). Separate repeated-measures analysis of vari-
disorder (ADHD) symptoms and response inhibition on the go/no-go task.
ance revealed significant main effects of time for both the A, Treatment significantly reduced ratings on the total score of the ADHD ADHD-RS-IV total score (F1,34=102.33, P⬍.001) and the Rating Scale-IV-Parent Version (ADHD-RS-IV) (F1,34=102.33, P⬍.001). The percentage of correct inhibitions on no-go trials mean percentage improvement in the ADHD-RS-IV ratings was 55% for themethylphenidate group and 57% for the atomoxetine group. B, Treatment (F1,34=5.77, P=.02). Treatment also increased the speed also increased the percentage of successful inhibitions on no-go trials of the and reduced the variability of responses on go trials, with go/no-go task (F1,34=5.77, P=.02). There were no differences between the 2 significant main effects of time for RT (F1,34= 8.88, medications in the improvement of symptom ratings and inhibitory functionover treatment. Error bars indicate 1 SD. Asterisks indicate significant time P ⬍ .001) and standard deviation of RT (F1,34= 8.25, effects (baseline vs posttreatment). Methylphenidate and atomoxetine both P ⬍.001). However, no significant main effects of medi- given in hydrochloride form.
cation or time ⫻medication interactions for any of theperformance measures were noted (Table 2).
no-go events minus correct go events in the baseline MRI and in Mean (SD) ADHD-RS-IV change scores did not differ the posttreatment minus baseline MRIs, respectively, resulting in for methylphenidate vs atomoxetine (55% [30%] vs 57% 2 contrast maps per participant.
[23%], t34=0.52, P=.88). Stepwise linear regression foundno association of symptomatic improvement with age in either the whole sample or the separate medication groups.
Specifically, only a small proportion of the variance was Second-level random-effects group analyses of the functional accounted for by the ADHD-RS-IV change score en- imaging data were conducted using SPM8 software. Prelimi- tered in step 1 (R2=0.001, F1,34=0.02, P=.88) and the medi- nary t tests were performed to define baseline activation re- cation variable entered in step 2 (R2⬍0.001, F lated to response inhibition in the whole sample and to test for P = .96). Most important, the age ⫻medication interac- group differences in baseline activation. The hypotheses relat- tion predictor entered in step 3 did not account for a sig- ing activation changes and symptomatic improvement weretested using a multiple linear regression model that partially nificant proportion of additional variance in sympto- parceled out practice effects. The posttreatment minus base- matic improvement (R2= 0.003, F1,32=0.10, P=.76).
line contrast maps of all the participants were entered into ageneral linear model with 3 regressors: (1) the centered ADHD- BASELINE NEURAL ACTIVATION
RS-IV change score, (2) the centered medication type, and (3)an interaction predictor, which was the product of the dichoto- Successful response inhibition at baseline activated a fron- mous medication type variable with the ADHD-RS-IV change toparietal network that included the bilateral inferior fron- score. The ADHD-RS-IV change score regressor identified ac- tal gyrus, right middle frontal gyri, bilateral anterior cin- tivation changes that were associated with symptomatic change gulate cortex, inferior parietal lobule, and caudate nucleus across the whole sample and that were, thus, similarly relatedto improvement irrespective of medication type. The medica- and deactivated the right precuneus (P ⬍.005) (eTable tion type regressor functioned as a between-group contrast to 1 and eFigure; http://www.archgenpsychiatry.com). Base- test for differential changes in activation that were indepen- line activation in the left superior parietal and paracen- dent of clinical improvement. Finally, the interaction predic- tral lobules was greater in youth treated with methyl- tor identified activation changes that were differentially re- phenidate than in those treated with atomoxetine lated to symptomatic improvement for methylphenidate and (P ⬍.005) (eTable 2).
atomoxetine (ie, divergent regression slopes). Of note, the medi-cation type regressor and interaction predictor both involved between-group contrasts that subtract out activation changes OF SYMPTOMATIC IMPROVEMENT
shared by the 2 groups of youth with ADHD, including prac-tice, expectation, and other nonspecific factors.
The resultant voxelwise statistical maps were thresholded Multiple linear regression revealed that clinical improve- for significance using a cluster size algorithm that protects against ment was associated with both common and unique changes false-positive results.36 The height (intensity) threshold of each in neural activation for atomoxetine and methylpheni- ARCH GEN PSYCHIATRY/ VOL 69 (NO. 9), SEP 2012 2012 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a Mt Sinai School Of Medicine User on 09/05/2012

Methylphenidate (n = 18)
Atomoxetine (n = 18)
Parameter Estimates for Change
in Left Motor Cortex Activation
Parameter Estimates for Change
in Right Motor Cortex Activation
ADHD-RS-IV Change Score
ADHD-RS-IV Change Score
Figure 3. Common therapeutic action of methylphenidate hydrochloride and atomoxetine hydrochloride treatments for attention-deficit/hyperactivity disorder
(ADHD). A, Symptomatic improvements with methylphenidate and atomoxetine use were associated with reductions in bilateral motor cortex activation in youth
with ADHD (n = 18 each). Results are displayed at P ⬍.005 uncorrected, with a cluster threshold of greater than 100 contiguous voxels. B, Parameter estimates for
left and right motor cortex signal change during treatment are plotted against percentage improvement in ratings on the ADHD Rating Scale-IV-Parent Version
(ADHD-RS-IV change score). Parameter estimates were extracted from 8-mm-radius spheres centered at the peaks of maximal activation. Noncentered
ADHD-RS-IV change scores are plotted for clarity. Regression lines in each scatterplot correspond to the lines of best fit.
