Oxy-powder® complete clinical studies

MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
REPORT FOR HUMAN CLINICAL TRIAL PHASE III
TO STUDY THE SAFETY AND EFFECTIVENESS
OF OXY-POWDER®
DOCUMENT NO.: MCERC/REPT-CLTR/OXY/1205/001
May 30th 2007
TRIAL TO STUDY THE SAFETY AND EFFECTIVENESS
OF OXY-POWDER® IN TREATING CONSTIPATION AND IBS.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE, (A KALTHIA GROUP ORGANIZATION)
Mohan Mill Compound, Ghodbunder Road, Thane-400 607 Ph: No. 91-022-2589 5856 Fax: 91-022-2589 5854 Email: [email protected] / [email protected]
Contacts:
Studies on Safety and Effectiveness of Oxy-Powder® in Treating Constipation
GLOBAL HEALING CENTER, INC.
Sponsored By:
2040 North Loop West, Suite 108 Houston, Texas 77018 Ph: (713) 476-0016, Fax: (713) 476-0017 www.ghchealth.com
Study Centre:
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE, (A KALTHIA GROUP ORGANIZATION), Mohan Mill Compound, Ghodbunder Road, Thane-400 607 Ph: No. 91-022-2589 5856,
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Email: [email protected] / [email protected]
Division:
Clinical Research
Document
Number:
Document Type:
Clinical Trial Report
Study Identifier:
Mfair/oxy/2005-06
Site of Issue:
Thane, Maharashtra
Document Date:
Abstract
"The clinical trial has been conducted following Globally accepted Regulatory Guidelines and
practices as follows":
¾ Human clinical trial was conducted following "Good Clinical Practices (GCP)" under
supervision of an expert team following Helsinki's Declaration for protection of rights of the
patients.The entire study was conducted based on globally accepted ICH 6E guidelines for
determining Safety, Efficacy and Tolerability of Oxy-Powder® in Human subjects.
¾ The Animal toxicity studies were conducted in an ISO certified laboratory following WHO
GCP guidelines and as per OECD tests. The tests were performed as per OECD guidelines
enumerated below:
(a) 5 DAYS ACUTE ORAL TOXICITY TEST-OECD Guidelines Section 4,
Test 420, 17-12 2001
(b) Repeated Dose 28 days Oral Toxicity Study in Rodents-Guidelines Section 4,
Test 408, 21-09-1998
¾ In vitro antimicrobial tests indicated that Probiotic Lactobacillus bulgaricus was not affected
in presence of Oxy-Powder® indicating thereby that Production of B Complex factors
produced by this organism in gastrointestinal tract of patients suffering from constipation and
IBS with related constipation shall continue to be produced in the normal course. The patient
on the Oxy-Powder® treatment shall not suffer from B Complex Deficiency attributed to
lethal effect of Oxy-Powder®.
¾ The capsules can be safely consumed by all vegetarians and non-vegetarians alike. The
ingredients, including the outer inactive cover (Kosher Shell) are Vegetarian. None of the
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
non-vegetarian materials such as gelatin, egg product, meat or chicken products, sea food
products, non-vegetarian oils and fats have been employed in the formulation or during
Constipation is the slow movement of feces (stool or body wastes) through the large intestine
resulting in infrequent bowel movements and the passage of dry, hard stools. The longer it takes for
the stool to move through the large intestine, the more fluid is absorbed and the drier and harder the
stool becomes. Constipation is annoying and uncomfortable, but fecal impaction (a collection of dry,
hard stool in the colon or rectum) can be life threatening. Patients with a fecal impaction may not have
gastrointestinal symptoms. Instead, they may have circulation, heart, or breathing problems. If fecal
impaction is not recognized, the signs and symptoms will get worse and the patient could die. Irritable
bowel syndrome (IBS), a functional gastrointestinal disorder characterized by the interplay of altered
motility, abnormal visceral sensation, and psychosocial factors, is one of the most common reasons
for referral to a gastroenterologist. It is associated with bouts of constipation and diarrhoea.
Multicentric Clinical Trial
‘Oxy-Powder®' used universally as a dietary supplement for relieving constipation was taken
up for the study under Clinical Trials Phase III in 40 constipation and 20 IBS patients in
Open, Randomized, Comparative studies in 2 Centres. The Study protocol included exclusion
and inclusion criteria, mode of administration of test and reference products, evaluation of
effectiveness and safety and data analysis and management. The GCP guidelines were
followed for the conduct of the studies. Reporting of AEs and SAEs has been emphasized.
The duration of the study, post administration was 6 weeks. Primary objective of the clinical
trial was to evaluate effectiveness and safety of Oxy-Powder® in treating constipation and
IBS. The final results indicated that complete cure was obtained in 42.3% patients treated
with Oxy-Powder® (as against 7.7% with Dulcolax), Improvement in 57.7% in patients
treated with Oxy-Powder® (as against 76.9 % with Dulcolax), and 0% failure in patients
treated with Oxy-Powder® (as against 15.4 % with Dulcolax), Thus, efficacy of Oxy-
Powder® in treating constipation was significantly (P<.05) more than Dulcolax. This
indicated that Oxy-Powder® was more efficacious in treating constipation than Dulcolax.
As regards ADR's in the Constipation group of patients, one patient in Oxy-Powder®
administered group of 27 patients had severe diarrhoea on the 2nd day of treatment. He could
not carry out his usual activities and felt dehydrated; hence he was withdrawn from the study
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
on 3rd day. Out of the remaining 26 patients, 2 patients had abdominal fullness after taking
Oxy-Powder® for 2-3 days after which they were symptom- free. Remaining 24 patients had
no ADR's. In the 13 Dulcolax administered group patients, 1 patient had mild abdominal pain
which disappeared without medication. Remaining 12 patients had no ADR's. As regards
ADR's in IBS + Constipation group of patients, none of the patients had any adverse events
during the study period. The patients tolerated Oxy-Powder® quite well.
In Vitro (in a test tube) Microbiological Studies
Before commencing the clinical trials, the in-vitro effect of Oxy-Powder® on the normal
Probiotic strains and colonies of microbes in the digestive tract was evaluated. The results
showed that the Oxy-Powder® capsules with citric acid samples (for acidification required
for liberation of nascent oxygen) were ineffective in killing the tests cultures Escherichia
coli, Staphylococcus aureus, Lactobacillus bifidigus, Enterobacter faecalis and Candida
albicans at the tested concentration indicating thereby that the normal healthy flora of GI
tract is not expected to be disturbed with the administration of Oxy-Powder®.
Animal Toxicity Studies
Non-clinical safety studies involving acute and sub-chronic toxicity in rats (including
histopathology) were also conducted. The acute toxicity profile suggested that Oxy-
Powder® was safe at 5000 mg/kg body weight dose level. The Sub–chronic oral toxicity
study was conducted to determine the toxicity profile of Oxy-Powder® when administered
via oral route daily at the dose level of 1000 mg/kg body weight for male and female animals
for 28 days in Sprague-Dawley rats.
Salient results of the study were as follows:
1) All the male and female animals from control and all the treated dose groups up to 1000
mg/kg survived throughout the dosing period of 28 days and the recovery period of 14 days.
2) No signs of intoxication were observed in male and female animals from different dose
groups during the dosing period of 28 days and during the recovery period of 14 days.
3) Male and female animals from all the treated dose groups exhibited comparable body
weight gain with that of controls throughout the dosing period of 28 days and the recovery
period of 14 days.
4) Food consumption of control and treated animals was found to be comparable throughout
the dosing period of 28 days and the recovery period of 14 days.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
5) Ophthalmoscopic examination, conducted prior to and at the end of dosing period on
animals from control and all the treated dose groups did not reveal any abnormality.
6) Haematological analysis conducted at the end of the dosing period on day 29 and at the
end of recovery period on day 43, revealed no abnormalities attributable to the treatment.
7) Biochemical analysis conducted at the end of the dosing period on day 29 and at the end of
recovery period on day 43, revealed no abnormalities attributable to the treatment.
8) Functional battery observation tests conducted at termination revealed no abnormalities.
9) Urine analysis, conducted at the end of the dosing period in week 4 and at the end of
recovery period in week 6, revealed no abnormality attributable to the treatment.
10) Organ weight data of male and female sacrificed at the end of the dosing period and at the
end of the recovery period was found to be comparable with that of respective controls.
11) Gross pathological examination did not reveal any abnormality.
12) Histopathological examination did not reveal any abnormality.
Based on these findings, the "No Observed Effect Level (NOEL)" of Oxy-Powder® in
Sprague Dawley rats via oral route, over a period of 28 days was found to be 1000 mg/kg
body weight for male and female animals.
Table of Contents
Sr. No. Content
Table of Contents
Synopsis
Acute Oral Toxicity of Oxy-Powder®
Sub Chronic Oral Toxicity of Oxy-Powder®
Antimicrobial Activity Testing of Oxy-Powder® Against 5 Cultures
Clinical Trial Phase III- Part A - Constipation
Clinical Trial Phase III- Part A – IBS + Constipation
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Synopsis
Individual Study Table Referring to Part of the Dossier
Dr. Edward Group's
Sponsor Company
Global Healing Center, Inc.
