Clinicadepele.com.br

Review Article
Types of Hair Loss and Treatment Options,Including the Novel Low-Level Light Therapyand Its Proposed MechanismMahyar Ghanaat, MD
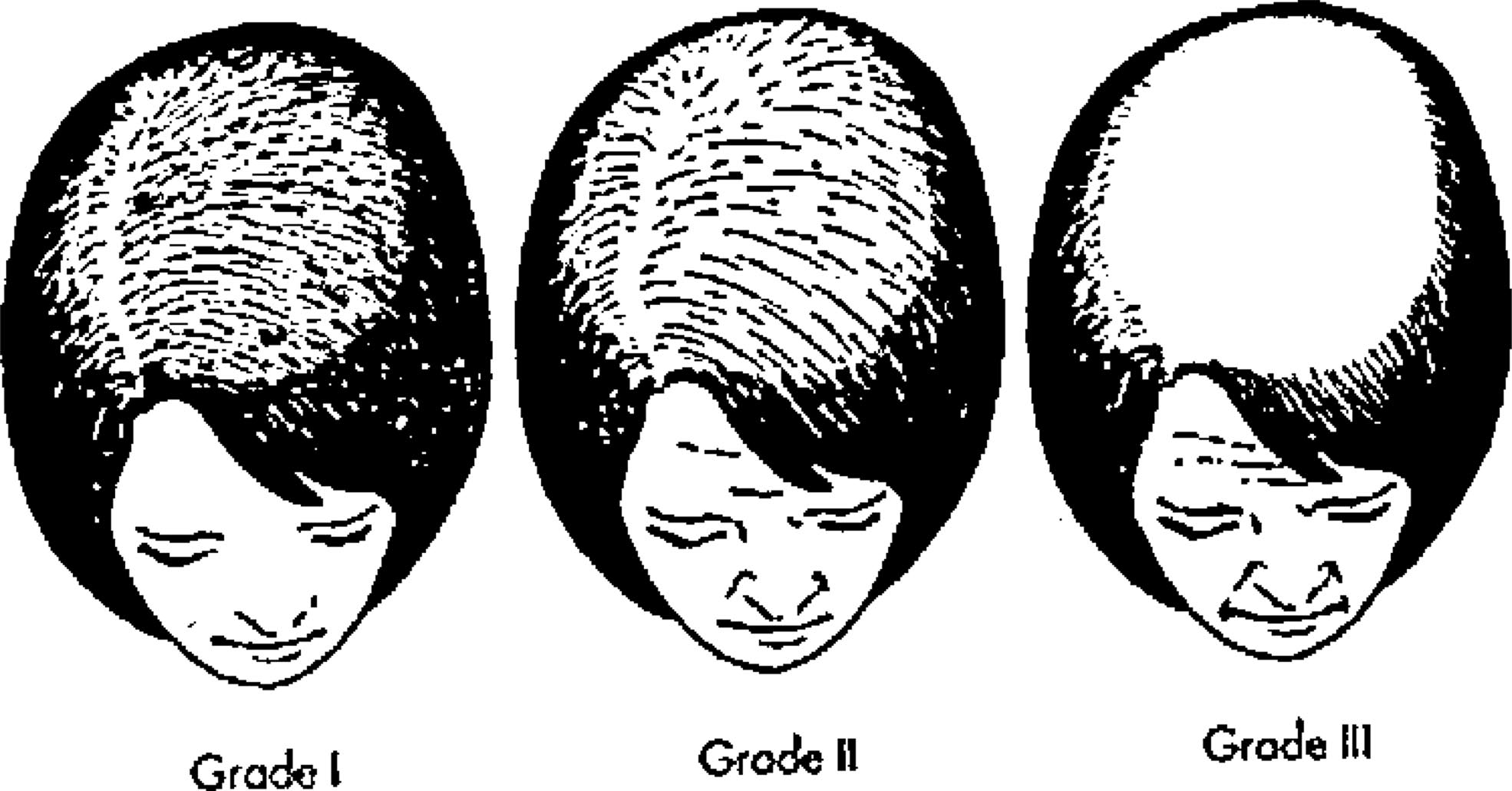
evaluated based on the Ludwig scale, which ranges from I-III
Abstract: Androgenetic alopecia (AGA) is the most common form
(Fig. 2).4 These classification systems differ based on the fact
of hair loss in men, and female pattern hair loss (FPHL) is the most
that hair loss and thinning in men most commonly occurs in
common form of hair loss in women. Traditional methods of treating
an orderly fashion and involves the temporal and vertex re-
hair loss have included minoxidil, finasteride, and surgical trans-
gion while sparing the occipital region; diffuse thinning and
plantation. Currently there is a myriad of new and experimental
loss of density with a normal distribution and maintenance of
treatments. In addition, low-level light therapy (LLLT) has recently
the frontal hairline is often seen in women.2,4,5,9,10
been approved by the United States Food and Drug Administration
The term AGA pertains to the pathophysiology of MPHL,
(FDA) for the treatment of hair loss. There are several theories and
in which there is an induction of hair loss due to the effects
minimal clinical evidence of the safety and efficacy of LLLT, al-
of androgens such as testosterone (T) and its derivative di-
though most experts agree that it is safe. More in vitro studies are
