Ar ¥ vol 10 ¥ nr 5
AR • Vol 10 • Nr 5 15.01.2001 16:11 Uhr Seite 231 THE ERYTHROCYTE ADHESIVENESS/AGGREGATION TEST (EAAT) IN THEPERIPHERAL BLOOD OF PATIENTS WITH ISCHEMIC HEART AND BRAIN
DISEASE WITH NORMAL FIBRINOGEN CONCENTRATIONS
D. Zeltser1, R. Rotstein1, O. Rogowski1, R. Fusman1, I. Shapira1, V. Prochorov1, N. M.
Bornstein2, A. Roth3, G. Keren3, D. Avitzour4, N. Arber5, A. Eldor6, S. Berliner1* Departments of Internal Medicine "D" 1, Neurology 2, Cardiology 3, Gastroenterology 5 and Hematol- ogy6, Tel Aviv Sourasky Medical Center, Tel Aviv, affiliated to the Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel, and Timorim4 Technologies, Jerusalem, Israel * Department of Internal Medicine "D", Tel-Aviv Sourasky Medical Center, 6 Weizman Street Tel Aviv 64239, Israel Phone: x972.3.6973313 Fax: x972.3.6974961 Received: 8.5.2000, Final version: 20.9.2000 ABSTRACT
Previous studies have documented the presence of increased red blood cell aggregability in patients with
ischemic heart and brain diseases. We adapted a simple slide technique and image analysis to reveal the state
of erythrocyte adhesiveness/aggregation (EAA) in the peripheral blood of 206 such patients and in 174 controls.
A significant (P<0.0001) correlation was noted between the EAA state and both fibrinogen concentrations and
erythrocyte sedimentation rate in the whole cohort. Noteworthy was a highly significant increment in the EAA
state in a subgroup of 49 patients who had normal fibrinogen concentrations when compared to matched
healthy controls. This was also the case in 82 patients who had a normal erythrocyte sedimentation rate. Thus,
the EAA assay appears to have the advantage of revealing the presence of acute phase response sticky proteins
not detected by either the erythrocyte sedimentation rate or clottable fibrinogen in some patients with a doc-
umented ischemic vascular disease.
Zusammenfassung
Vorangegangene Untersuchungen haben ein erhöhtes Aggregationsvermögen roter Blutkörperchen bei Patien-
ten mit kardialen und cerebralen Ischämien zeigen können. Mit einer einfachen rheologischen Analysetechnik
wurde in dieser Studie die Erythrozytenadhäsion und -aggregation (EAA) im peripheren Blut von 206 solcher
Patienten untersucht und mit 174 Kontrollpersonen verglichen. Es wurde eine signifikante (p<0.0001) Korrela-
tion zwischen der EAA und der Fibrinogenkonzentration sowie der Blutkörperchensenkungsgeschwindigkeit
(BKS) bei den untersuchten Personen gefunden. Erwähnenswert war ein hochsignifikanter Anstieg der EAA in
einer Untergruppe von 49 Patienten, welche im Vergleich zugesunden Kontrollpersonen normale Fibrino-
genkonzentrationen hatten. Das war auch bei 82 Patienten der Fall, die eine normale BKS aufwiesen. Folglich
scheint die Untersuchung der EAA den Vorteil zu bieten, die Präsenz von adhärenten Akute-Phase-Proteinen
anzuzeigen, welche weder mittels BKS noch anhand einer Fibrinogenbestimmung bei einigen Patienten mit
ischämischen Gefäßerkrankungen festgestellt werden kann.
Résumé
Des études précédentes ont certifié la présence d'une aggrégabilité accrue des cellules sanguines chez des
patients avec un coeur ischémique et des maladies du cerveau. Nous avons adapté une technique simple de
glissement et d'analyse d'image afin de révéler l'état d'aggrégation/non aggrégation de l'érythrocyte (EAA) dans
le sang périphérique de 206 patients et pour 174 tests. Une corrélation significative (P<0.0001) a été remarquée
entre l'état de l'EAA et les concentrations en fibrinogènes et le taux de sédimentation de l'érythrocyte dans tous
les tests effectués. Plus particulièrement, dans un sous groupe de 49 patients, qui possèdent des concentrations
normales en fibrinogènes, nous avons remarqué une augmentation très significative de l'état de l'EAA par rap-
port à des contrôles saints équivalents. Ce fut également le cas pour 82 patients présentant un taux normal de
sédimentation de l'érythrocyte. Ainsi, le test de l'EAA semble avoir l'avantage de pouvoir détecter la présence
de protéines collantes, qui ne peuvent être révélées par le taux de sédimentation de l'érythrocyte ou par la
présence de fibrinogène coagulant, chez des patients atteints de maladies vasculaires de nature ischémique.