Table 3. Brain Regions Showing Common and Differential Changes in Neural Activation Related to Symptomatic
Improvement for the Methylphenidate (n = 18) and Atomoxetine (n = 18) Groups
Relation to
Brain Region
Right primary motor cortex
Left primary motor cortex
Differential changes
Right inferior frontal gyrus
Left anterior cingulate cortex
Left supplementary motor area
Bilateral posterior cingulate cortex
Abbreviations: ADHD, attention-deficit hyperactivity disorder; ADHD-RS-IV, ADHD Rating Scale-IV-Parent Version; ATX, atomoxetine hydrochloride;
MPH, methylphenidate hydrochloride.
a Coordinates of peak activation based on the Montreal Neurological Institute stereotactic coordinate system.
b Number of voxels. One voxel = 8 mm3.
c Arrows denote the direction of the relationship between activation and ADHD-RS-IV change score for the MPH and ATX groups: ↑, positive; ↓, negative.
d One cluster with 2 separate peaks.
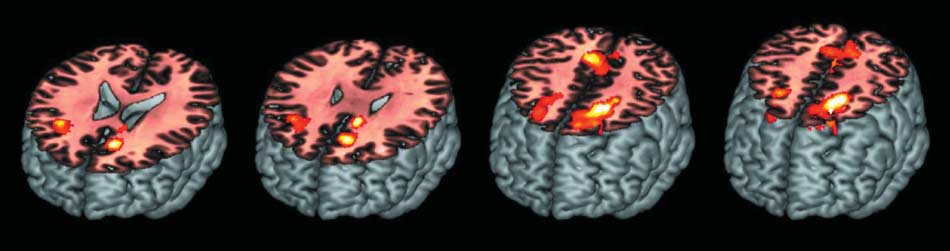
date treatment (Figure 3 and Table 3). The ADHD-
moxetine treatment and reductions in activation in these
RS-IV change score regressor identified corresponding re-
same regions with methylphenidate treatment (P ⬍.005
gions of the right and left motor cortices in which decreases
for all) (Figure 4B). There was no evidence that changes
in activation were associated with symptomatic improve-
in striatal activation were associated with improvement
ment irrespective of the treatment (P⬍.005). Greater symp-
in either the whole sample or the 2 treatment groups sepa-
tomatic improvement was seen in youth who showed larger
rately, even when a small volume correction was used
reductions in the magnitude of activation in the motor cor-
to account for the small size of striatal structures.
tex during treatment (Figure 3B). This relationship be-tween activation and improvement was independent ofmedication type. In contrast, the medication type regres-
sor detected no differential changes in activation that wereindependent of clinical improvement.
These findings provide the first evidence, to our knowl-
The interaction term identified several frontoparietal
edge, of distinct frontoparietal therapeutic mechanisms of
regions that showed differential changes in activation re-
action for stimulant and nonstimulant treatments in youth
lated to clinical improvement with the use of methyl-
with ADHD. Comparable improvements in response in-
phenidate vs atomoxetine (Figure 4 and Table 3). Symp-
hibition and ADHD symptoms were seen after 6 to 8 weeks
tomatic improvement was related to gains in the
of daily treatment with methylphenidate vs atomoxetine.
magnitude of activation in the right inferior frontal gy-
Symptomatic improvement was divergently associated with
rus, left anterior cingulate cortex/supplementary motor
gains in task-related activation for atomoxetine and reduc-
area, and bilateral posterior cingulate cortex with ato-
tions in activation for methylphenidate in the right infe-
ARCH GEN PSYCHIATRY/ VOL 69 (NO. 9), SEP 2012
2012 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a Mt Sinai School Of Medicine User on 09/05/2012
Methylphenidate (n = 18)Atomoxetine (n = 18)
Parameter Estimates for Change
in Inferior Fronal Gyrus Activation
Parameter Estimates for Change
Parameter Estimates for Change
in Anterior Cingulate Cortex Activation
in Posterior Cingulate Cortex Activation
ADHD-RS-IV Change Score
ADHD-RS-IV Change Score
ADHD-RS-IV Change Score
Figure 4. Unique therapeutic actions of methylphenidate and atomoxetine treatments for attention-deficit/hyperactivity disorder (ADHD). A, Symptom
improvement was differentially related to gains in activation for the atomoxetine hydrochloride group and reductions in activation for the methylphenidate
hydrochloride group in the right inferior frontal gyrus, left anterior cingulate/supplementary motor area, and bilateral posterior cingulate cortex in youth with ADHD
(n = 18 each). Results are displayed at P ⬍.005 uncorrected, with a cluster threshold at greater than 100 contiguous voxels. L indicates left; and R, right.