hydrotestosterone (DHT) in genetically susceptible individu-
necessary to elucidate the mechanism and effectiveness at the cel-
als.2 Recently, authors have argued against the use of the term
lular level, and more controlled studies are necessary to assess the
AGA in women, as the role of androgens in FPHL is debat-
role of this new treatment in the general population.
able.4,7,11,12 Testosterone is a lipophilic compound that dif-
Key Words: fibroblast, hair growth, hair loss, low level laser ther-
fuses the cell membrane. It is converted into its more active
apy, low-level light therapy
form, DHT, by the cytoplasmic enzyme 5-alpha reductase(5-AR).2,4 There are two types of 5-AR. Type 1 is found in
Types and Epidemiology of Hair Loss
keratinocytes, fibroblasts, sweat glands, and sebocytes, and
Male pattern hair loss (MPHL), also known as androge-
Type 2 is found in skin and the inner root sheath of hair
netic alopecia (AGA), is the most common form of hair loss
follicles.4,13,14 Androgens play an important role in the con-
in men.1–3 Similarly, female pattern hair loss (FPHL) is the
trol of hair. During puberty, due to a surge in T, there is an
most common form of hair loss in women.4 The incidence
induction of pubic hair growth and a decrease in follicle size
and prevalence of MPHL is dependent on age and race. Chi-
in the bitemporal region.8 Also, castrated men are not known
nese, Japanese, and African American people are affected
to develop MPHL.2,7 However, there is no correlation be-