Key words: Erythrocyte aggregation, ischemic vascular disease
Appl. Rheol. 10, 5, 231-237 (2000) September/October 2000
AR • Vol 10 • Nr 5 15.01.2001 16:11 Uhr Seite 232
Table 1 (left):
The correlation between the
concentration of the hemo-
globin and percent of hema-
tocrit and either the ery-
throcyte sedimentation rate
(ESR) or the variables of the
test (VR, AR, EP) in 380
patients with ischemic vas-
cular diseases and in the
controls (VR = vacuum
radius, AR = aggregation
radius, EP = erythrocyte per-
PATIENTS AND METHODS
Table 2 (right):
A significant correlation is
Previous studies have shown that there is an
present between the three
increased red blood cell aggregability in patients
PATIENTS AND CONTROLS
variables of the erythrocyte
with ischemic heart [1-5] and brain[6-9] disease.
Consent was obtained from all the individuals
test (EAAT) (VR, AR, EP) and
This augmented aggregation might have detri-
who participated in the present study according
either fibrinogen concentra-
mental rheological consequences that lead to
to the approval of the local ethics committee.
tion or the erythrocyte sedi-
the need for therapeutic interventions for reduc-
Included were two groups of patients with ische-
mentation rate (ESR) in 380
ing the degree of these cellular interactions.[10-
mic vascular diseases and one of healthy controls.
patients and controls.
16]. There are various reasons for the appearance
Group assignment was as follows:
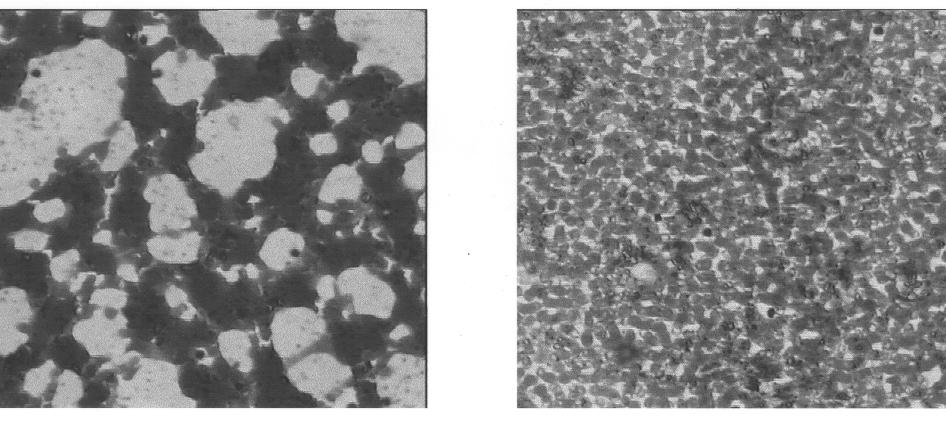
Figure 1 (bottom):
of increased erythrocyte aggregation in patients
A typical picture from a
with ischemic vascular diseases, among which
1. Ischemic heart disease: patients with chest
patient with increased ery-
are the presence of an acute phase response and
pain who were admitted for observation and
throcyte adhesiveness/ag-gregation (left) and a con-
an increased synthesis of adhesive proteins,[17]
in whom acute myocardial infarction was
trol (right).
hyperlipidemia,[18] and changes in the erythro-
ruled out. Documentation of ischemic heart
cyte's membrane.[19] We have recently adapted
disease was by means of a history of myocar-
a simple slide technique and image analysis to
dial infarction (MI), coronary artery bypass
reveal the erythrocyte adhesiveness/aggrega-
graft surgery (CABG), present or past positive
tion state in the peripheral blood.[20-25] The pre-
coronary angiography, or a positive thallium
sent study was conducted in patients with docu-
mented ischemic heart and brain disease. We
2. Ischemic neurological event: patients with an
could note the expected significant correlation
acute transient ischemic attack or ischemic
between the results of this test and either fib-
stroke in whom a hemorrhagic stroke was
rinogen concentration or the erythrocyte sedi-
ruled out by means of computerized tomog-
mentation rate. However, an unexpected and
significant increment in the EAA state was found
3. Healthy controls: members of the medical
in a subgroup of patients who had normal fib-
staff and members of a health club who vol-
rinogen concentrations and a normal rate of ery-
unteered to participate in the study.