Finished Product
1. Ozonated Magnesium Oxides with Germanium-132 in
Active Ingredient
Oxy-Powder®
2. Bisacodyl in Dulcolax
(For National Authority Use only)
TITLE OF THE STUDY:
Studies on Efficacy & Safety of Oxy-Powder®
INVESTIGATORS:
CLINICAL:
1. Dr. Sharad Shah
2. Dr.Chetan Bhatt assisted By Dr. Aditi
3. Dr. Meena U. Shah
4. Dr. Deven Parmar
TOXICOLOGY:
1. Dr. Ranjit Bhide
1. Dr. Deepa Bhajekar
PUBLICATION (Reference): Proposed in Journal of Alternative Medicine
STUDIED PERIOD (Years)
Clinical (date of first enrollment) 21-6-2006
Clinical (date of last completed)
Completion
Report Date
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
STUDY OBJECTIVES:
Primary: The effectiveness and safety of Oxy-Powder® in treating constipation and IBS
Secondary: The in-vitro effect of Oxy-Powder® on the normal Probiotic strain and colonies in
the digestive tract. Safety studies involving acute and sub-chronic toxicity in rats/ mice
(including histopathology)
Study Center(s):
OVERALL: MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE, THANE.
Mayfair Clinical Education & Research Centre,
Mohan Mill Compound, opp. Lawkim, Ghodbunder Road, Thane-400 607, India.
Ph. No.: 91-22-2589 5856, Fax.: 91-22-2589 5854
1) NON-CLINICAL DATA
(a) Indian Institute of Toxicology, (FOR TOXICITY STUDIES)
‘KIM' 2057, Sadashiv Peth, Vijaynagar Colony, PUNE-411 030
Tel: 91-020-24333185/ 26819961-62.Telefax: 91-020-26871429
Contact: Prof. J. K. Lalla, PhD.
Contact: Dr. Ranjit Bhide
(b) MicroChem Laboratory, (FOR ANTI-MICROBIAL TESTING)
125, Vardhman Ind. Estate, Gokul Nagar, Thane (W) – 400 601.
Tel: 91-22-55772657. Telefax: 91-22-25304376/25390631.
Contact: Dr. Deepa Bhajekar
2) CLINICAL DATA
(c) Dr. Sharad C. Shah's Clinic,
49, Hughes Road, Mumbai – 400 007.
Tel: 91-22-23632809.
Contact: Dr. Sharad C. Shah
(d) Bhatia General Hospital
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
J. Dadaji Road, Grant Road, Tardeo, Mumbai – 400 007.
Tel : 91-22-23071291-92
Contact: Dr. Chetan B. Bhatt. : 3071291, 3071292
Diagnosis and main criteria for inclusion
Diagnosis :
Patients suffering from constipation alone or constipation with IBS
Main Criteria for inclusion :
1. 18 to 60 years of both sexes (60% females + 40% males)
2. Height & Weight conforming to Height/Weight chart of Life Insurance
Corporation of India
3. Food habits: Vegetarians are eligible but Non–vegetarians preferred
4. Satisfying the Rome II Criteria for Constipation and IBS
Test product, dose and mode of administration
(A)Test product :Oxy-Powder® capsules, each containing 715.5 mg active ingredients
Dose and mode of administration :
For Cleansing: 4 capsules in the evening on an empty stomach with 240 mL water. If 3-5 bowel
movements were not achieved the following day, the dosage was increased by adding two (2)
capsules every night until 3-5 bowel movements were achieved the following day. Finalization of the
dosage was considered as" day one (1)" of the seven (7) day cleanses. This dosage was continued for
seven (7) consecutive days. After the seven (7) day cleanse, the maintenance dose was started.
Maintenance Dose: 4 capsules on alternate days for the next 5 weeks.
Batch number: 112809 Mfr. Date: Not Available Expiry date: Not Available
Duration of treatment: 6 weeks
(B) Reference therapy, dose and mode of administration
Reference therapy, Bisacodyl tablets (Dulcolax tablets of Cadila Health Care Ltd.)
Each tablet containing 5 mg drug was dispensed in a hard gelatin capsule, size ‘0'
Dose and mode of administration: 2 capsules in the evening on an empty stomach with 240 mL
water. Treatment was followed as described for Oxy-Powder® capsules
Batch number G 1136 Mfr. Date: Jan.2006 Expiry date: Dec. 2009
Dose and mode of administration: 2 capsules in the evening on an empty stomach with 240 mL
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
water. Treatment was followed as described for Oxy-Powder® capsules
Criteria for evaluation:
Efficacy in patients :
Findings of i) Stool examination ii) Barium meal and iii) Colonoscopy
Relief of constipation and IBS, improvement of Quality of life
Safety: In-vitro findings of effectiveness of Oxy-Powder® on, normal Probiotic and pathogenic
strains of microbes generally present in digestive tract.Safety studies involving acute and sub-chronic
toxicity in rats (including histopathology)
(a) Recording of ADR's / SAEs, in patients, if any
Statistical methods
Student t test, Chi square or Fisher's exact test
Summary & Conclusions for Constipation Study
EFFICACY RESULTS
Type 1 patients Summary
Efficacy
Oxy-Powder®
Bisacodyl (Dulcolax)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Conclusions
Efficacy of Oxy-Powder® in treating constipation was significantly (P <.05) more than Dulcolax.
This indicated that Oxy-Powder® was more efficacious in treating constipation than Dulcolax.
Summary & Conclusions for IBS + Constipation Study
Type 2 patients Summary
Efficacy
Oxy-Powder®
Bisacodyl (Dulcolax)
Conclusions
Efficacy of Oxy-Powder® in treating IBS with constipation was significantly (P<.05) more than
Dulcolax. This indicated that Oxy-Powder® was more efficacious in treating IBS with constipation
Safety Results - Adverse events
Type 1 patients
One patient in Oxy-Powder® administered group of 27 patients had severe diarrhoea on the 2nd day of
treatment. He could not carry out his usual activities and felt dehydrated; hence he was withdrawn
from the study on 3rd day. Out of the remaining 26 patients, 2 patients had abdominal fullness after
taking Oxy-Powder® for 2-3 days after which they were symptom- free. Remaining 24 patients had
In 13 Dulcolax administered group patients, 1 patient had mild abdominal pain which disappeared
without medication. Remaining 12 patients had no ADR's.
Type 2 patients (IBS+Constipation)
None of the patients had any adverse events during the study period.
Date of report: 30th May 2007
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
SUMMARY REPORT ON ANIMAL TOXICITY
(A) Acute Toxicity
PROJECT NO.12203
ACUTE ORAL TOXICITY OF OXY-POWDER®
IN SPRAGUE DAWLEY RATS
Data Requirements
OECD Guidelines, Section 4, Test No.420, 17th December, 2001.
Study Director: Dr. R. M. Bhide, PhD
Testing Facility: Indian Institute of Toxicology
32/A/1, Hadapsar Industrial Estate,
Pune - 411 013.
Sponsor: Mayfair Clinical Education and Research Centre, Mumbai
ACUTE ORAL TOXICITY OF OXY-POWDER®
TABLE OF CONTENTS
CONTENTS
Table of contents
Statement of Compliance
Statement of Quality Assurance Unit
Personnel Involved in the Study
Summary and Conclusion
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Materials and Methods
Preparation of Dose
Rationale for Selection of Sprague Dawley Rat as Test System
Route of Administration and Reasons for Choice
Justification for Selection of Doses
Randomization and Numbering of Animals
Preparation of Animals
Experimental Procedure
Clinical Signs of Intoxication
Clinical Signs of Intoxication and Mortality
Gross Pathology Findings
Summary of Mortality Record: Table No. A
Summary of Clinical Signs of Intoxication: Table No. B
Mean Body Weight and Percent Body Weight Gain: Table No. C
Summary of Gross Pathology Findings: Table No. D
Individual Animal - Mortality Record: Appendix No. I
Individual Animal - Clinical Signs of Intoxication: Appendix No. II
Individual Animal - Body Weight and Percent Body Weight Gain:
Appendix No. III
Individual Animal - Gross Pathology Findings: Appendix No. IV
STATEMENT OF COMPLIANCE
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Project No. : 12203
Test Substance : Oxy-Powder®
Study Title : Acute Oral Toxicity of Oxy-Powder® in Sprague Dawley Rat
We hereby attest to the authenticity of the study and guarantee that the data is correct and
accurate to the best of our knowledge and that the study was performed by the procedure
described in the Indian Institute of Toxicology Standard Operating Procedures for the testing
of chemicals. We hereby attest that this study was conducted in compliance with Protocol
submitted to and approved by the sponsor. This study was performed in full compliance with
the OECD Guideline for the Testing of Chemicals (No. 420, Section 4: Health Effects)
"Acute Oral Toxicity - Fixed Dose Method" Adopted on 17th December 2001, Schedule "Y"
in Drugs and Cosmetics (Eighth Amendment) Rules 1988, Ministry of Health and Family
Welfare, Government of India and regulations of the Committee for the Purpose of Control
and Supervision of Experiments on Animals (CPCSEA, Indian Institute of Toxicology
Registration No.15/1999/CPCSEA).