less than Caucasians.2,5 Its incidence increases by age.5 Prev-
tween T levels and MPHL.2 The role of DHT was first no-
alence values have variable ranges from 16 –96%, depending
ticed in pseudohermaphrodites lacking this enzyme, who did
on the age group and whether or not mild forms of MPHL are
not develop MPHL.2,7 DHT then binds the nuclear androgen
included (Table 1).2,6,7 Prevalence values for FPHL are com-
receptor (AR) that regulates gene expression.2,7 Although the
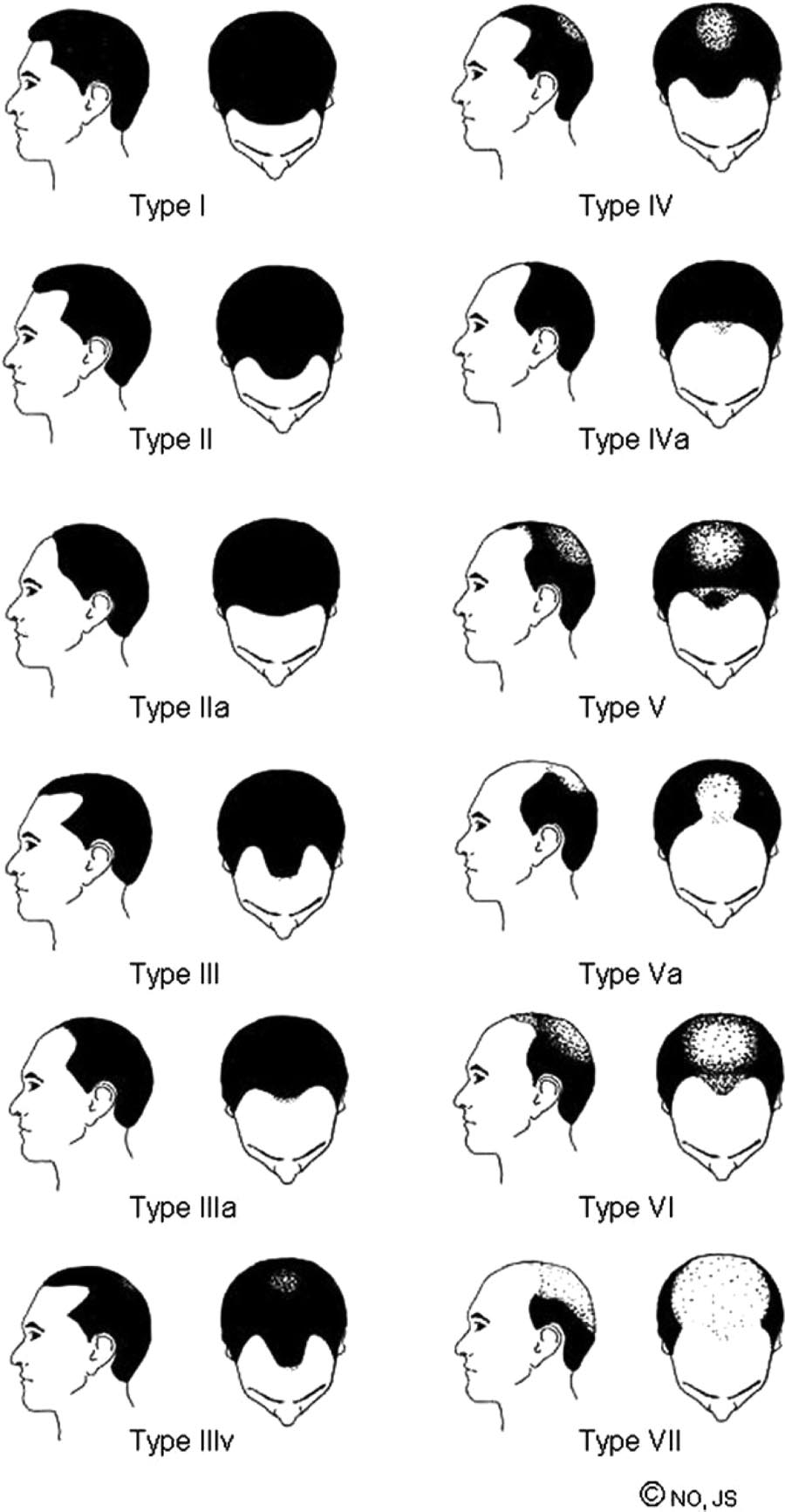
parable to MPHL (Table 2).8 The severity of MPHL is based
exact genes involved in hair loss are not known with cer-
on the Norwood Hamilton Classification, which takes into
tainty, some of the proposed genes responsible for hair growth
account bitemporal and vertex hair loss (Fig. 1).2 FPHL is
(mainly studied in knockout and transgenic mice) are desmo-
From the Department of Dermatology, SUNY Downstate Medical Center,
Brooklyn, NY.
• Low-level light therapy (LLLT) appears safe and ef-
Reprint requests to Mahyar Ghanaat, BS, MD, SUNY Downstate Medical
Center, Box #50, 450 Clarkson Avenue, Brooklyn, NY 11230. Email:
fective for the treatment of hair loss.
• LLLT may serve as an adjunct to other treatment
No authors have any financial support and proprietary interest.
Accepted October 22, 2009.
• More cellular and human research is necessary to elu-
Copyright 2010 by The Southern Medical Association
cidate the mechanism of LLLT.