throcyte sedimentation, suggesting a potentialadvantage of the erythrocyte adhesive-
Excluded from the present study were individuals
ness/aggregation test (EAAT) in unmasking rhe-
who had any underlying inflammatory or malig-
ological information that is not provided by
nant disease as well as those who were on
either the measurement of clottable fibrinogen
steroidal or non-steroidal anti-inflammatory
or the erythrocyte sedimentation rate.
medications (except for aspirin up to a dose of 325mg per day). In addition, we excluded individualswho had any traumatic or infectious conditionincluding angiography, surgery or MI during thethree months preceding study recruitment.
VARIABLES OF THE ACUTE PHASE RESPONSE
The blood count was performed by means of theCoulter STKS electronic cell analyzer, the erythro-cyte sedimentation rate by the method of West-ergren [26] and the concentration of fibrinogenby the method of Clauss [27] and a Sysmex x6000analyzer.
232 Applied Rheology
September/October 2000
AR • Vol 10 • Nr 5 15.01.2001 16:11 Uhr Seite 233
2.2.2 PREPARATION OF PERIPHERAL BLOOD
to Class 1, which we name Erythrocyte Percent-
age (EP). This is the proportion of image area cov-
The guidelines for the preparation of the periph-
ered by erythrocytes. The two-point statistics are
eral blood slides were reported elsewhere.[28]
described by the probability p1(r) of a pixel
Briefly, blood was drawn into a syringe contain-
belonging to Class 1, given that it is a distance r
ing sodium citrate (one volume of 3.8% sodium
from a pixel Class 1, and similarly the probability
citrate and three volumes of whole blood). Sev-
p2(r) of a pixel belonging to Class 2, given that it
eral large drops of blood were placed on a slide
is a distance r from a pixel of Class 2. These prob-
that was held for 2 to 3 seconds at an angle of 45°
abilities are equal to 1 for r = 0 and decrease as
so that the blood could run down by gravity, leav-
functions of r. As r grows without bound they
ing a fine film. The slides were then dried at room
tend to EP and 1-EP, respectively. The typical size
temperature while in a completely horizontal
of erythrocyte aggregates and of plasma spaces
position. Automatic staining was performed by
may be quantified by the rate of decrease of the
means of the HEMA TEK slide stainer (AMES) and
functions p1(r) and p2(r). In the following discus-
a HEMA TEK bloc colorant stain pack (Bayer Diag-
sion we will deal with p1, where it is understood
that the treatment of p2 is similar. If, for exam-ple, the erythrocyte aggregates are very small,
2.2.3 INFLAMMATION METER (INFLAMET™)
the probability p1(r) will decrease very fast as a
For analysis of the slides, we used an image
function of r because at a quite a short distance
analysis system (INFLAMET™) [20-25] consisting
from a point of Class 1, a pixel has no longer a
of a Pentium Win 95 equipped with a Matrox
marked preference to belong to Class 1. A typical
Meteor colour frame grabber, a colour CCD cam-
distance scale for the size of aggregates may be
era and a microscope which was operated at x
defined by the negative inverse of the derivative
200 magnification, resulting in an image resolu-
of p1 at r = 0. The derivative must be computed
tion of 0.4 micron per pixel. Nine images were
numerically, which we did using the following
taken from each slide. The fields of view were
chosen systematically to sample differentregions on the slide. Each image is processed sep-
• Choose a threshold somewhat smaller than 1
arately and the outputs are then averaged to
• Find r such as p
) = threshold
form the final slide outputs. The nine fields of
• Estimate p1'(0) as:
view cover a total area of 0.6 mm2.
TION TEST (EAAT)
• The desire distance scale is:
The erythrocyte adhesiveness/aggregation statein the peripheral blood was determined by usingthe same image analysis system (INFLAMET™).
We have used color characteristics to classifyimage pixels into two classes:
In practice we chose threshold = 0.7 since downto this value p1 appears to be linear. We define
Class 1: Aggregates of erythrocytes
the aggregation radius (AR) as r0 - differing by a
Class 2: Everything else (plasma, platelets,
constant factor of 0.3 from above. Vacuum
Radius (VR) is the analogous quantity defined forclass 2.