B, Parameter estimates for signal change during treatment in the right inferior frontal gyrus, left anterior cingulate cortex/supplementary motor area, and bilateral
posterior cingulate cortex are plotted against percentage improvement in ratings on the ADHD Rating Scale-IV-Parent Version (ADHD-RS-IV change score).
Parameter estimates were extracted from 8-mm-radius spheres centered at the peaks of maximal activation. Noncentered ADHD-RS-IV change scores are plotted
for clarity. Regression lines in each scatterplot correspond to the lines of best fit.
rior frontal gyrus, left anterior cingulate/supplementary mo-
methylphenidate to produce comparable changes in the
tor area, and bilateral posterior cingulate cortex. These
intracortical facilitation and inhibition of motor activ-
results confirm the importance of medial and lateral pre-
ity.38 Several weeks of methylphenidate treatment has been
frontal inhibitory mechanisms to the therapeutic actions
found to normalize deficient motor cortex inhibition in
of both methylphenidate and atomoxetine but also indi-
children with ADHD, with an increase in inhibition cor-
cate that different processes in these regions underlie re-
related with clinical improvement.39 The therapeutic re-
sponse to the 2 treatments. Results also suggest a unique
ductions in motor cortex activation in the present study
contribution of posterior cingulate cortex deactivation to
may, therefore, reflect attenuation in the prepotency of
the therapeutic actions of methylphenidate that may re-
the inhibited responses. At the same time, the lack of a
flect the suppression of task-independent activity linked
between-group contrast for the ADHD-RS-IV change score
to distractibility. These frontoparietal mechanisms have been
regressor in the present study, plus the absence of pla-
implicated in the pathophysiology of ADHD and poten-
cebo control conditions in previous studies of motor cor-
tially represent the neurophysiologic basis of differential
tex,38,39 makes it impossible to conclusively ascribe this
response to ADHD treatments reported in the literature.4
attenuation in motor prepotency to the therapeutic ac-
In contrast, the comparable improvement-related reduc-
tions of the 2 medications, as opposed to practice, ex-
tions seen in motor cortex activation with methylpheni-
pectation, and other nonspecific factors shared by youth
date and atomoxetine treatment may represent a common
treated with methylphenidate and those treated with ato-
therapeutic mechanism that could account for the obser-
moxetine. The potential for this motor cortex mecha-
vation that many individuals respond to multiple ADHD
nism to serve as a therapeutic target for a broad range of
future interventions merits further investigation in pla-
The common therapeutic actions of methylpheni-
date and atomoxetine on motor cortex activation may re-
The divergent therapeutic effects of methylphenidate and
flect direct pharmacologic actions at catecholamine trans-
atomoxetine on inferior frontal activation indicate that clini-
porters. Moderate levels of both DAT and NET are
cal improvement is not solely attributable to the direct phar-
expressed in the motor cortex15,19 and may provide the
macologic actions of medication. Challenge doses of both
substrate for single-challenge doses of atomoxetine and
methylphenidate and atomoxetine block the same promis-
ARCH GEN PSYCHIATRY/ VOL 69 (NO. 9), SEP 2012
2012 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a Mt Sinai School Of Medicine User on 09/05/2012
cuous NET and produce comparable increases in extra-
The lack of evidence in this study implicating stria-
cellular catecholamine levels in the prefrontal cortex,12-14
tum in the therapeutic actions of methylphenidate
which indirectly modulates event-related prefrontal acti-
treatment is surprising given the robust acute effects
vation,5,7,8,11 likely via dopamine D1 receptors and ␣2-
that stimulants have on striatal dopamine function.
adrenoceptors.9 However, long-term administration of
Single therapeutic doses of methylphenidate produce
atomoxetine but not methylphenidate was found to at-
robust increases in extracellular dopamine levels,57,58
tenuate the prefrontal noradrenergic response to chal-
which potentiate corticostriatal inputs,59 and have been
lenge.40 The divergent inferior frontal actions of the treat-
found to enhance striatal activation in children with
ments would, therefore, seem to reflect differences in
ADHD.6-8 However, repeated surges in extracellular
functional adaptations of NET, ␣2-adrenoceptors, and/or
dopamine over weeks of daily methylphenidate treat-
downstream signal mechanisms (eg, cyclic adenosine
ment have been shown to trigger adaptive downregula-
monophosphate). These results suggest that improve-
tions in neuronal activity,60,61 dopamine synthesis,62
ment of ADHD symptoms involves more than acute cat-
and DAT binding,22 all of which could have blunted fur-
echolamine transporter and/or receptor actions.
ther stimulant-induced dopamine release40 and may ac-
The present findings, nevertheless, suggest that infe-
count for the lack of effect for methylphenidate treat-
rior frontal and anterior cingulate mechanisms serve an im-
ment on striatal activation in this and the few other
portant role in the therapeutic actions of atomoxetine. The
available treatment studies.24,25 Nevertheless, it is pos-
inferior frontal gyrus, particularly in the right hemi-
sible that the actions of methylphenidate in striatum
sphere, is purported to be a neural effector for response in-
may have contributed to clinical improvement by influ-
hibition41,42 and to exert inhibitory control over the pri-
encing activation in other critical regions (eg, the pos-
mary motor, supplementary motor, and premotor
terior cingulate cortex63).