_ signed /- 12-7-2006
Study Director Signature Date
Dr. P. R. Tikhe, PhD signed /- 12-7-2006 _ –––––––––––––––– Quality Assurance Unit Signature Date
Mr. V. M. Bhide, M.B.A signed /- 12-72006_
------------- _ ------------------ _
Director, Administration Signature Date
STATEMENT OF QUALITY ASSURANCE UNIT
Project No. : 12203
Test Substance: Oxy-Powder®
Study Title: Acute Oral Toxicity of Oxy-Powder® in Sprague Dawley Rats
Quality Assurance Unit of the testing facility inspected the conduct of study on the following
22/04/2006, Test substance preparation
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
27/04/2006, Clinical observations
Raw data audit - 15/05/2006
Final report audit - 12/07/2006
No inspection led to findings which had to be reported to the management or would have
impaired this study in any way.
Dr. P. R. Tikhe, PhD
_ _ Quality Assurance Unit Signature Date
ARCHIVING
Project No. : 12203
Test Substance: Oxy-Powder®
Study Title: Acute Oral Toxicity of Oxy-Powder® in Sprague Dawley Rats
Indian Institute of Toxicology takes the responsibility of archiving Protocol, Raw data and all
the relevant material generated during the study along with a copy of final report for a period
Mr. V. M. Bhide M.B.A signed/- 12-7-2006 _ _
Director, Administration Signature Date
PERSONNEL INVOLVED IN THE STUDY
Study Director: Dr. R. M. Bhide, PhD
Head Administration : Mr. V. M. Bhide M.B.A
Animal Care: Dr. S. D. Bhande T.V.'s
Technician: Mr. D. G. Shirsath B.Sc., Applied Toxicology
Quality Assurance : Dr. P. R. Tikhe, PhD
SUMMARY AND CONCLUSION
The study now reported was designed to determine the acute oral toxicity profile of Oxy-
Powder® in Sprague Dawley rats.
The sighting study did not result in any signs of intoxication at the dose level of 2000 mg/kg
body weight and the animal survived; therefore, one animal was treated with the higher dose
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
of 5000 mg/kg body weight. No signs of intoxication were observed in animals treated at the
dose level of 5000 mg/kg body weight. Therefore the main study was continued at the dose
level of 5000 mg/kg body weight.
The main study did not result in any signs of intoxication at the dose level of 5000 mg/kg
body weight. All animals survived through the study period of 14 days.
Gross pathological examination did not reveal any abnormalities.
It was concluded that the acute toxicity study of Oxy-Powder® supplied by Mayfair
Clinical Education and Research Centre, Mumbai, when administered via oral route in
Sprague Dawley rats falls into the category 5 criteria of Globally Harmonised System (GHS).
DR. R.M.BHIDE
STUDY DIRECTOR
1) The results relate only to the items tested.
2) This report shall not be reproduced except in full, without the written approval of the
Study Title : Acute Oral Toxicity of Oxy-Powder® in Sprague Dawley Rats
Sponsor : Mayfair Clinical Education and Research Centre, Mumbai
Monitoring Scientist: Dr. J. K. Lalla
Testing Facility : Indian Institute of Toxicology,
32/A/1, Hadapsar Industrial Estate,
Pune - 411 013.
Project No.: 12203
Schedule
Sighting study:
Date of treatment : 20/04/2006 and 22/04/2006
Date of termination 04/05/2006 and 06/05/2006
Main study:
Date of treatment : 24/04/2006
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Date of termination 08/05/2006
Date of reporting : 12/07/2006
Guidelines
This study was performed in full compliance with the OECD Guideline for the Testing of
Chemicals (No. 420, Section 4: Health Effects) "Acute Oral Toxicity - Fixed Dose Method"
Adopted on 17th December 2001.
Schedule "Y" in Drugs and Cosmetics (Eighth Amendment) Rules 1988, Ministry of Health
and Family Welfare, Government of India.
OBJECTIVES
The purpose of this study is to assess the Toxicological profile of Oxy-Powder® to a single
administration via oral route to Sprague Dawley rats. The animals were observed for 14 days
or more, depending on the occurrence of toxic symptoms. The results of acute toxicity study
were useful for selection of doses for repeated dose toxicity study and may also provide
preliminary information on the target organ of toxicity.
MATERIALS AND METHODS
TEST SUBSTANCE
Sponsor : Mayfair Clinical Education and Research Centre, Mumbai
Label on Sample : Oxy-Powder®
Characteristics of Sample :
Consistency - Solid (Capsule)
Disclaimer: The above physicochemical data of test substance is supplied by the Sponsor. All
responsibility with regards to the accuracy and authenticity of this information remains with the
Sponsor. The test lab is not responsible for any variations with the batch number supplied.
Preparation of Dose
Sighting study:
Dose : Treatment – Female: 2000 mg/kg body weight
: 5000 mg/kg body weight
Main study:
Dose : Treatment - Female - 5000 mg/kg body weight
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Dose volume : 10 mL/kg.
Vehicle: Distilled water
Procedure: The test substance was suspended in distilled water to obtain 200.0 mg/mL and 500.0
mg/mL strength of suspensions. The test substance was administered in the dose volume of 10
mL/kg body weight. The formulation was prepared fresh on the day of dosing.
TEST SYSTEM
Strain Sprague Dawley
Source : I.I.T. Animal house
No. of animals per dose : Sighting study: One and Main study: Four
Acclimation: Five days prior to dosing.
Veterinary examination: Before allocation of animals to different doses after the completion of
acclimation period.
Identification of animals: By cage number and individual marking on fur.
Diet: Pelleted feed ad libitum supplied by Nav Maharashtra ,Chakan Oil Mills Ltd., Pune.
Water: Aqua guard potable water in glass bottles ad libitum
Housing & Environment :
Sighting study: One animal per polypropylene cages provided with Bedding of husk.
Main study: Maximum 5 animals per polypropylene cages provided with bedding of husk. The
temperature was maintained between 20 & 24 °C and relative humidity between 30 and 70%; 10-15
air changes per hour and 12 hours each of dark and light cycle was maintained.
Rationale for Selection of Sprague Dawley Rat as Test System
One of the recommended rodent species by the regulatory authorities for conducting preclinical
toxicity studies among rodents, as it is a sensitive species for expression of toxic responses.
1) Rat is recommended rodent species for conducting acute toxicity studies as per OECD
2) Availability of the historical control data at the facility.
Route of Administration and Reason for Choice
Oral route of administration is the proposed therapeutic route of administration in human being
Justification for Selection of Doses
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Sighting study:
Results based on the sighting study, following dose was selected for the main study.
Main study:
(mg/kg body weight)
Randomization and Numbering of Animals
Eleven healthy female rats, acclimatized to laboratory conditions for 5 days prior to dosing, were used
in this study. Animals were randomly assigned to the cages and the individual animal was fur marked
with picric acid. The females were nulliparous and non-pregnant.
Preparation of Animals
The rats were deprived of feed for 16 hours before and 3 hours after the administration of the test
substance. Water was not withheld during this period.
EXPERIMENTAL PROCEDURE
The test substance, suspended in distilled water was administered by gavage to rats using a ball-tipped
intubations needle (18 G) fitted on to a syringe as per SOP on Test Article/Substance (TA/S)
administration – Gavage / Intubations, (SOP No.IIT/S-PSC/16.2).
Allocation of animals:
Sighting study:
Main study:
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Clinical Signs of Intoxication
Observations of clinical signs were made at 10 minutes, 30 minutes, 60 minutes, 2 hours, 4 hours and
6 hours after dosing on day 1 and once daily thereafter for 14 days at approximately the same time.
Cage side observations included changes in the skin, fur, eyes and mucous membrane. It also included
respiratory, circulatory, autonomic and central nervous system and somatomotor activity and
behavioural pattern. Particular attention was directed to the observation of tremors, convulsion,
salivation, diarrhoea, lethargy, sleep and coma.
Mortality
Animals were observed twice daily for mortality
Body Weight
Individual animal body weight were recorded following the period of fasting on day 0, weekly
thereafter and at termination on day 15. Changes in body weights were calculated and recorded.
Gross Pathology
Macroscopic examination was performed on animals found dead and animals sacrificed at the end of
the observation period of 14 days.
Necropsy examination did not reveal any gross abnormality hence histopathological examination was
not carried out.
Clinical Signs of Intoxication and Mortality (Table No. A, B & App. No. I, II)
Sighting study:
Group I - Animal treated at the dose level of 2000 mg/kg body weight did not result in any signs of
intoxication during the study period of 14 days. Animal survived through the study period of 14 days.