Southern Medical Journal • Volume 103, Number 9, September 2010

Ghanaat • Low-Level Light Therapy in Hair Loss
Table 1. Prevalence of male pattern hair loss
Not including Type II frontal Hamilton37
Including Type II frontal
recession in Hamilton'sdata37
Including Type II frontal
recession in Norwoods'data38
62% in 20–40 yr olds
Have bitemporal recession
54% of those ⬎30 yrs old
Have androgenetic alopecia
53% of 40–49 yr olds
Have Type III or greater
42% of 18–49 yr olds
Have Type III or greater
16% of 18–29 yr olds
Have Type III or greater
Moderate to severe hair loss
Rhodes study including all
types of hair loss
30% by 30, 50% by 50, and White men
See references for full citation.
glein, activin, epidermal growth factor (EGF), fibroblastgrowth factor (FGF), lymphoid-enhancer factor-1 (LEF-1),and Sonic Hedgehock.15
Besides patterned baldness, there are several other forms
of hair loss, which include alopecia areata (AA), telogen ef-fluvium (TE), and several androgen-related female alopecias.
AA is an autoimmune inflammatory condition which mayaffect the hair of the head, face, and body.16 Although mostcommonly thought of as an acquired disorder, congenitalcases have been described.17 It has an incidence of 0.1– 0.2%,and affects 1–2% of men and women.16,18 Hair involvementin AA is often patchy. Two variants of AA are alopecia
totalis, a total loss of scalp hair, and alopecia universalis, total
Norwood Hamilton classification. Reprinted with per-
mission from Endocrinol Metab Clin North Am 2007;36:381,
loss of scalp and body hair.16 AA is linked to several human
2007 Elsevier Inc. All rights reserved.
leukocyte antigen (HLA) alleles, such as HLA-AI, HLA-HLA-B26, HLA-DQ1, and HLA-DQ3.16 Although most com-monly treated by an injection of intralesional corticosteroids,
and systemic corticosteroids, minoxidil for moderate cases, an-
other treatment modalities are used.16 These include topical
thralin, contact sensitizers (when more than half the scalp isaffected), psoralen plus ultraviolet A (PUVA), cyclosporine, ta-crolimus, and biologics.16,18,19 Biologics include agents such as
Table 2. Prevalence of female pattern hair loss
alefacept, efalizumab, etanercept, infliximab, and adalimumab.
Of these, alefacept seems to be most promising, while adali-mumab and infliximab have been reported to induce AA.20
12% of those 20–29 yr old
Dinh and Sinclair4
Telogen effluvium (TE) is abnormal hair cycling caus-
⬎50% in those ⬎80 yr old
Dinh and Sinclair4
ing excessive loss of telogen hair.12 It is likely the most
common cause of alopecia in children.12 Some of the com-
mon causes include acute severe illness, surgery, iron de-
10% of premenopausal women
ficiency anemia, thyroid disease, malnutrition, chronic ill-
50–75% of women ⬎65 yr old
ness, and medications such as oral contraceptives, lithium,
See References for full citation.
and cimetidine.12,19 A good illness and medication history
2010 Southern Medical Association

have shown the same efficacy with the 5% solution, yet ahigher rate of hypertrichosis with topical application.8,19 Mi-noxidil is effective in adolescents.12
Finasteride is an oral agent, which is a competitive 5-AR
inhibitor with more affinity for Type II 5-AR.8,11,13 Thus, itinhibits the conversion of T to its more active form of DHT.2,4Given its systemic nature, potential side effects of finasterideinclude erectile dysfunction, gynecomastia, and loss of li-bido.1 Like minoxidil, this is an ongoing therapy. Finasterideis only approved for men 18 years of age or older.12
Whereas minoxidil and finasteride are temporizing mea-
Fig. 2 Ludwig classification. Reprinted with permission from
surements and require continuous administration, hair resto-
Clin Interv Aging 2007;2:190, 2007 Dove Medical Press Ltd.
ration may serve as a definitive treatment.2,9 This procedure
All rights reserved.