cortices.43,44 Gains in this inferior frontal activation may have
The divergent effects of atomoxetine and methylphe-
contributed to the improvements in response inhibition seen
nidate treatment in association with clinical improve-
in this and other studies with atomoxetine therapy.10,45,46
ment highlight the importance of adopting a network-
The anterior cingulate cortex forms a separate network that
based framework to understand medication-related
has been implicated in the top-down control of volitional
changes in regional activation. Clinical improvement in-
behavior,47 including the implementation of these task sets
volved changes in activation in the same direction (ie,
in downstream sensorimotor processors,48 and has been
increases for atomoxetine and decreases for methylphe-
shown to interact with inferior frontal gyrus during go/
nidate) in the inferior frontal gyrus/anterior cingulate cor-
no-go tasks.49 These anterior cingulate and inferior fron-
tex and posterior cingulate cortex, regions that gener-
tal mechanisms have been implicated in the inhibitory and
ally operate in opposition to each other during optimal
executive deficits that are central to the pathophysiology
behavioral performance.53 For atomoxetine, these changes
of ADHD.50,51 The present results suggest that the benefi-cial actions of atomoxetine involve a gain in inhibitory ef-
suggest that the therapeutic increases in prefrontal acti-
fort and top-down control of attention,52 with a coinci-
vation engendered homeostatic gains in posterior cin-
dent amelioration of the frequently reported prefrontal
gulate activity. Conversely, the therapeutic deactivation of
hypoactivation.50,51 The improvement-related reductions in
posterior cingulate cortex by methylphenidate may have
prefrontal activation for methylphenidate would seem para-
reduced the need for prefrontal inhibitory activation. The
doxical and may reflect the indirect actions of the medi-
comparable changes in frontal and parietal activation as-
cation in interconnected brain regions (eg, the posterior
sociated with clinical improvement for each treatment may
have addressed the functional disconnection of anterior and
The divergent therapeutic effects of the 2 treatments on
posterior cingulate cortices that has been reported in pa-
posterior cingulate activation conversely provide clues re-
tients with ADHD.64 Yet, these improvement-related changes
garding the mechanisms of action for methylphenidate.
in activation were accompanied by improvements in re-
Moderate levels of DAT expression in the posterior cingu-
sponse consistency (ie, standard deviation of RT) that are
late offer the pharmacologic substrate for methylpheni-
more commonly seen when frontal and parietal regions are
date to directly enhance deactivation and, thereby, pro-
activated in opposition to each other.65
duce clinical improvement.15 This enhanced posterior
The unique focus of this study on the differential ef-
cingulate deactivation is consistent with findings from
fects of stimulant and nonstimulant treatments for ADHD,
single-dose challenge studies of methylphenidate11,18 and
together with an innovative analytic approach that in-
potentially represents the neurobiological basis for sup-
corporated clinical improvement and changes in brain
pression of distracting mental processes with treat-
activity, provides a window into the possible neurophysi-
ment.16,54 The reductions in posterior cingulate interfer-
ologic mechanisms of differential response. To summa-
ence may have improved neural efficiency and, thereby,
rize, effective treatment with methylphenidate and ato-
diminished the need for prefrontal inhibitory effort,55 which
moxetine produces a variety of direct, indirect, and
could have accounted for the improvement-related de-
downstream effects on neural activation during re-
creases in inferior frontal and anterior cingulate activa-
sponse inhibition via a common mechanism in motor cor-
tion for methylphenidate. In contrast, the sparse density
tex and distinct mechanisms in frontoparietal regions.
of NET sites for atomoxetine to directly affect posterior cin-
These findings provide a neurobiological basis for un-
gulate activation suggests that the observed gain in activa-
derstanding selective response to the 2 classes of medi-
tion may reflect the downstream effects of excitatory infe-
cation, which represents an important first step in match-
rior frontal and anterior cingulate actions of treatment.56
ing treatments to individual patients.
ARCH GEN PSYCHIATRY/ VOL 69 (NO. 9), SEP 2012
2012 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a Mt Sinai School Of Medicine User on 09/05/2012
Submitted for Publication: August 1, 2011; final revision
disorder: a functional magnetic resonance study. Proc Natl Acad Sci U S A. 1998;
received November 24, 2011; accepted December 2, 2011.
9. Gamo NJ, Wang M, Arnsten AF. Methylphenidate and atomoxetine enhance pre-
Correspondence: Jeffrey H. Newcorn, MD, Department
frontal function through ␣2-adrenergic and dopamine D1 receptors. J Am Acad
of Psychiatry, Mount Sinai School of Medicine, One
Child Adolesc Psychiatry. 2010;49(10):1011-1023.
Gustave L Levy Pl, PO Box 1230, New York, NY 10029.