A description of one-point and two-point statis-tics for this classification turns out to require very
2.2.5 STATISTICAL ANALYSIS
few parameters. The main reason for this is that
Means ± SD, Student's t-test and the Pearson
the image statistics are homogenous (position-
coefficient of correlation were carried out by
independent) and isotropic (direction-indepen-
means of the SPSS package. By using the paired
dent). The one point statistics are completely
t-test, we compared a subgroup of patients who
described by the probability of a pixel belonging
had either normal concentrations of fibrinogen
September/October 2000
AR • Vol 10 • Nr 5 15.01.2001 16:11 Uhr Seite 234
or a normal erythrocyte sedimentation rate to
A significant difference in all
healthy controls who presented with exactly the
three variables of the ery-
same values. Thus, a patient with a fibrinogen
ness/aggregation test exists
concentration of 292 mg/dL was compared to a
between patients with
healthy individual with the same value, etc.
ischemic heart and brain
disease and the controls
despite of their being no dif-
ference in the concentration
In the present study, we examined a total of 134
of fibrinogen between the
patients with an ischemic heart disease (age
groups (paired t-test; Hb =
hemoglobin, HCT = hemat-
62±13 years; 89 males and 45 females), 72 with an
ocrit, ESR = erythrocyte sedi-
ischemic neurological event (age 70 ± 12 years; 39
mentation rate, Fg = fib-
males and 33 females) and 174 healthy individu-
rinogen; all values are given
in mean ± SD).
als (age 39 ± 17 years, 92 males and 82 females).
The correlation between the three variables ofthe erythrocyte adhesiveness/aggregation test,i.e., the VR, AR and EP, and the hemoglobin con-centration and the hematocrit values in 380 indi-viduals (patients and controls) are shown in
Table 1. These correlations were also significant
A highly significant differ-
when they were applied to the erythrocyte sedi-
ence in all three variables of
the erythrocyte adhesive-
mentation rate (Table 1).
There was a highly significant correla-
(EAAT) exists between
tion between the three variables of the EAAT and
patients with ischemic heart
the concentration of fibrinogen as well as the ery-
and brain disease and the
controls despite of there
throcyte sedimentation rate (Table 2). However,
being no significant differ-
when the results obtained in a subgroup of
ence in their erythrocyte
patients in whom the concentration of fibrino-
gen was found to be within normal limits (i.e.,200-400 mg/dL) were compared to the normalvalues in the controls, significant differences inthe variables of the erythrocyte adhesive-ness/aggregation were observed, despite com-parable fibrinogen concentrations (paired t-test,Table 3). Similar differences could also be seen ina subgroup of patients who had not only com-parable fibrinogen concentrations but also
exactly the same erythrocyte sedimentation rate
A highly significant differ-
(Table 4). In an analysis of a smaller group, we
ence exists for all three vari-
could reproduce the results and show that this is
ables of the erythrocyte
not an age-related effect (Table 5).
test (EAAT) between
patients with ischemic heart
and brain disease and the
controls despite of there
We adapted a simple slide test coupled with a
being no significant differ-
precise image analysis system to study the ery-
ence in their age, erythro-
throcyte adhesiveness/aggregation state in the
cyte sedimentation rate or
peripheral blood of patients with documented
(n.s. = not significant).
ischemic heart and brain diseases. As expected,a significant correlation was noted between theadhesiveness/aggregation state and the con-centration of fibrinogen in both the patients andcontrols. In effect, fibrinogen has been shown in
234 Applied Rheology
September/October 2000
AR • Vol 10 • Nr 5 15.01.2001 16:11 Uhr Seite 235
the past to be a major determinant in the appear-
correlation between the EAAT and fibrinogen
ance of aggregated erythrocytes in the peripher-
concentrations that was observed when the
al blood [29] although other acute phase
group was evaluated as a whole is suggestive
response proteins could participate as well [17,
that this molecule does have some role in the
18]. However, our main intent in conducting this
induction and on the maintenance of an
study was to determine whether the EAAT is
increased cell aggregability. The fact that we
capable of disclosing information that is not
could increase the aggregability of the cells by
available by looking at the results of either clot-
using an intravenous infusion of gamma globu-
table fibrinogen or the sedimentation rate. To do
lin [22] as well as our yet unpublished observa-
so, we matched patients and controls who had
tions that this aggregability can be attenuated
exactly the same within normal limits (200-400
by reducing cholesterol and triglyceride concen-
mg/dl) fibrinogen concentrations. It turned out
trations in hyperlipidemic individuals, raises the
that a clear and significant increment in the EAAT
possibility that we are facing a kind of a "sum-
values could be seen in the group of patients with
marizing" effect of various aggregatory forces
ischemic vascular diseases as opposed to the con-
that operate on the cells in the peripheral blood
trols (Table 3). In a further sub-analysis, we could
of a given patient.