is based on the fact that occipital hair follicles are not andro-gen dependent, and that transplanted hair maintains donor
is necessary to make the diagnosis, as well as laboratory
dominance.9,22 Follicular units are acquired from the occipital
studies such as complete blood count (CBC), thyroid func-
scalp and transplanted into the frontal scalp in a cosmetically
tion tests, and syphilis titers.12,19
acceptable manner.9,22 This procedure should ideally be per-
Androgen-related female alopecias include a variety of
formed on individuals who have reached a plateau in balding
types of hypergonadism. Polycystic ovarian syndrome
and have realistic expectations.9,22 Side effects are usually
(PCOS) is a common cause of hypergonadism which could
minor and include postoperative pain, delayed hair growth,
cause amenorrhea, hirsutism, and FPHL.14 Some antiandro-
and, rarely, infection.9 Periorbital and frontal swelling may
gen medications that may be helpful for FPHL include cypro-
also occur.22 Some argue that the future procedure of hair
terone acetate, spironolactone, and flutamide.10 However, one
cloning may dramatically improve this process.23
study argues that 88% of FPHL will not improve with oral
In addition, there are a variety of off-label and investi-
gational drugs that are used or considered in the treatment ofhair loss. Dutasteride is a dual Type I and II 5-AR inhibitor.4,7
Traditional Treatment Options
Latanoprost is a prostaglandin mainly used for glaucoma,
The two medications approved for MPHL by the United
which was observed to stimulate eyelash and eyebrow
States Food and Drug Administration (FDA) are 5% minoxi-
growth.7 The antifungal agent ketoconazole may also pro-
dil and finasteride.2,3,19 Two percent minoxidil is the only
mote hair growth, perhaps by inhibiting inflammation and
approved medication for FPHL.3,10 Minoxidil is an antihy-
serving as an antiandrogen.7 Other investigational drugs in-
pertensive medication with peripheral vasodilator properties,
clude fluridil, a topical antiandrogen; naminidil, which works
and the side effect when taken systemically is hypertricho-
through the potassium (K) channel; P-45, which may inhibit
sis.1,11 After application, minoxidil is converted to minoxidil
interleukin 4 (I-L4)-induced CD23 expression; PSK 3841, a
sulfate, a potassium channel opener which relaxes vascular
topical nonsteroidal androgen antagonist; and lemuteporfin
smooth muscle and increases blood flow.6 It was first sus-
(QLT 0074), a photosensitizer to be used with photodynamic
pected that this increased blood flow is the mechanism by
therapy.3 Other agents include antiandrogen oligonucleo-
which minoxidil affects hair loss, but this may not be the
tides—which are deoxyribonucleic acid (DNA) that pairs
case.11 In vitro studies of hair growth have shown that hair
with complementary ribonucleic acid (RNA)—KF19418,
cultures grown in the presence of minoxidil maintain mor-
LGD1331, steroid sulfatase inhibitors, and thymosin beta 4,
phology, whereas controls undergo kinking and necrosis.21 A
which stimulates hair growth via stem cell migration.3 Gene
common side effect of minoxidil is contact dermatitis, which
delivery through liposome technology has also showed some
can initially be managed by switching to a 2% solution or the
foam preparation, which lacks propylene glycol (an irritatingsubstance).2 Corticosteroids may also be beneficial to im-prove pruritic side effects.11 One drawback with minoxidil
Low-Level Light Therapy
treatment is that it requires twice daily application indefi-
In 2007, low-level light therapy (LLLT) was approved
nitely to maintain results.1,2,6 Shin et al6 have proposed that
by the FDA as a treatment for hair loss.23 LLLT is also
combination of minoxidil with tretinoin once a day makes no
known as low level laser therapy, red light therapy, cold laser,
significant difference in efficacy or side effect profile (as
soft laser, biostimulation, and photobiomodulation.24–26 Most
opposed to minoxidil twice a day), and may improve patient
experts agree that LLLT is safe for the treatment of hair loss,
compliance. Tretinoin increases the absorption of minoxidil.6
but more studies are needed to confirm its therapeutic ef-
Two percent minoxidil is approved for women, as studies
fects.24 LLLT was discovered in the 1960s and first used by
Southern Medical Journal • Volume 103, Number 9, September 2010

Ghanaat • Low-Level Light Therapy in Hair Loss
the National Aeronautics and Space Administration (NASA)
One study reported a failure in treatment of AA.32 However,