Group II - Animal treated at the dose level of 5000 mg/kg body weight did not result in any signs of
intoxication during the study period of 14 days. Animal survived through the study period of 14 days.
Main study:
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Group I - Animals treated at the dose level of 5000 mg/kg body weight did not result in any signs of
intoxication during the study period of 14 days. All animals survived through the study period of 14
Body Weight (Table No. C & App. No. III)
Sighting study:
Group I (2000 mg/kg) - Percent body weight gain after 7 days and 14 days was found to be 14.46%
and 32.93% respectively.
Group II (5000 mg/kg) – Percent body weight gain after 7 days and 14 days was found to be 18.77%
and 36.19% respectively.
Main study: Group I (5000 mg/kg) - Percent body weight gain after 7 days and 14 days was found to
be 15.41% and 30.88% respectively.
Gross Pathology Findings (Table No. D & App. IV)
Macroscopic examination of animals sacrificed at termination revealed no abnormalities.
Table No. A
Summary of Mortality Record
Under the conditions of the present study, the following mortality rates were recorded:
Sighting study:
(mg/kg body weight)
Absolute Relative
Main study
(mg/kg body weight)
Absolute Relative
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table No. B
Summary of Clinical Signs of Intoxication
Sighting study:
Period of signs in
Main study:
Table No. C
Mean Body Weight and Percent Body Weight Gain
Sighting study:
I 2000 124.50 142.50 14.46 165.50 16.14 32.93
II 5000 133.20 158.20 18.77 181.40 14.66 36.19
Main study:
I 5000 130.08 150.00 15.41 170.05 13.39 30.88
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table No. D
Summary of Gross Pathology Findings
Sighting study:
SITE AND LESION OBSERVED
Main study:
SITE AND LESION OBSERVED
(NAD = No Abnormality Detected)
Appendix No. I
Individual Animal - Mortality Record
Sighting study:
Absolute Relative
Main study:
Absolute Relative
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Appendix No. II
Individual Animal - Clinical Signs of Intoxication
Sighting study:
Period of signs in
Main study:
Period of signs in
Appendix No. III
Individual Animal - Body Weight and Percent Body Weight Gain
Sighting study:
Group: I Dose: 2000 mg/kg body weight
1 124.5 142.5 14.46 165.5 16.14 32.93
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Sighting study:
Group: II Dose: 5000 mg/kg body weight
1 133.2 158.2 18.77 181.4 14.66 36.19
Appendix No. III (Contd.)
Individual Animal - Body Weight and Percent Body Weight Gain
Main study:
Group l: Dose: 5000 mg/kg body weight
2 137.8 155.3 12.70 174.8 12.56 26.85
3 125.4 146.9 17.15 168.0 14.36 33.97
4 133.0 151.2 13.68 170.0 12.43 27.82
5 124.1 146.6 18.13 167.4 14.19 34.89
Appendix No. IV
Individual Animal - Gross Pathology Findings
Sighting study:
Dose: 2000 mg/kg body weight
Gross Pathology Findings
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Group: II
Dose 5000 mg/kg body weight
Gross Pathology Findings
Main study:
Dose: 5000 mg/kg body weight
Gross Pathology Findings
[TS = Terminal sacrifice]
[NAD = No abnormality detected]
SUMMARY REPORT ON ANIMAL TOXICITY STUDIES
(B) Sub Chronic Toxicity
PROJECT NO.12204
SUBCHRONIC ORAL TOXICITY STUDY (28 DAY)
OF OXY-POWDER®
IN THE SPRAGUE DAWLEY RATS
STUDY DIRECTOR: DR. R.M.BHIDE Ph.D.
TESTING FACILITY:
INDIAN INSTITUTE OF TOXICOLOGY,
32/A/1, HADAPSAR INDUSTRIAL ESTATE,
PUNE - 411 013, INDIA.
DATA REQUIREMENTS:
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
OECD GUIDELINE,
SECTION 4, TEST NO.408,
21 SEPTEMBER, 1998.
SPONSOR: MAYFAIR CLINICAL EDUCATION AND
RESEARCH CENTRE, MUMBAI
SUB CHRONIC ORAL TOXICITY OF OXY-POWDER®
TABLE OF CONTENTS
Table of Contents
Statement of Compliance
Statement of Quality Assurance Unit
Personnel Involved in the Study
Summary and Conclusion
Materials and Methods
Randomization, Numbering and Grouping of Animals
Route of Administration
Justification for Selection of Sprague Dawley rats for the Study
Justification for Selection of Route
Dose Preparation
Justification for Dose Selection
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Food Consumption
Functional Observations
Terminal Studies
Laboratory Investigations
Haematological Investigations
Biochemical Investigations
Urine Analysis (including microscopy)
Statistical Analysis
Food Consumption
Functional Observations
Haematological Investigations
Biochemical Investigations
APPENDICES
Individual Animal - Body Weight (g)
Individual Animal - Functional Observational Battery
Individual Animal – Haematological Investigations
Individual Animal – Biochemical Investigations
Individual Animal - Urine Analysis
Organ Weights Absolute Values (g)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Individual Animal - Necropsy and Histopathology Findings XI
Normal Laboratory Ranges at Indian Institute of Toxicology
Normal Laboratory Ranges– Haematology
Normal Laboratory Ranges– Biochemistry
STATEMENT OF COMPLIANCE
Project No. : 12204
Test Substance : Oxy-Powder®
Title: Sub chronic Oral Toxicity Study (28 day) Of Oxy-Powder® in the Sprague Dawley Rats
We hereby attest to the authenticity of the study and guarantee that the data is correct and
accurate to the best of our knowledge and that the study was performed by the procedure
described in the Indian Institute of Toxicology Standard Operating Procedures. We hereby
attest that this study was conducted in compliance with Protocol submitted to and approved
by the sponsor. The study also complies with the Schedule Y in Drugs and Cosmetic Act
(2nd Amendment) Rules, 2005, Ministry of Health and Family Welfare, Government of
India, OECD Guideline for the testing of Chemicals No.408, "Repeated Dose 28 -day Oral
Toxicity Study in Rodents" adopted on September 21st, 1998 and regulations of the
Committee for the Purpose of Control and Supervision of Experiments on Animals
(CPCSEA, Indian Institute of Toxicology Registration No.15/1999/CPCSEA).
Dr. R. M. Bhide Ph.D. Signed /- 12-7-2006
Study Director Signature Date
Dr. P. R. Tikhe Ph.D. Signed /- 12-7-2006
Quality Assurance Unit Signature Date
Mr. V. M. Bhide M.B.A. Signed /- 12-7-2006
Director, Administration Signature Date
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
STATEMENT OF QUALITY ASSURANCE UNIT
Project No. : 12204
Test Substance : Oxy-Powder®
Study Title: Sub chronic Oral Toxicity Study (28 day) of Oxy-
Powder®
in the Sprague Dawley Rats
Quality Assurance Unit of the testing facility inspected the conduct of study on the following
10-05-2006, Body weight data collection
11-05-2006, Test substance administration
25-05-2006, Food consumption data collection
08-06-2006, Necropsy
22-06-2006, Haematology technique
Raw data audit: 08-07-2006
Final report audit: 12-07-2006
No inspection led to findings which had to be reported to the management or would have
impaired this study in any way.
Dr. P. R. Tikhe Ph.D. Signed /- 12-7-2006
Quality Assurance Unit Signature Date
ARCHIVING
Project No. : 12204
Test Substance Oxy-Powder®
Study Title: Sub chronic Oral Toxicity Study (28 day) Of Oxy-Powder® in the Sprague
Dawley Rats
Indian Institute of Toxicology takes the responsibility of archiving the following items for a
period of two years: Protocol, Raw data and a copy of Final Report, Wet tissue samples,
Histology slides and blocks.
Mr. V. M. Bhide, M.B.A. Signed /- 12-7-2006
Director, Administration Signature Date
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
PERSONNEL INVOLVED IN THE STUDY
Study Director : Dr. R. M. Bhide Ph.D.
Head Administration: Mr. V. M. Bhide M.B.A.
Animal Care : Dr. S. D. Bhande B. V. Sc. & A. H.
Histopathology : Dr. S. K. Bokan M. V. Sc.
Technician : Dr. V. S. Jagadale M. V. Sc.
Biochemistry : Mr. N. G. Bidkar B.Sc.
Histology : Miss S. G. Tikhe B.Sc., D.M.L.T.
: Mr. S. N. Gaikwad B.Sc., D.M.L.T.
: Mrs. S. C. Gaikwad B.Sc., D.M.L.T.
Quality Assurance : Dr. P. R. Tikhe Ph.D.
SUMMARY AND CONCLUSION
The Sub chronic oral toxicity study was designed and conducted to determine the toxicity
profile of Oxy-Powder® when administered daily for 28 days in Sprague Dawley rats. In
acute toxicity test the compound was found to be non toxic at the dose level of 5000 mg/kg
body weight. The dose has been selected on this basis and the justification provided on page
14 of this report.