show the same results for patients and controls
The use of image analysis to detect the
who had an identical erythrocyte sedimentation
aggregability of red blood cells is not new and has
rate: again, a highly significant increment in the
been reported in the past [33]. The novel
EAAT existed in the patients as opposed to the
approach is that we use no dilution or washing
controls. Our conclusion is that the direct obser-
steps and that the slide test is extremely easy to
vation of the aggregated erythrocytes made pos-
perform. At the moment we do not know if the
sible by using the slide test discloses information
aggregation radius and the vacuum radius have
that is not demonstrated by either clottable fib-
any physiological significance except the idea
rinogen concentrations or the erythrocyte sedi-
that they give for the typical size of erythrocyte
mentation rate in some of the patients.
aggregates and plasma spaces, respectively.
There are multiple causes that can
However, we are currently investigating the rela-
increase the adhesiveness and aggregation of
tions between the morphology of the aggrega-
red blood cells in the peripheral blood of patients
tion and the inter erythrocytic adhesion forces. It
with ischemic vascular disorders, including pro-
remains to see whether the most round and cir-
teins of the acute phase response [17, 18] hyper-
cular aggregates represent the most sticky cells.
lipidemia [30] and changes in the composition of
This might have consequences in terms of flow
the erythrocyte membrane [19, 31]. The potential
in the microcirculation.
additional diagnostic value of our test is in that
The present study was performed in
while the above-mentioned factors can acceler-
patients with both ischemic heart and brain dis-
ate the sedimentation rate, our test was clearly
ease. We assume that both have similar etiolo-
positive in a group of patients in whom the ery-
gies in terms of the presence of atherosclerosis
throcyte sedimentation rate was observed as
smoldering inflammation as well as similar risk
being within normal limits. Thus, our slide test
factors. However, we could reproduce the results
might be a sensitive test for detecting the pres-
in a group of patients with ischemic brain disease
ence of a smoldering inflammatory response in
solely (to be published elsewhere). Our present
a group of individuals with relatively normal fib-
study favors, therefore, the notion that the find-
rinogen concentrations or erythrocyte sedimen-
ings are not confined to a single clinical entity
tation rates. Although sensitive CRP assays could
and might be related to the underlying patho-
be used for this purpose, the importance of
directly diagnosing the presence of red blood cell
Finally, one has to be aware that various
hyperaggregability [32] lies in the potential ther-
optical methodologies have been used to quan-
apeutic applications that might result from this
titate the aggregability of red blood cells includ-
information [16].
ing the erythroaggregometer (Regules, France),
Although the mechanisms of increased
Laser-assisted optical rotational (cell analyzer,
erythrocyte adhesiveness/aggregation were not
Mechatronics, Netherlands) and the fully auto-
investigated in the current work, the significant
matic erythrocyte aggregometer (Myrene, Ger-
September/October 2000
AR • Vol 10 • Nr 5 15.01.2001 16:11 Uhr Seite 236
many) [34]. However, we introduced our slide
Tanahashi N, Gotoh F et al.: Enhanced Erythro-cyte Aggregability in Occlusive Cerebrovascular
test due to its simplicity, low cost and a potential
Disease, Stroke 20 (1989) 1202-1207.
of becoming a real time (almost bed-side)
Kee DBJr, Wood JH: Rheology of the Cerebral Cir-
methodology. The question was therefore, is it
culation, Neurosurgery 15 (1984) 125-131.
superior to the indirect determination that one
[10] Atkinson RP: Ancrod in the Treatment of Acute
can obtain by using the westergen sedimenta-
Ischemic Stroke. A Review of Clinical Data, Cere-
tion rate [35].
brovasc. Dis 8 Suppl 1 (1998) 23-28.