to accelerate wound healing in space.25 Since then, LLLT has
the researchers used a small dose (630 nm at 37 J/cm2 for 7.5
been used to reduce neurogenic pain, reduce inflammation,
min) only once a month.32 In addition, they reported success-
and promote wound healing.25–27 Other uses include non-
ful treatment in beard AA after only three sessions in three
melanoma skin cancer and its precursors, acne vulgaris, pho-
patients.32 Sobanko and Alster25 propose that better under-
torejuvenation, hidradenitis suppurativa, and psoriasis.28 It
standing of the mechanisms of LLLT will help resolve some
may also prove helpful in killing bacteria, fungi, and vir-
of these questions. Some negative results are also attributed
uses.28 LLLT has also been used to achieve attenuation of
to poor design and use of very low doses.33 Unresolved ques-
retinal toxicity in methanol-poisoned rats.27 The role of LLLT
tions regarding the properties of light being used include:
in hair growth was discovered accidentally in 1967.26 In an
wavelength, laser vs noncoherent, dose, pulsed vs continuous
attempt to test if LLLT causes cancer in shaved mice, re-
wave (CW), and polarization status.26 All of these conditions
searchers discovered that these mice did not develop cancer,
and cell culture condition will determine the effect of LLLT.33
but instead grew hair.26
Usually wavelengths in the 600-1000 nm range and powers
Before describing the mechanisms of LLLT, a brief dis-
from 5–500 mW are used.25 Evans and Abrahamse33 studied
course into its terminology will be taken. The term "laser"
the effect of light with wavelengths of 638.2, 830, and 1064
refers to the fact that monochromatic light is used.27 This is
nm at 5, 10, and 16 J/cm2 intensities to compare control vs
in contrast to light emitting diode (LED). The term "low
wounded fibroblasts. They found the most stimulatory effect
level" alludes to the fact there is a specific wavelength of
on wounded fibroblasts using 5 J/cm2 of 632.8 nm light.33
light that has optimal therapeutic effects, and any level higher
They also found the dose of 16 J/cm2 to cause DNA damage
or lower than this may not be proficient.26 This therapeutic
and reversible cell damage (in most instances).33 Similarly, in
window ranges roughly from 600 to less than 1,400 nm, and
assessing free radical formation, Haywood et al34 found no
is close to the absorption spectrum of hemoglobin and water,
detectable free radicals after exposure of human skin biopsy
respectively.26 Furthermore, respiratory chain components
to 694 nm light at 11–14 J/cm2 in 0.9 ms pulses using electron
(mainly cytochrome c) have a similar absorption spec-
spin resonance spectroscopy.
trum.26 This low level results in a negligible change intissue temperature.25
LLLT appears safe and effective for the treatment of hair
The Mechanism of LLLT
loss in theory and through minimal observational studies, but
There are several theories that explain the mechanisms of
more clinical and in vitro studies are needed. Proposed in
LLLT: cytochrome c oxidase-mediated increase in adenosine
vitro studies may include the effect of LLLT on fibroblast
triphosphate (ATP) production, the singlet oxygen hypothe-
function in controlled settings. Factors such as growth rate
sis, the redox properties alteration hypothesis, and nitrous
and apoptotic rate may be assessed. Similar in vitro studies
oxide (NO) hypothesis.26 Cytochrome c oxidase is part of the
may be carried out with intact hair follicles. Finally, random-
respiratory chain that ultimately results in ATP production. It
ized double blind multicenter trials are needed to truly assess
is hypothesized that the light absorbed by this moiety may
safety and efficacy; one such trial has found promising results
ultimately result in increased ATP production, which may
thus far.35 Another study of seven patients did not reveal
alter cell metabolism.26 This is a concept similar to photo-
statistical significance, and proposed that some individuals
synthesis in plants. Singlet oxygen hypothesis stems from the
may be more responsive to this treatment.36
fact that radiation used in high doses to kill cancer cellscauses a paradoxical cell proliferation in low doses.26 Theredox properties alteration hypothesis proposes that enzymes
other than cytochrome c are induced to produce superoxide
1. Bienova´ M, Kucerova´ R, Fiura´skova´ M, et al. Androgenetic alopecia and
anion.26 The NO hypothesis proposes that LLLT may unin-
current methods of treatment. Acta Dermatovenerol Alp Panonica Adriat2005;14:5– 8.