Oxy-Powder® suspended in distilled water was administered to animals at the dose levels
250 mg/kg, 500 mg/kg and 1000 mg/kg body weight. Two additional dose levels were added
to the study as 0 mg/kg (Rev.) and 1000 mg/kg (Rev.), in order to study the reversibility or
delayed occurrence of symptoms, if any. The control animals were administered with vehicle
Salient features of the study were as follows:
1) All the male and female animals from control and all the treated dose groups up to 1000
mg/kg survived throughout the dosing period of 28 days and the recovery period of 14 days.
2) No signs of intoxication were observed in male and female animals from different dose
groups during the dosing period of 28 days and during the recovery period of 14 days.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
3) Male and female animals from all the treated dose groups exhibited comparable body
weight gain with that of controls throughout the dosing period of 28 days and the recovery
period of 14 days.
4) Food consumption of control and treated animals was found to be comparable throughout
the dosing period of 28 days and the recovery period of 14 days.
5) Ophthalmoscopic examination, conducted prior to and at the end of dosing period on
animals from control and all the treated dose groups did not reveal any abnormality.
6) Haematological analysis conducted at the end of the dosing period on day 29 and at the
end of recovery period on day 43, revealed no abnormalities attributable to the treatment.
7) Biochemical analysis conducted at the end of the dosing period on day 29 and at the end of
recovery period on day 43, revealed no abnormalities attributable to the treatment.
8) Functional battery observation tests conducted at termination revealed no abnormalities.
9) Urine analysis, conducted at the end of the dosing period in week 4 and at the end of
recovery period in week 6, revealed no abnormality attributable to the treatment.
10) Organ weight data of male and female sacrificed at the end of the dosing period and at the
end of the recovery period was found to be comparable with that of respective controls.
11) Gross pathological examination did not reveal any abnormality.
12) Histopathological examination did not reveal any abnormality
Based on these findings the no observed effect level (NOEL) of Oxy-Powder® supplied by
Mayfair Clinical Education and Research Centre, Mumbai, in Sprague Dawley rat via
oral route, over a period of 28 days was found to be 1000 mg/kg body weight for male and
DR. R.M.BHIDE
STUDY DIRECTOR
1) The results relate only to the items tested.
2) This report shall not be reproduced except in full, without the written approval of the
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Title: Sub chronic Oral Toxicity Study (28 day) of Oxy-Powder® in the Sprague Dawley Rats
Sponsor : Mayfair Clinical Education and Research Centre, Mumbai
Monitoring Scientist Dr. J. K. Lalla
Testing Facility Indian Institute of Toxicology,
32/A/1, Hadapsar Industrial Estate,
Project No. 12204
Test Substance Oxy-Powder®
Schedule
Date of receipt of animals for : 10/05/2006
Treatment (day 0)
Date of treatment (day 1) : 11/05/2006
Date of termination of dosing : 07/06/2006
Date of sacrifice (day 29) : 08/06/2006
Date of completion of recovery : 21/06/2006
Date of sacrifice 43 Day : 22/06/2006
Date of reporting : 12/07/2006
Objective
The objective of this study is to assess the toxicological profile of Oxy-Powder® after
administering at three dose levels by oral route for 28 consecutive days to Sprague Dawley
rats to determine the target organ of toxicity and no observed effect level (NOEL). The study
objective also includes the detection of delayed occurrence or reversibility of any signs /
toxicity at the end of recovery period of 14 days
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
MATERIALS AND METHODS
TEST SUBSTANCE
Sponsor: Mayfair Clinical Education and Research Centre, Mumbai
Label on Sample : Oxy-Powder®
Characteristics of Sample :
Consistency – Solid (Capsule)
Colour – White
Disclaimer: The above physiochemical data of test substance is supplied by the Sponsor. All
responsibility with regards to the accuracy and authenticity of this information remains with the
Sponsor. The test lab is not responsible for any variations with the batch number supplied.
TEST SYSTEM
Strain Sprague Dawley
Source : Indian Institute of Toxicology, Pune
Sex : Male and female
No. of animals per dose level : 5 per sex (dose groups sacrificed on day 29)
5 per sex (reversal groups sacrificed on day 43)
Acclimation : Seven days prior to dosing.
Veterinary examination : Prior to and at the end of the acclimation period.
Identification of animals : By cage number, animal number and individual marking on fur.
Diet : Pelleted feed supplied by Nav Maharashtra Chakan Oil Mills Ltd., Pune
Water: Aqua guard pure water in glass bottles ad libitum
Housing & Environment: The animals were housed 5 each, of the same sex in Polypropylene cages
provided with bedding of husk.
The temperature was maintained between 20 & 24 °C and relative humidity between 30 and 70%; 10-
15 air changes per hour and 12 hours each of dark and light cycle was maintained.
Dose: Male 0 mg/kg, 0 mg/kg (Rev.), 250 mg/kg, 500 mg/kg, 1000 mg/kg and 1000 mg/kg
(Rev.) body weight
Female 0 mg/kg, 0 mg/kg (Rev.), 250 mg/kg, 500 mg/kg,1000 mg/kg and 1000 mg/kg (Rev.) body
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Body weight at start of Study
Male Mean 96.66 g (= 100 %)
Minimum: 91.5 g (- 5.34 %)
Maximum: 100.5 g (+ 3.97 %)
Total No. of animals: 30
Female Mean 87.96 g (= 100 %)
Minimum: 81.7 g (- 7.12 %)
Maximum: 97.3 g (+ 10.62 %)
Total No. of animals: 30
Randomization, Numbering and Grouping of Animals
Sixty rats i.e. 30 male and 30 female healthy animals were randomly divided into four groups of 5
animals per sex for dosing up to 28 days and 5 animals per sex as reversal groups for control and high
dose i.e. 0 mg/kg, 0 mg/kg (Rev.) 250 mg/kg, 500 mg/kg, 1000 mg/kg and 1000 mg/kg (Rev.) body
weight. Animals were allowed acclimation period of 7 days to laboratory conditions prior to the
initiation of treatment. Rats were assigned five per sex per cage wise and the individual animal was
fur marked with picric acid. The females were nulliparous and non-pregnant.
Randomization was conducted as per the Indian Institute of Toxicology Standard Operating Procedure
on Randomization of Study Animals (SOP No.IIT/S-PSC/13).
Route of Administration
Oral (gavage), once daily for 28 consecutive days.
Justification for Selection of Sprague Dawley rats for the Study
1) One of the rodent species recommended as test system for the use in toxicity studies,
2) This test system has been demonstrated to be sensitive to toxins,
3) Widely used throughout industry for the evaluation of toxicity of various products,
4) Historical data and evidence at the facility.
Justification for Selection of Route
The oral route was selected for use because,
Oral route is considered to be a proposed therapeutic route.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Dose Preparation
Oxy-Powder® suspended in distilled water was administered to animals at the dose levels of 250
mg/kg, 500 mg/kg and 1000 mg/kg in the dose volume of 10 mL/kg. The test substance suspensions
were freshly prepared every day for 28 days. The control animals were administered vehicle only.
Justification for Dose Selection
In acute toxicity test the compound was found to be non toxic at the dose level of 5000 mg/kg body
weight. The doses selected for the study were 0 mg/kg, 250 mg/kg, 500 mg/kg and 1000 mg/kg body
Clinical Signs
All animals were observed daily for clinical signs. The time of onset, intensity and duration of these
symptoms, if any, were recorded.
Mortality
All animals were observed twice daily for mortality during the period of the study.
Body Weight
The weight of each rat was recorded on day 0 and at weekly intervals throughout the course of the
study and at termination to calculate relative organ weights. The group means body weights and
percent body weight gain were calculated.
Food Consumption
The quantity of food consumed by groups consisting of five animals of each sex (or ten animals, 0
mg/kg, 250 mg/kg, 500 mg/kg and 1000 mg/kg) and five animals of each sex (or ten animals, 0 mg/kg
Rev. and 1000 mg/kg Rev.) was recorded weekly and the food consumption per animal was calculated
for control and all the treated dose groups.
Ophthalmoscopy
The eyes of control and all the treated dose group animals were examined prior to the initiation of the
dosing and in week 4 and in week 6 (for reversal group animals) of the study. Eye examination was
carried out using a hand slit lamp after induction of mydriasis with 0.5% solution of tropicamide.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Functional Observations
Towards the end of the exposure period in week 4, sensory reactivity to stimuli of different types
(auditory, visual and proprioceptive stimuli) and by grading different stimuli according to the
Standard Operating Procedure for ‘Conduct of functional observational battery' No.IIT/S-PSC/36,
assessment of grip strength (Digital Grip Strength Meter, using Columbus Instrument) and motor
activity assessment was conducted.
TERMINAL STUDIES
Laboratory Investigations
Following laboratory investigations were carried out on day 29 and on day 43 in animal's fasted over-
night. Blood samples were collected from orbital sinus following morning using sodium heparin (200
IU/ml) for Blood chemistry and potassium EDTA (1.5 mg/ml) for Haematology as anticoagulant.