10. Chamberlain SR, Mu¨ller U, Blackwell AD, Clark L, Robbins TW, Sahakian BJ.
Author Contributions: Dr Schulz performed the statis-
Neurochemical modulation of response inhibition and probabilistic learning in
tical analyses for the study and takes responsibility for
11. Marquand AF, De Simoni S, O'Daly OG, Williams SC, Moura˜o-Miranda J, Mehta
the integrity of the data and the accuracy of the data analy-
MA. Pattern classification of working memory networks reveals differential ef-
sis. Drs Schulz, Be´dard, and Newcorn had full access to
fects of methylphenidate, atomoxetine, and placebo in healthy volunteers.
all the data in the study.
Financial Disclosure: Dr Newcorn is a recipient of grants
12. Bymaster FP, Katner JS, Nelson DL, Hemrick-Luecke SK, Threlkeld PG, Heili-
for research support from Eli Lilly & Co, Ortho-McNeil-
genstein JH, Morin SM, Gehlert DR, Perry KW. Atomoxetine increases extracel-lular levels of norepinephrine and dopamine in prefrontal cortex of rat: a poten-
Janssen, and Shire and is or has been an advisor/
tial mechanism for efficacy in attention deficit/hyperactivity disorder.
consultant for Alcobra, Biobehavioral Diagnostics, Eli Lilly
& Co, Ortho-McNeil-Janssen, and Shire. Dr Newcorn is
13. Berridge CW, Devilbiss DM, Andrzejewski ME, Arnsten AF, Kelley AE, Schmei-
now a member of the advisory boards for NEOS, Ot-
chel B, Hamilton C, Spencer RC. Methylphenidate preferentially increases cat-echolamine neurotransmission within the prefrontal cortex at low doses that en-
suka, and Shionogi.
hance cognitive function. Biol Psychiatry. 2006;60(10):1111-1120.
Funding/Support: This study was supported by research
14. Moro´n JA, Brockington A, Wise RA, Rocha BA, Hope BT. Dopamine uptake through
the norepinephrine transporter in brain regions with low levels of the dopamine
(Dr Newcorn), and K01 MH070892 (Dr Schulz) from the
transporter: evidence from knock-out mouse lines. J Neurosci. 2002;22(2):
National Institutes of Health; by grant UL1RR029887 from
15. Lewis DA, Melchitzky DS, Sesack SR, Whitehead RE, Auh S, Sampson A. Dopa-
the National Center for Research Resources, a component
mine transporter immunoreactivity in monkey cerebral cortex: regional, lami-
of the National Institutes of Health; and by research grant
nar, and ultrastructural localization. J Comp Neurol. 2001;432(1):119-136.
B4Z-US-X012 from Eli Lilly & Co (Dr Newcorn).
16. Fassbender C, Zhang H, Buzy WM, Cortes CR, Mizuiri D, Beckett L, Schweitzer
Role of the Sponsors: The funding sources had no role in
JB. A lack of default network suppression is linked to increased distractibility in
the design or conduct of the study; collection, management,
ADHD. Brain Res. 2009;1273:114-128.
17. Peterson BS, Potenza MN, Wang Z, Zhu H, Martin A, Marsh R, Plessen KJ, Yu
analysis, or interpretation of the data; or preparation, re-
S. An FMRI study of the effects of psychostimulants on default-mode process-
view, or approval of the manuscript. The contents of this
ing during Stroop task performance in youths with ADHD. Am J Psychiatry. 2009;
article are solely the responsibility of the authors.
Additional Contributions: The baseline MRIs from a sub-
18. Tomasi D, Volkow ND, Wang GJ, Wang R, Telang F, Caparelli EC, Wong C, Jayne
set of the sample described in this article were used in a
M, Fowler JS. Methylphenidate enhances brain activation and deactivation re-sponses to visual attention and working memory tasks in healthy controls.
previous publication.33
Online-Only Material: The eTables and eFigure are avail-
19. Seneca N, Gulya´s B, Varrone A, Schou M, Airaksinen A, Tauscher J, Vanden-
able at http://www.archgenpsychiatry.com.
hende F, Kielbasa W, Farde L, Innis RB, Halldin C. Atomoxetine occupies the nor-epinephrine transporter in a dose-dependent fashion: a PET study in nonhumanprimate brain using (S,S)-[18F]FMeNER-D2. Psychopharmacology (Berl). 2006;
20. Sasane´ R, Hodgkins P, Meijer W. Treatment stabilization in children and ado-
1. Winterstein AG, Gerhard T, Shuster J, Zito J, Johnson M, Liu H, Saidi A. Utiliza-
lescents with attention-deficit/hyperactivity disorder: data from the Netherlands.
tion of pharmacologic treatment in youths with attention deficit/hyperactivity dis-
Curr Med Res Opin. 2010;26(11):2565-2574.
order in Medicaid database. Ann Pharmacother. 2008;42(1):24-31.
21. Newcorn JH, Sutton VK, Weiss MD, Sumner CR. Clinical responses to atomoxetine
2. Gatley SJ, Pan D, Chen R, Chaturvedi G, Ding YS. Affinities of methylphenidate
in attention-deficit/hyperactivity disorder: the Integrated Data Exploratory Analysis
derivatives for dopamine, norepinephrine and serotonin transporters. Life Sci.