hibit the effect of NO on cytochrome c.26
2. Otberg N, Finner AM, Shapiro J. Androgenetic alopecia. Endocrinol
There have been several studies to evaluate the effects of
Metab Clin North Am 2007;36:379 –398.
LLLT. Increase in ATP synthesis, proton electrochemical po-
3. Poulos GA, Mirmirani P. Investigational medications in the treatment of
tential, and oxygen uptake have all been shown in rat liver
alopecia. Expert Opin Investig Drugs 2005;14:177–184.
mitochondria.26,29,30 LLLT has been shown to increase pro-
4. Dinh QQ, Sinclair R. Female pattern hair loss: current treatment con-
collagen synthesis in fibroblasts.25,26 However, numerous hu-
cepts. Clin Interv Aging 2007;2:189 –199.
man and animal studies have shown inconsistent results,
5. Stough D, Stenn K, Haber R, et al. Psychological effect, pathophysiol-
mainly due to lack of coherence in protocols.25 Some also
ogy, and management of androgenetic alopecia in men. Mayo Clin Proc
relate the variability in results across studies to the fact that
the effect of LLLT depends on the physiologic state of cells.31
6. Shin HS, Won CH, Lee SH, et al. Efficacy of 5% minoxidil versus
2010 Southern Medical Association

combined 5% minoxidil and 0.01% tretinoin for male pattern hair loss:
laser/light sources in the treatment of male and female pattern hair loss.
a randomized, double-blind, comparative clinical trial. Am J Clin Der-
J Cosmet Laser Ther 2007;9:27–28.
25. Sobanko JF, Alster TS. Efficacy of low-level laser therapy for chronic
7. Ellis JA, Sinclair RD. Male pattern baldness: current treatments, future
cutaneous ulceration in humans: a review and discussion. Dermatol Surg
prospects. Drug Discov Today 2008;13:791–797.
8. Price VH. Treatment of hair loss. N Engl J Med 1999;341:964 –973.
26. Hamblin MR, Demidova TN. Mechanisms of low level light therapy
9. Venkataram M. Changing trends in hair restoration surgery. Indian J
Proc SPIE 2006;6140:1–12.
Dermatol Venereol Leprol 2006;72:103–111; quiz 112, 125.
27. Desmet KD, Paz DA, Corry JJ, et al. Clinical and experimental appli-
10. Scheinfeld N. A review of hormonal therapy for female pattern (andro-
cations of NIR-LED photobiomodulation. Photomed Laser Surg 2006;
genic) alopecia. Dermatol Online J 2008;14:1.
11. Haber RS. Pharmacologic management of pattern hair loss. Facial Plast
28. Taub AF. Photodynamic therapy: other uses. Dermatol Clin. 2007;25:
Surg Clin North Am 2004;12:181–189.
12. Bedocs LA, Bruckner AL. Adolescent hair loss. Curr Opin Pediatr
29. Pastore D, Greco M, Petragallo VA, et al. Increase in 4H⫹/e- ratio of the
2008;20:431– 435.
cytochrome c oxidase reaction in mitochondria irradiated with helium-neonlaser. Biochem Mol Biol Int 1994;34:817– 826.
13. Burkhart CG, Burkhart CN. 5 alpha-reductase and finasteride in pattern
alopecia and acne. J Drugs Dermatol 2004;3:363–364.