In conclusion, we have demonstrated
Ehrly AM: Improvement of the Flow Properties
that a simple slide test and image analysis
of Blood: a New Therapeutical Approach in
enables the detection of the presence of aggre-
Occlusive Arterial Disease, Angiology 27 (1976)
gated red blood cells in the peripheral blood of
Walzl M, Lechner H et al.: Improved Neurologi-
patients with ischemic heart and brain diseases.
cal Recovery of Cerebral Infarctions After
Of interest was the discovery that the test
Plasmapheretic Reduction of Lipids and Fibrino-
remained positive even when fibrinogen con-
gen, Stroke 24 (1993) 1447-1451.
centrations or the erythrocyte sedimentation
Tanahashi N, Fukuuchi Y et al.: Ticlopidine
rate were comparable to those obtained in a con-
Improves the Enhanced Erythrocyte Aggregabil-
trol group of healthy volunteers. Thus, the EAAT
ity in Patients With Cerebral Infarction, Stroke 24
might be useful for unmasking relevant infor-
(1993) 1083-1086.
mation that relates to the acute phase response
Beigel Y, Fuchs J et al.: Lovastatin Therapy in
that is not always given by either determining
Hypercholesterolemia: Effect on Fibrinogen,Hemorrheologic Parameters, Platelet Activity,
the concentration of clottable fibrinogen or the
and Red Blood Cell Morphology, J Clin. Pharma-
erythrocyte sedimentation rate.
col. 31 (1991) 512-517.
Branchi A, Rovellini A et al.: Effect of Three
Fibrate Derivatives and of Two HMG-CoA Reduc-
We are indebted to Ms. Esther Eshkol for editor-
tase Inhibitors on Plasma Fibrinogen Level in
ial assistance.
Patients With Primary Hypercholesterolemia,Thromb. Haemost. 70 (1993) 241-243.
[16] Dujovne CA, Harris WS et al.: Effect of Atorvas-
tatin on Hemorheologic-Hemostatic Parame-
Chien S: Blood Rheology in Myocardial Infarction
ters and Serum Fibrinogen Levels in Hyperlipi-
and Hypertension, Biorheology 23 (1986) 633-
demic Patients, Am. J. Cardiol. 85 (2000) 350-353.
Weng X, Cloutier G et al.: Influence of Acute-
Boss N, Wietelmann H et al.: Red Blood Cell
Phase Proteins on Erythrocyte Aggregation, Am
Aggregation in Men With Coronary Artery Dis-
J Physiol. 271 (1996) H2346-H2352.
ease, Eur. J Cardiol. 12 (1980) 47-54.
Weng X, Roederer GO et al.: Contribution of
Rainer C, Kawanishi DT et al.: Changes in Blood
Acute-Phase Proteins and Cardiovascular Risk
Rheology in Patients With Stable Angina Pectoris
Factors to Erythrocyte Aggregation in Nor-
As a Result of Coronary Artery Disease, Circula-
molipidemic and Hyperlipidemic Individuals,
tion 76 (1987) 15-20.
Thromb. Haemost. 80 (1998) 903-908.
Arntz HR, Perchalla G et al.: Blood Rheology in
[19] Martinez M, Vaya A et al.: Alterations in Ery-
Acute Myocardial Infarction: Effects of High-
throcyte Aggregability in Diabetics: the Influ-
Dose I.V. Streptokinase Compared to Placebo,
ence of Plasmatic Fibrinogen and Phospholipids
Eur. Heart J. 13 (1992) 275-280.
of the Red Blood Cell Membrane, Clin. Hemorhe-
Dintenfass L, Forbes CD: Effect of Fibrinogen on
ol. Microcirc. 18 (1998) 253-258.
Aggregation of Red Cells and on Apparent Vis-
[20] Berliner S, Shapira I et al.: Combined Leukocyte
cosity of Artificial Thrombi in Haemophilia,
and Erythrocyte Aggregation in the Peripheral
Myocardial Infarction, Thyroid Disease, Cancer
Venous Blood During Sepsis. A Clue to the Pres-
and Control Systems: Effect of ABO Blood
ence of a Commonly Shared Adhesive Protein(s),
Groups, Microvasc. Res. 9 (1975) 107-118.
Int. J. Clin. Lab. Res. 30 (2000) 27-31.
Grotemeyer KH: Abnormal Hemorheological
Rotstein R, Zeltser D et al.: The Inflammation
Parameters in Vertebrobasilar-Insufficiency,
Meter (INFLAMET). A New Diagnostic Approach
Acta Neurol. Scand. 81 (1990) 529-532.
to Reveal the Presence of an Inflammatory
Fisher M, Meiselman HJ: Hemorheological Fac-
Response and for the Assessment of Its Intensi-
tors in Cerebral Ischemia, Stroke 22 (1991) 1164-
ty, Isr. Med. Assoc. J. 2 (2000) 476-477.