(IDEA) study. J Am Acad Child Adolesc Psychiatry. 2009;48(5):511-518.
22. Dresel S, Krause J, Krause KH, LaFougere C, Brinkba¨umer K, Kung HF, Hahn K,
3. Bolden-Watson C, Richelson E. Blockade by newly-developed antidepressants
Tatsch K. Attention deficit hyperactivity disorder: binding of [99mTc]TRODAT-1
of biogenic amine uptake into rat brain synaptosomes. Life Sci. 1993;52(12):
to the dopamine transporter before and after methylphenidate treatment. Eur J
Nucl Med. 2000;27(10):1518-1524.
4. Newcorn JH, Kratochvil CJ, Allen AJ, Casat CD, Ruff DD, Moore RJ, Michelson
23. Lee JS, Kim BN, Kang E, Lee DS, Kim YK, Chung JK, Lee MC, Cho SC. Regional
D; Atomoxetine/Methylphenidate Comparative Study Group. Atomoxetine and os-
cerebral blood flow in children with attention deficit hyperactivity disorder: com-
motically released methylphenidate for the treatment of attention deficit hyper-
parison before and after methylphenidate treatment. Hum Brain Mapp. 2005;
activity disorder: acute comparison and differential response. Am J Psychiatry.
24. Schweitzer JB, Lee DO, Hanford RB, Zink CF, Ely TD, Tagamets MA, Hoffman
5. Chamberlain SR, Hampshire A, Mu¨ller U, Rubia K, Del Campo N, Craig K, Re-
JM, Grafton ST, Kilts CD. Effect of methylphenidate on executive functioning in
genthal R, Suckling J, Roiser JP, Grant JE, Bullmore ET, Robbins TW, Sahakian
adults with attention-deficit/hyperactivity disorder: normalization of behavior but
BJ. Atomoxetine modulates right inferior frontal activation during inhibitory con-
not related brain activity. Biol Psychiatry. 2004;56(8):597-606.
trol: a pharmacological functional magnetic resonance imaging study. Biol
25. Bush G, Spencer TJ, Holmes J, Shin LM, Valera EM, Seidman LJ, Makris N, Sur-
man C, Aleardi M, Mick E, Biederman J. Functional magnetic resonance imaging
6. Rubia K, Halari R, Cubillo A, Smith AB, Mohammad AM, Brammer M, Taylor E.
of methylphenidate and placebo in attention-deficit/hyperactivity disorder dur-
Methylphenidate normalizes fronto-striatal underactivation during interference
ing the multi-source interference task. Arch Gen Psychiatry. 2008;65(1):102-
inhibition in medication-naive boys with attention-deficit hyperactivity disorder.
26. Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, Williamson D, Ryan N.
7. Epstein JN, Casey BJ, Tonev ST, Davidson MC, Reiss AL, Garrett A, Hinshaw
Schedule for Affective Disorders and Schizophrenia for School-Age Children-
SP, Greenhill LL, Glover G, Shafritz KM, Vitolo A, Kotler LA, Jarrett MA, Spicer
Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am
J. ADHD- and medication-related brain activation effects in concordantly af-
Acad Child Adolesc Psychiatry. 1997;36(7):980-988.
fected parent-child dyads with ADHD. J Child Psychol Psychiatry. 2007;48
27. DuPaul GJ, Power TJ, Anastopoulos AD, Reid R. ADHD Rating Scale-IV: Check-
lists, Norms, and Clinical Interpretation. New York, NY: Guilford Press; 1998.
8. Vaidya CJ, Austin G, Kirkorian G, Ridlehuber HW, Desmond JE, Glover GH, Ga-
28. Swanson J, Gupta S, Lam A, Shoulson I, Lerner M, Modi N, Lindemulder E, Wi-
brieli JD. Selective effects of methylphenidate in attention deficit hyperactivity
gal S. Development of a new once-a-day formulation of methylphenidate for the
ARCH GEN PSYCHIATRY/ VOL 69 (NO. 9), SEP 2012
2012 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a Mt Sinai School Of Medicine User on 09/05/2012
treatment of attention-deficit/hyperactivity disorder: proof-of-concept and proof-
48. Dosenbach NU, Fair DA, Miezin FM, Cohen AL, Wenger KK, Dosenbach RA, Fox
of-product studies. Arch Gen Psychiatry. 2003;60(2):204-211.
MD, Snyder AZ, Vincent JL, Raichle ME, Schlaggar BL, Petersen SE. Distinct brain
29. Witcher JW, Long A, Smith B, Sauer JM, Heilgenstein J, Wilens T, Spencer T,
networks for adaptive and stable task control in humans. Proc Natl Acad Sci U S A.
Biederman J. Atomoxetine pharmacokinetics in children and adolescents with
attention deficit hyperactivity disorder. J Child Adolesc Psychopharmacol. 2003;
49. Schulz KP, Be´dard AC, Czarnecki R, Fan J. Preparatory activity and connectivity
in dorsal anterior cingulate cortex for cognitive control. Neuroimage. 2011;
30. Zhang S, Faries DE, Vowles M, Michelson D. ADHD Rating Scale IV: psychomet-
ric properties from a multinational study as a clinician-administered instrument.