30. Yu W, Naim JO, McGowan M, et al. Photomodulation of oxidative
metabolism and electron chain enzymes in rat liver mitochondria. Pho-
14. Essah PA, Wickham EP III, Nunley JR, et al. Dermatology of androgen-
tochem Photobiol 1997;66:866 – 871.
related disorders. Clin Dermatol 2006;24:289 –298.
31. Hawkins DH, Abrahamse H. The role of laser fluence in cell viability,
15. Rogers GE, Hynd PI. Animal models and culture methods in the study
proliferation, and membrane integrity of wounded human skin fibro-
of hair growth. Clin Dermatol 2001;19:105–119.
blasts following helium-neon laser irradiation. Lasers Surg Med 2006;
16. Wasserman D, Guzman-Sanchez DA, Scott K, et al. Alopecia areata. Int
38:74 – 83.
J Dermatol 2007;46:121–131.
32. Ferna´ndez-Guarino M, Harto A, García-Morales I, et al. Failure to treat
17. Lenane P, Pope E, Krafchik B. Congenital alopecia areata. J Am Acad
alopecia areata with photodynamic therapy. Clin Exp Dermatol 2008;
Dermatol 2005;52(2 suppl 1):8 –11.
18. Dombrowski NC, Bergfeld WF. Alopecia areata: what to expect from
33. Evans DH, Abrahamse H. Efficacy of three different laser wavelengths
current treatments. Cleve Clin J Med 2005;72:758, 760 –751; 765–756
for in vitro wound healing. Photodermatol Photoimmunol Photomed
2008;24:199 –210.
19. Ross EK, Shapiro J. Management of hair loss. Dermatol Clin 2005;23:
34. Haywood RM, Wardman P, Gault DT, et al. Ruby laser irradiation (694
nm) of human skin biopsies: assessment by electron spin resonancespectroscopy of free radical production and oxidative stress during laser
20. Bui K, Polisetty S, Gilchrist H, et al. Successful treatment of alopecia
depilation. Photochem Photobiol 1999;70:348 –352.
universalis with alefacept: a case report and review of the literature.
Cutis 2008;81:431– 434.
35. Leavitt M, Charles G, Heyman E, et al. HairMax LaserComb laser
phototherapy device in the treatment of male androgenetic alopecia: a
21. Buhl AE, Waldon DJ, Kawabe TT, et al. Minoxidil stimulates
randomized, double-blind, sham device-controlled, multicentre trial. Clin
mouse vibrissae follicles in organ culture. J Invest Dermatol 1989;
Drug Investig 2009;29:283–292.
36. Avram MR, Rogers NE. The use of low-level light for hair growth: part
22. Rawnsley JD. Hair restoration. Facial Plast Surg Clin North Am 2008;
I. J Cosmet Laser Ther 2009;11:110 –117.
16:289 –297, v.
37. Hamilton JB. Patterned loss of hair in man; types and incidence. Ann N
23. Avram MR, Rogers NE. Hair transplantation for men. J Cosmet Laser
Y Acad Sci 1951;53:708 –728.
Ther 2008;10:154 –160.
38. Norwood OT. Male pattern baldness: classification and incidence. South
24. Avram MR, Leonard RT Jr, Epstein ES, et al. The current role of
Med J 1975;68:1359 –1365.
Southern Medical Journal • Volume 103, Number 9, September 2010
Source: http://clinicadepele.com.br/Arquivos/artigos/quedadecabelo/lasercapilar04.pdf
geobiologie.biz
Wie Wildtiere Blauer Engel entzweit ein auf Handystrahlen für das Dorf im Allgäu Samuel Hahnemanns Jünger freuten sich über ihren Trumpf: Homöopathie kuriert auch kranke Tiere. Seit Wissenschaftler dies wissen, rauben sie allen Kritikern die Argumente, die hartnäckig die Heilerfolge der sanften Medizin ins Reich der Phantasie abdrängen. Niemand
eee-researchers.gr
the year in science Two of the biggest breakthroughs of this leap year relied on breathtaking amounts of data. The ENCODE project has generated 15 terabytes of data over the past five years to uncover the functions of human DNA sequences; CERN has stored 26 petabytes of data this year alone from its Large Hadron Collider, as physicists worked to prove the existence