Prothrombin time analysis was conducted using citrate bulb (100 µl of 3.8% solution of sodium citrate
for 1 ml of blood). Blood samples were centrifuged at 3000 rpm for 10 minutes.
Haematological Investigations
Following haematological parameters were studied using Beckman Coulter Haematology analyzer.
Hb : Haemoglobin (g %)
RBC: Red Blood Corpuscles (x 106 /c mm)
HCT: Hematocrit (%)
MCV: Mean Corpuscular Volume (μ m3)
MCH: Mean Corpuscular Haemoglobin (pg)
MCHC: Mean Corpuscular Haemoglobin Concentration (%)
Platelets (x103 / μL)
WBC : White Blood Corpuscles (x 103 / μL)
Analysis of following parameters was performed manually:
Rt. : Reticulocyte (%)
N Neutrophils (%)
L : Lymphocytes (%)
E : Eosinophils (%)
M : Monocytes (%)
B : Basophil (%)
Pt. : Prothrombin time (Sec.)
Biochemical Investigations
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Following biochemical parameters were studied using VeTEX (Veterinary Chemistry Expert) Clinical
Chemistry auto-analyzer system.
Total Protein (g %)
BUN: Blood Urea Nitrogen (mg %)
ALT: Alanine Aminotransferase (IU/L)
AST: Aspartate Aminotransferase (IU/L)
AP: Alkaline Phosphatase (IU/L)
Blood Sugar (mg %)
Phosphorous (mg %)
γ GT: Gamma Glutamyl Transferase (U/L)
Bilirubin (mg %)
Creatinine (mg %)
CPK: Creatine Phospho Kinase (IU/L)
Sodium (m mol/L)
Potassium (m mol/L)
Chloride (m mol/L)
Cholesterol (mg %)
Triglycerides (mg %)
LDH: Lactate dehydrogenase (IU/L)
Urine Analysis
Urine samples were collected in week 4 and in week 6
The following parameters were estimated using appropriate methodology as discussed below:
Volume (urine volume was collected from all male and female animals from each dose group using
metabolic cages and collection duration was fixed at 16 hours.)
Appearance
pH = Multistix
Specific Gravity = Multistix
Proteins = Multistix
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Glucose = Multistix
Ketones = Multistix
Bilirubin = Multistix
Urobilinogen = Multistix
Occult Blood = Multistix
Nitrite = Multistix
Results are reported according to the following convention:
Small amount of analyte = ++
Moderate amount of analyte = +++
Large amount of analyte = ++++
Microscopy
Urine samples were centrifuged at 1000 rpm for 10 minutes. Following components were observed
under the microscope:
P: Pus cells
E: Epithelial cells
Cr: Crystals
The presence and approximate frequency of these constituents are reported according to the
following convention:
Grade Description
None found in any field
Few found in some field
Few found in many field
Many found in many field
Necropsy
All the animals were sacrificed on day 29 except for reversal group animals which were sacrificed on
day 43 i.e. post-dosing period of 14 days, using CO2 asphyxiation technique (body weights mentioned
in the table section are fasting body weights, Appendix No. IX and X).
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Necropsy of all animals was carried out and the weights of the following organs were recorded of
Liver, kidneys, adrenals, epididymis, thymus, spleen, brain, heart, uterus and testes/ovaries. The organ
weights were recorded as absolute values and their relative values (i.e. per cent of the body weight)
were calculated.
Following tissue samples of organs from control and animals treated at the highest dose level of 1000
mg/kg, were preserved in 10% formalin and were subjected to Histopathological examination.
Adrenals, Aorta, Brain, Cecum, Colon, Duodenum, Epididymis, Gonads, Heart, Ileum, Jejunum,
Kidneys, Liver, Lungs, Lymph nodes, Oesophagus, Prostate, Rectum, Sciatic nerve, Spleen, Sternum
with bone marrow, Stomach, Seminal Vesicles, Spinal cord, Thymus, Thyroid / parathyroid, Trachea,
Urinary Bladder and Uterus.
Following tissue samples of organs from low and intermediate dose groups' animals were preserved
for histopathology examination.Liver, kidneys, adrenals, epididymis, thymus, spleen, brain, heart,
uterus and testes/ovaries.
Statistical Analysis
All findings such as clinical signs of intoxication, body weight changes, food consumption, and
haematology and blood chemistry were tabulated. Data on all parameters were evaluated by analysis
(co-)variance followed by Student's' test and Cochran T-Test.
Histopathological observations were tabulated; evaluated and individual animal score is calculated
according to degree and area by using software, LABCAT Module for Histopathology, Innovative
Programming Associates, INC., Princeton, New Jersey.
Clinical Signs
Group I (0 mg/kg): Animals were free of intoxicating signs throughout the dosing period of 28 days
(animal nos.1 to 5).
Group II (0 mg/kg, Reversal): Animals were free of intoxicating signs throughout the dosing period
of 28 days and during the recovery period of 14 days (animal nos.11 to 15).
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Group III (250 mg/kg): Animals were free of intoxicating signs throughout the dosing period of 28
days (animal nos.21 to 25).
Group IV (500 mg/kg): Animals were free of intoxicating signs throughout the dosing period of 28
days (animal nos.31 to 35).
Group V (1000 mg/kg): Animals were free of intoxicating signs throughout the dosing period of 28
days (animal nos.41 to 45).
Group VI (1000 mg/kg, Reversal): Animals were free of intoxicating signs throughout the dosing
period of 28 days and during the recovery period of 14 days (animal nos.51 to 55).
Females -
Group I (0 mg/kg) Animals were free of intoxicating signs throughout the dosing period of 28 days
(animal nos.6 to 10).
Group II (0 mg/kg, Reversal): Animals were free of intoxicating signs throughout the dosing period
of 28 days and during the recovery period of 14 days (animal nos.16 to 20).
Group III (250 mg/kg) Animals were free of intoxicating signs throughout the dosing period of 28
days (animal nos.26 to 30).
Group IV (500 mg/kg) Animals were free of intoxicating signs throughout the dosing period of 28
days (animal nos.36 to 40).
Group V (1000 mg/kg) Animals were free of intoxicating signs throughout the dosing period of 28
days (animal nos.46 to 50).
Group VI (1000 mg/kg, Reversal) Animals were free of intoxicating signs throughout the dosing
period of 28 days and during the recovery period of 14 days (animal nos.56 to 60).
Mortality
Male and Female - All animals from control and all the treated dose groups survived throughout the
dosing period of 28 days and the post-dosing recovery period of 14 days
Body Weight (App. I)
Male and Female - Animals from control and different dose groups exhibited comparable body
weight gain throughout the dosing period of 28 days.During the post-dosing recovery period, animals
from 1000 mg/kg reversal group exhibited normal body weight gain when compared with that of
respective controls.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Food Consumption
Male and Female -
During the dosing period and the post-dosing recovery period the quantity of food consumed by
animals from different dose groups was found to be comparable with that by control animals.
The eyes of control and all the treated dose group animals were examined prior to the initiation of the
dosing and in week 4 and in week 6 (for reversal group animals) of the study. Ophthalmoscopic
examination did not reveal any abnormality.
Functional Observations (App. II, III, IV and V)
Functional observation tests conducted at termination revealed no abnormalities.
Haematological Investigations (App. VI)
Males and Females
Haematological investigations conducted on day 29 and on day 43 (for reversal group animals)
revealed following significant changes in the values of different parameters studied when compared
with those of respective controls; However, the increase or decrease in the values obtained was within
normal biological and laboratory limits. In other words, the effect was not dose–dependent.
MCHC: Decreased values were obtained for animals from 500 mg/kg (P<0.05) and 1000 mg/kg
(P<0.01) dose groups, sacrificed on day 29 and
Total WBC: Increased values were obtained for animals from 500 mg/kg dose group, sacrificed on
day 29 (P<0.05).
Females:
MCV: Increased values were obtained for animals from 500 mg/kg dose group, sacrificed on day 29
MCV and MCH: Increased values were obtained for animals from 1000 mg/kg reversal group,
sacrificed on day 43 (P<0.05).
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Parameters Laboratory range
44.5 to 69.0 (μm3)
12.0 to 24.5 (pg)
21.6 to 42.0 (%)
3.00 to 19.00 (x 103 /uL)
Biochemical Investigations (App. VII)
Males and Females -
Biochemical investigation's conducted on day 29 and on day 43 (for reversal group animals), revealed
following significant changes in the values of different parameters studied when compared with that
of respective controls, however, the values obtained were within normal biological and laboratory
limits or the effect was not dose dependent.
Blood Urea Nitrogen: Elevated levels were observed in animals from 500 mg/kg dose group,
sacrificed on day 29 (P<0.05),
LDH: Elevated levels were observed in animals from 1000 mg/kg dose group, sacrificed on day 29
Aspartate Aminotransferase: Decreased levels were observed in animals from 1000 mg/kg
reversal group, sacrificed on day 43 (P<0.01).