50. Aron AR, Poldrack RA. The cognitive neuroscience of response inhibition: rel-
Int J Methods Psychiatr Res. 2005;14(4):186-201.
evance for genetic research in attention-deficit/hyperactivity disorder. Biol
31. Durston S, Thomas KM, Worden MS, Yang Y, Casey BJ. The effect of preceding
context on inhibition: an event-related fMRI study. Neuroimage. 2002;16(2):
51. Bush G, Valera EM, Seidman LJ. Functional neuroimaging of attention-deficit/
hyperactivity disorder: a review and suggested future directions. Biol Psychiatry.
32. Durston S, Tottenham NT, Thomas KM, Davidson MC, Eigsti IM, Yang Y, Ulug
AM, Casey BJ. Differential patterns of striatal activation in young children with
52. Milham MP, Banich MT, Claus ED, Cohen NJ. Practice-related effects demon-
and without ADHD. Biol Psychiatry. 2003;53(10):871-878.
strate complementary roles of anterior cingulate and prefrontal cortices in at-
33. Be´dard AC, Schulz KP, Cook EH Jr, Fan J, Clerkin SM, Ivanov I, Halperin JM,
tentional control. Neuroimage. 2003;18(2):483-493.
Newcorn JH. Dopamine transporter gene variation modulates activation of stria-
53. Uddin LQ, Kelly AM, Biswal BB, Xavier Castellanos F, Milham MP. Functional con-
tum in youth with ADHD. Neuroimage. 2010;53(3):935-942.
nectivity of default mode network components: correlation, anticorrelation, and
34. Friston KJ, Fletcher P, Josephs O, Holmes A, Rugg MD, Turner R. Event-related
causality. Hum Brain Mapp. 2009;30(2):625-637.
fMRI: characterizing differential responses. Neuroimage. 1998;7(1):30-40.
54. Mason MF, Norton MI, Van Horn JD, Wegner DM, Grafton ST, Macrae CN.
35. Johnstone T, Ores Walsh KS, Greischar LL, Alexander AL, Fox AS, Davidson RJ,
Wandering minds: the default network and stimulus-independent thought. Science.
Oakes TR. Motion correction and the use of motion covariates in multiple-
subject fMRI analysis. Hum Brain Mapp. 2006;27(10):779-788.
55. Volkow ND, Fowler JS, Wang GJ, Telang F, Logan J, Wong C, Ma J, Pradhan K,
36. Hayasaka S, Phan KL, Liberzon I, Worsley KJ, Nichols TE. Nonstationary cluster-
Benveniste H, Swanson JM. Methylphenidate decreased the amount of glucose
size inference with random field and permutation methods. Neuroimage. 2004;
needed by the brain to perform a cognitive task. PLoS One. 2008;3(4):e2017.
56. Smith HR, Beveridge TJ, Porrino LJ. Distribution of norepinephrine transport-
37. Slotnick SD, Schacter DL. A sensory signature that distinguishes true from false
ers in the non-human primate brain. Neuroscience. 2006;138(2):703-714.
memories. Nat Neurosci. 2004;7(6):664-672.
57. Volkow ND, Wang GJ, Fowler JS, Logan J, Franceschi D, Maynard L, Ding YS,
38. Gilbert DL, Ridel KR, Sallee FR, Zhang J, Lipps TD, Wassermann EM. Compari-
Gatley SJ, Gifford A, Zhu W, Swanson JM. Relationship between blockade of dopa-
son of the inhibitory and excitatory effects of ADHD medications methylpheni-date and atomoxetine on motor cortex. Neuropsychopharmacology. 2006;
mine transporters by oral methylphenidate and the increases in extracellular dopa-
mine: therapeutic implications. Synapse. 2002;43(3):181-187.
39. Buchmann J, Gierow W, Weber S, Hoeppner J, Klauer T, Benecke R, Haessler F,
58. Volkow ND, Wang G, Fowler JS, Logan J, Gerasimov M, Maynard L, Ding Y, Gat-
Wolters A. Restoration of disturbed intracortical motor inhibition and facilitation
ley SJ, Gifford A, Franceschi D. Therapeutic doses of oral methylphenidate sig-
in attention deficit hyperactivity disorder children by methylphenidate. Biol
nificantly increase extracellular dopamine in the human brain. J Neurosci. 2001;
40. Koda K, Ago Y, Cong Y, Kita Y, Takuma K, Matsuda T. Effects of acute and chronic
59. Bamford NS, Zhang H, Schmitz Y, Wu NP, Cepeda C, Levine MS, Schmauss C,
administration of atomoxetine and methylphenidate on extracellular levels of nor-
Zakharenko SS, Zablow L, Sulzer D. Heterosynaptic dopamine neurotransmis-
adrenaline, dopamine and serotonin in the prefrontal cortex and striatum of mice.
sion selects sets of corticostriatal terminals. Neuron. 2004;42(4):653-663.