[22] Fusman R, Zeltser D et al.: INFLAMET: an Image
236 Applied Rheology
September/October 2000
AR • Vol 10 • Nr 5 15.01.2001 16:11 Uhr Seite 237
Analyzer to Display Erythrocyte Adhesive-
[29] Fabry TL: Mechanism of Erythrocyte Aggrega-
ness/Aggregation, Eur. J. Int. Med. (in press
tion and Sedimentation, Blood 70 (1987) 1572-
[23] Maharshak N, Kassirer M et al.: The Inflamma-
[30] Vaya A, Martinez M et al.: Red Blood Cell Aggre-
tion Meter: Novel Technique to Detect the Pres-
gation and Primary Hyperlipoproteinemia,
ence of Infection/Inflammation in Patients
Thromb. Res. 72 (1993) 119-126.
Without Leukocytosis but With an Increased
Hadengue A, Razavian SM et al.: Influence of Sial-
Leukocyte Adhesiveness/Aggregation, Acta
ic Acid on Erythrocyte Aggregation in Hypercho-
Haematol. (in press).
lesterolemia, Thromb. Haemost. 76 (1996) 944-
[24] Rotstein R, Zeltser D et al.: An Inflammation
Meter to Reveal the Presence and Extent of
[32] Weng X, Cloutier G et al.: Contribution of the -
Inflammation in Elderly Patients, J. Am. Ger. Soc.
455G/A Polymorphism at the Beta-Fibrinogen
(letter to editor, in press).
Gene to Erythrocyte Aggregation in Patients
[25] Rogowski O, Zeltser D et al.: Correlated Expres-
with Coronary Artery Disease, Throm. Haemost.
sion of Adhesive Properties for Both White and
82 (1999) 1406-1411.
Red Blood Cells During Inflammation. A Clue to
[33] Chen S, Eldor A et al.: Enhanced Aggregability of
the Presence of Denominating Proteins, Biorhe-
Red Blood Cells of Beta-Thalassemia Major
ology (in press).
Patients, Am. J. Physiol. 270 (1996) H1951-H1956.
[26] International Committee for Standardization in
[34] Zhao H, Wang X et al.: Comparison of Three Opti-
Hematology. Recommendation of Measure-
cal Methods to Study Erythrocyte Aggregation,
ment of Erythrocyte Sedimentation Rate of
Clin. Hemorheol. Microcirc. 21 (1999) 297-302.
Human Blood., Immunochemistry 2 (1965) 235-
[35] Danesh J, Collins R et al.: Haematocrit, Viscosity,
Erythrocyte Sedimentation Rate: Meta-Analyses
[27] Clauss A: Gerinnungsphysiologische Schnell-
of Prospective Studies of Coronary Heart Dis-
methode zur Bestimmung des Fibrinogens, Acta
ease., Eur. Heart. J. 21 (2000) 515-520.
Haematol. Basel 17 (1957) 237-246.
[28] Berliner S, Fishelson Z et al.: The Phenomenon of
Leukergy: Induction and Detection of LeukocyteAggregation in Whole Human Blood., J. Lab. Clin.
Med. 109 (1987) 575-582.
September/October 2000
Source: http://vg09.met.vgwort.de/na/68378abb7e42141a27e1d2598860ba?l=http://www.ar.ethz.ch/ARONLINE_FREE/10_231.pdf
The brazing guide
The Brazing Guide GH Induction Atmospheres Turnkey Heating Solutions GH Induction Atmospheres • 35 Industrial Park Circle, Rochester New York 14624 USA • Tel: 585.368.2120 • Fax: 585.368.2123 • [email protected] • www.inductionatmospheres.com The Brazing Guide Brazing is a method of joining two pieces of metal together with a third, molten fil er
Microsoft powerpoint - hiv npep for iafn final 12-5-13 [compatibility mode]
Welcome to the IAFN, SAFE-TA, and MATEC Webinar: PEP for Prevention of HIV: When, Why & How IAFN requests that you e-mail the names of any non-registered attendees who may be sharing this webinar experience with you so we can track attendance. Please send additional attendee names to [email protected] today.