Females:
Alkaline Phosphatase: Elevated levels were observed in animals from 1000 mg/kg reversal group,
sacrificed on day 43 (P<0.05).
Parameters Laboratory range
Alkaline Phosphatase
300 to 400 (IU/L)
Urine Analysis (App. VIII)
Male and Female -
Urine analysis of control and treated animals in week 4 and reversal group animals in week 6,
revealed no abnormality.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Organ Weights (App. XI, X)
Males and Females –
In comparison with respective controls on day 29, organ weight data of animals from different dose
groups was found to be comparable.
In comparison with respective controls on day 43, organ weight data of animals from 1000 mg/kg
reversal group was found to be comparable.
Necropsy (App. XI)
Gross pathological examination did not reveal any abnormality.
Histopathology (App. XI)
Histopathological examination revealed focal Lymphocytic infiltration and/or necrosis in liver,
Lymphocytic infiltration in the kidneys, focal Lymphocytic infiltration in the heart, gliosis in the
brain, interstitial Pneumonitis in the lungs, eosinophillic infiltration in uterus were observed in few
male and female animals from control and 1000 mg/kg dose group animals with similar quality and
quantity and are considered incidental, gender and physiology related and are covered in the
background data of the pathology.
Normal Laboratory Ranges at Indian Institute of Toxicology (App. XII)
Haematology
Parameters Laboratory range
Laboratory range
Laboratory range
11.1 to 18.0 (g %)
10.2 to 16.6 (g %)
9.3 to 19.3 (g %)
5.0 to 12.0 (x 106
6.70 to 12.5 (x 106
4.0 to 8.6 (x 106 /cmm)
36.0 to 52.0 (%)
32.0 to 54.0 (%)
30.0 to 53.0 (%)
44.5 to 69.0 (μm3)
31.0 to 62.0 (μm3)
57.0 to 90.0 (μm3)
12.0 to 24.5 (pg)
9.20 to 20.8 (pg)
16.0 to 31.0 (pg)
21.6 to 42.0 (%)
22.0 to 35.5 (%)
22.0 to 38.7 (%)
140 to 600 (x 103 /uL)
150 to 500 (x 103 /uL)
120 to 800 (x 103 /uL)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
3.00 to 19.00 (x 103
5.40 to 16.00 (x 103
2.0 to 15.0 (x 103 /uL)
Activated Partial
Thromboplastin Time
4.0 to 7.0 % (Young)
1.0 to 3.0 % (Adult)
3.0 to 6.0 % (Young)
0.5 to 2.5 % (Adult)
PARAMETERS Laboratory
range Laboratory range
Laboratory range
Alkaline Phosphatase
90 to 120 (mg %)
90 to 120 (mg %)
90 to 120 (mg %)
70 to 110 (mg %)
70 to 110 (mg %)
70 to 110 (mg %)
0.8 to 1.2 (mg %)
0.8 to 1.2 (mg %)
0.8 to 1.2 (mg %)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
130 to 150 (mmol/l)
130 to 150 (mmol/l)
130 to 150 (mmol/l)
6.6 to 8.6 (g %)
6.6 to 8.6 (g %)
6.6 to 8.6 (g %)
95 to 106 (mmol/l)
95 to 106 (mmol/l)
95 to 106 (mmol/l)
300 to 400 (IU/L)
300 to 400 (IU/L)
300 to 400 (IU/L)
80 to 120 (mg %)
80 to 120 (mg %)
80 to 120 (mg %)
THE END
SUMMARY REPORT OF
ANTIMICROBIAL STUDIES ON OXY-POWDER®
PROJECT NO. 9165
ANTIMICROBIAL ACTIVITY TESTING
OF OXY-POWDER®
AGAINST 5 CULTURES
STUDY DIRECTOR
DR. (MRS) DEEPA BHAJEKAR, Ph.D.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
TESTING FACILITY
THE MICRO CHEM LABORATORY
125, VARDHMAN INDUSTRIAL ESTATE,
GOKUL NAGAR, THANE (W) 400 601
(Laboratory Certified by NABL for ISO / 17025)
SPONSOR: MAYFAIR CLINICAL, EDUCATION AND RESEARCH CENTRE,
DATA REQUIREMENTS
AS SPECIFIED BY SPONSOR
ANTIMICROBIAL ACTIVITY TESTING OF OXY-POWDER®
AGAINST 5 CULTURES
SPONSOR: Mayfair Clinical Education and Research Centre, Mumbai
TABLE OF CONTENTS
Table of Contents
Statement of Compliance
Statement of Quality Assurance Unit
Personnel Involved in the Study
Normal Gastrointestinal Tract Flora Probiotics Intestinal Flora / Probiotics Supportive Information References on Probiotics Diseases caused by overgrowth of potential pathogens
Summary and Conclusion
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Materials and Methods
STATEMENT OF COMPLIANCE
Project No. : 9165
Test Substance : Oxy-Powder®
Study Title: ANTIMICROBIAL ACTIVITY TESTING OF OXY-POWDER® AGAINST 5
CULTURES
We hereby attest to the authenticity of the study and guarantee that the data is correct and accurate to
the best of our knowledge and that the study was performed by the procedure described in The Micro
Chem. Laboratory Standard Operating Procedures. We hereby attest that this study was conducted in
compliance with Protocol submitted to and approved by the sponsor.
The study also complies with the Schedule Y in Drugs and Cosmetic Act (2nd Amendment) Rules,
2005, Ministry of Health and Family Welfare, Government of India,
DR (MRS.) DEEPA BHAJEKAR, Ph.D. Signed /- 03-06-2006
Study Director Signature Date
Miss Nameeta Ganpule, MSc. Signed /- 03-06-2006
Quality Manager Signature Date
STATEMENT OF QUALITY ASSURANCE UNIT
Project No.: 9165
Test Substance: Oxy-Powder®
Study Title :
ANTIMICROBIAL ACTIVITY TESTING OF OXY-POWDER® AGAINST 5 CULTURES
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Quality Assurance Unit of the testing facility inspected the conduct of study on the following dates
22-05-2006: Preparation and sterilization of Media,
24-05-2006: Inoculation with relevant organism, transfer to sterile Petri Plates and boring of cups.
25-05-2006: Test solution preparation, addition to cups in LF unit and incubation.
29-05-2006: Incubation Result
31-05-2006: Raw data audit:
03-06-2006: Final report audit
No inspection led to findings which had to be reported to the management / sponsor or would have
impaired this study in any way.
Miss Nameeta Ganpule, MSc signed /- 03-06-2006
Quality Manager Signature Date
PERSONNEL INVOLVED IN THE STUDY
Study Director : DR (MRS.) DEEPA BHAJEKAR, Ph.D.
Microbiologist : Miss Niveda Prabhu MSc.
Quality Manager Audit : Miss Nameeta Ganpule, MSc.
Introduction:
(Ref: Normal Gastrointestinal Tract Flora by Charles Patrick Davis in
"Microbiology of the Gastrointestinal Tract" ed. by Sherwood L. Gorbach Medmicro Chapter 6)
The stomach is a relatively hostile environment for bacteria. It contains bacteria swallowed with the
food and those dislodged from the mouth. Acidity lowers the bacterial count, which is highest
(approximately 103 to 106 organisms/g of contents) after meals and lowest (frequently undetectable)
after digestion. Some Helicobacter species can colonize the stomach and are associated with type B
gastritis and peptic ulcer disease. Aspirates of duodenal or jejunal fluid contain approximately 103
organisms/ml in most individuals. Most of the bacteria cultured (streptococci, lactobacilli,
Bacteroides) are thought to be transients. Levels of105 to about107 bacteria/mL in such aspirates
usually indicate an abnormality in the digestive system (for example, achlorhydria or malabsorption
syndrome). Rapid peristalsis and the presence of bile may explain in part the paucity of organisms in
the upper gastrointestinal tract. Further along the jejunum and into the ileum, bacterial populations
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
begin to increase, and at the ileocecal junction they reach levels of 106 to 108 organisms/mL, with
streptococci, lactobacilli, Bacteroides, and bifidobacteria predominating. Concentrations of 109 to 1011
bacteria / g of contents are frequently found in human colon and feces. This flora includes a
bewildering array of bacteria (more than 400 species have been identified); nonetheless, 95 to 99
percent belong to anaerobic genera such as Bacteroides, Bifidobacterium, Eubacterium,
Peptostreptococcus, and Clostridium. In this highly anaerobic region of the intestine, these genera
proliferate, occupy most available niches, and produce metabolic waste products such as acetic,
butyric, and lactic acids. The strict anaerobic conditions, physical exclusion (as is shown in many
animal studies), and bacterial waste products are factors that inhibit the growth of other bacteria in the
Although the normal flora can inhibit pathogens, many of its members can produce disease in
humans. Anaerobes in the intestinal tract are the primary agents of intra-abdominal abscesses and
peritonitis. Bowel perforations produced cancer, infarction, byappendicitis, surgery, or gunshot
wounds almost always seed the peritoneal cavity and adjacent organs with the normal flora.