J Neurochem. 2010;114(1):259-270.
60. Chase TD, Brown RE, Carrey N, Wilkinson M. Daily methylphenidate adminis-
41. Garavan H, Hester R, Murphy K, Fassbender C, Kelly C. Individual differences in
tration attenuates c-fos expression in the striatum of prepubertal rats. Neuroreport.
the functional neuroanatomy of inhibitory control. Brain Res. 2006;1105(1):
61. Allen JK, Wilkinson M, Soo EC, Hui JP, Chase TD, Carrey N. Chronic low dose
42. Xue G, Aron AR, Poldrack RA. Common neural substrates for inhibition of spo-
Adderall XR down-regulates cfos expression in infantile and prepubertal rat stria-
ken and manual responses. Cereb Cortex. 2008;18(8):1923-1932.
tum and cortex. Neuroscience. 2010;169(4):1901-1912.
43. Duann JR, Ide JS, Luo X, Li CS. Functional connectivity delineates distinct roles
62. Gray JD, Punsoni M, Tabori NE, Melton JT, Fanslow V, Ward MJ, Zupan B, Men-
of the inferior frontal cortex and presupplementary motor area in stop signal
zer D, Rice J, Drake CT, Romeo RD, Brake WG, Torres-Reveron A, Milner TA.
inhibition. J Neurosci. 2009;29(32):10171-10179.
Methylphenidate administration to juvenile rats alters brain areas involved in cog-
44. Stevens MC, Kiehl KA, Pearlson GD, Calhoun VD. Functional neural networks un-
nition, motivated behaviors, appetite, and stress. J Neurosci. 2007;27(27):
derlying response inhibition in adolescents and adults. Behav Brain Res. 2007;
63. Tomasi D, Volkow ND, Wang R, Telang F, Wang GJ, Chang L, Ernst T, Fowler
45. Chamberlain SR, Robbins TW, Winder-Rhodes S, Mu¨ller U, Sahakian BJ, Black-
JS. Dopamine transporters in striatum correlate with deactivation in the default
well AD, Barnett JH. Translational approaches to frontostriatal dysfunction in at-
mode network during visuospatial attention. PLoS One. 2009;4(6):e6102.
tention-deficit/hyperactivity disorder using a computerized neuropsychological
64. Castellanos FX, Margulies DS, Kelly C, Uddin LQ, Ghaffari M, Kirsch A, Shaw D,
battery. Biol Psychiatry. 2011;69(12):1192-1203.
Shehzad Z, Di Martino A, Biswal B, Sonuga-Barke EJ, Rotrosen J, Adler LA, Mil-
46. Chamberlain SR, Del Campo N, Dowson J, Mu¨ller U, Clark L, Robbins TW, Sa-
ham MP. Cingulate-precuneus interactions: a new locus of dysfunction in adult
hakian BJ. Atomoxetine improved response inhibition in adults with attention deficit/
attention-deficit/hyperactivity disorder. Biol Psychiatry. 2008;63(3):332-337.
hyperactivity disorder. Biol Psychiatry. 2007;62(9):977-984.
65. Kelly AM, Uddin LQ, Biswal BB, Castellanos FX, Milham MP. Competition be-
47. Paus T. Primate anterior cingulate cortex: where motor control, drive and cog-
tween functional brain networks mediates behavioral variability. Neuroimage. 2008;
nition interface. Nat Rev Neurosci. 2001;2(6):417-424.
ARCH GEN PSYCHIATRY/ VOL 69 (NO. 9), SEP 2012
2012 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a Mt Sinai School Of Medicine User on 09/05/2012
Source: http://people.qc.cuny.edu/Faculty/Jin.Fan/Documents/Schulz_2012_69.pdf
"clevinger, the corporal, and colonel korn agreed that it was neither possible nor necessary to educate people who never questioned anything
"For the moment let us note that getting the better of words in writing is commonly a very hard struggle."–H.G. Widdowson Spring 2012 ENG 101- Section 428 Office Hours: W 2-5 Percival Hall 314A Writing for Others This class intends to help you strengthen your composition skills for academic, professional, and personal purposes. The course will have three main focuses: 1) language's role in constructing the world, 2) audience awareness, and 3) classical rhetoric. These are some of the most important things for writers to be aware of, and while most good writers internalize these components of composition we will consciously analyze, discuss, and use them to achieve our four official Course Goals: 1) Know the Context, 2) Think Critically, 3) Learn Processes for Writing, Revision, and Reflection, and 4) Know the Rules. These goals are explained in WiP pages xvi-xvii, and we will discuss them extensively in class.
Lieti carta 2013
CENTRO DIAGNOSTICO CARTA DEI SERVIZI Carta dei servizi redatta ai sensi: del DPCM del 19 maggio 1995 "Schema generale di riferimento della Carta dei servizi pubblici sanitari", del DGRC n° 369 del 23 marzo 2010 "Linee Guida per La Carta Dei Servizi Sanitari" e del DGRC n° 2100 del 31 dicembre 2008. Verificata da Responsabile Qualità