Anaerobes can also cause problems within the gastrointestinal lumen. Treatment with antibiotics may
allow certain anaerobic species to become predominant and cause disease. For example, Clostridium
difficile, which can remain viable in a patient undergoing antimicrobial therapy, may produce pseudo
membranous colitis. Other intestinal pathologic conditions or surgery can cause bacterial overgrowth
in the upper small intestine. Anaerobic bacteria can then deconjugate bile acids in this region and bind
available vitamin B12 so that the vitamin and fats are malabsorbed. In these situations, the patient
usually has been compromised in some way; therefore, the infection caused by the normal intestinal
flora is secondary to another problem.
More information is available on the animal than the human micro flora. Research on animals has
revealed that unusual filamentous microorganisms attach to ileal epithelial cells and modify host
membranes with few or no harmful effects. Microorganisms have been observed in thick layers on
gastrointestinal surfaces (Fig. 6-3) and in the crypts of Lieberkuhn. Other studies indicate that the
immune response can be modulated by the intestinal flora. Studies of the role of the intestinal flora in
biosynthesis of vitamin K and other host-utilizable products, conversion of bile acids (perhaps to co-
carcinogens), and ammonia production (which can play a role in hepatic coma) show the dual role of
the microbial flora in influencing the health of the host. Additional basic studies of the human bowel
flora are necessary to define their effect on humans.
The micro ecology of the human gastrointestinal tract is incredibly complex, as there are at least five
hundred different species of micro flora that are part of the normal intestinal flora. There are nine
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
times as many bacteria in the gastrointestinal tract as there are cells in the human body. The type and
number of the gut bacteria play an important role in determining health and disease in the human
body. Probiotics are beneficial micro organisms like Lactobacillus, Bifidobacteria, and Streptococcus
in human intestinal tract. They manufacture vitamins, especially B vitamins like biotin, niacin, folic
acid and B6 that detoxify chemicals and metabolize hormones. They empower enzymes that
maximize food assimilation and digestion. A state of altered bacterial flora in the gut is known as
Dysbiosis.
• Probiotics boost immune response by inhibiting growth of pathogenic organisms
• Probiotics detoxify the intestinal tract by protecting intestinal mucosa levels
• Probiotics develop a barrier to food-borne allergies
• Probiotics neutralize antibiotic-resistant strains of bacteria
• Probiotics reduce cancer risk
• Probiotics reduce the risk of inflammatory bowel disease (IBS) and Diverticulosis
• Probiotics synthesize needed vitamins for healing
• Probiotics prevent Diarrhea by improving digestion of proteins and fats.
Intestinal Flora / Probiotics Supportive Information
A large body of evidence over the past 75 years has demonstrated the preventive health value of
eating foods fermented with Lactobacilli or Bifidobacteria. These beneficial bacteria are referred
to as Probiotics. Probiotic bacteria are considered "friendly" bacteria. They are an essential
component of a healthy gastrointestinal tract as they inhibit the growth of harmful bacteria, boost
immune function, decrease infection in the digestive tract, and enhance digestion through enzyme
production. There are numerous species of lactobacilli and many strains for each species. The most
well known of these, Lactobacillus acidophilus and Bifidobacteria are normal inhabitants of the
human digestive tract. Others, like L. bulgaricus and L. Salivarius are not. These organisms, though,
still play an important role in maintaining the proper ratio of "friendly" organisms in the bowel by
producing "bacteriocins" chemicals that destroy harmful (unfriendly) bowel organisms.
Acidophilus and bifidobacteria maintain a healthy balance of intestinal flora by producing organic
compounds such as lactic acid, hydrogen peroxide and acetic acid. These compounds increase the
acidity of the intestine and inhibit the growth of less desirable organisms that fair poorly in this acidic
environment. By occupying an ecological niche in the intestine, they further limit the growth of
opportunistic organisms.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
A number of studies have demonstrated benefit of supplementation with Probiotics. The Annals of
Internal Medicine published a study which showed that Lactobacillus ingestion reduced and
prevented vaginal yeast infections in women. Lactobacillus has also demonstrated positive benefits in
irritable bowel syndrome (IBS). In a recent study, increasing levels of bifidobacteria reduced the
count of Clostridium, a pathogenic disease causing bowel organism. Lowering of the level of
Clostridium reduced the amount of large bowel toxic chemicals believed to promote cancer. Also, the
incidence of "traveller's Diarrhea," which is caused by pathogenic bacteria can be reduced by
preventive use of probiotics. It is also important to utilize Probiotics after antibiotic use as re-
colonizing the intestine may reduce post antibiotic infection in the digestive tract by fifty percent.
The choice of Probiotics is very important. It should be manufactured using highly viable, stable
strains of organisms that survive passage through the digestive tract and take up residence in the GI
Side Effects: There are no known side effects with the use of probiotics.
References:
De Simone C, Vesely R, Bianchi SB, et al. The role of probiotics in modulation of the immune system
in man and in animals. Int J Immunotherapy 1993; 9:23–28.
2. Rasic JL. The role of dairy foods containing bifido and acidophilus bacteria in nutrition and health.
N Eur Dairy J 1983 4:80–88.
3. Barefoot SF, Klaenhammer TR. Detection and activity of Lactacin B, a Bacteriocin produced by
Lactobacillus acidophilus. Appl Environ Microbiology 1983; 45:1808–15.
4. Hilton E, Isenberg HD, Alperstein P, et al. Ingestion of yogurt containing Lactobacillus acidophilus
as prophylaxis for Candida vaginitis. Ann Int Med 1992; 116:353–57.
5. Elmer GW, Surawicz CM, McFarland LV. Bio-therapeutic agents. JAMA 1996; 275(11):870–76.
6. Scarpignato C, Rampal P. Prevention and treatment of traveller's Diarrhea: A clinical
pharmacological approach. Chemotherapy 1995; 41:48–81.
7. Golledge CL, Riley TV. "Natural" therapy for infectious diseases. Med J Austral 1996; 164: 94–95
8. Newcomer AD, Park HS, O'Brian PC, et al. Response of patients with irritable bowel syndrome
and lactase deficiency using unfermented acidophilus milk. Am J Clinical Nutr 1983; 38:257–263.
9. D Bagchi and SK Dash, Lactobacillus Acidophilus- Natural Antibiotics and Beyond, Townsend
Letter 78-82, 1996.
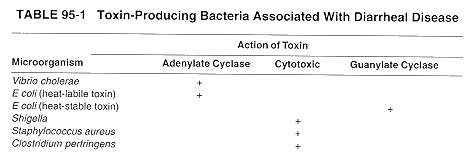
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Diseases Caused by Overgrowth of Potential Pathogens
Bacterial Diarrhea
Enterotoxin-Mediated Diarrhoeal Diseases
Several enterotoxin-producing bacteria cause Diarrhea diseases (Table 95-1). The Diarrhea disease
caused by Vibrio cholerae and enterotoxigenic strains of E coli has three main characteristics. First,
there is intestinal fluid loss that is related to the action of an enterotoxin on the small bowel epithelial
cells. Second, the organism itself does not invade the mucosal surface; rather, it colonizes the upper
small bowel, adhering to the epithelial cells and elaborating the enterotoxin. The mucosal architecture
remains intact with no evidence of cellular destruction. Bacteremia does not occur. Third, the fecal
effluent is watery and often voluminous, so that the Diarrhea can result in clinical dehydration. The
fluid originates in the upper small bowel. where the enterotoxin is most active.
The paradigm of the enterotoxigenic Diarrhea diseases is cholera in which stool volume can exceed 1
L / hour, with daily fecal outputs of 15 to 20 L if the patient is kept hydrated. Cholera is caused by V
cholerae, which is usually ingested in contaminated water. Vibrios that survive passage through the
stomach colonize the surface of the small intestine, proliferate, and elaborate the enterotoxin. Cholera
toxin acts via adenylate cyclase to stimulate secretion of water and electrolytes from the epithelial
cells into the lumen of the gut. The duodenum and upper jejunum are more sensitive to the toxin than
the ileum is. The colon is relatively insensitive to the toxin and may still absorb water and electrolytes
normally. Thus, cholera is an "overflow Diarrhea," in which the large volumes of fluid produced in
the upper intestine overwhelm the resaborptive capacity of the lower bowel. Cholera stool is described
as resembling rice watery clear fluid flecked with mucus and is isotonic with plasma. Microscopy
reveals no inflammatory cells in the fecal effluent; all that can be seen are small numbers of shed
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Enterotoxigenic Ecolab Diarrhea
Certain strains of E. coli cause Diarrhea disease by elaborating enterotoxins. These strains produce
two types of enterotoxins. One, called heat-labile toxin, similar in structure and in its mechanism of
action to cholera toxin. The other, called heat-stable toxin appears to act via guanylate cyclase.
Enterotoxigenic E coli strains are the most common cause of travelers' Diarrhea
Other Diarrhea causing toxins: Many strains of Shigella produce an enterotoxin, called
Shiga toxin that causes secretion of fluid from the small intestine. Shiga toxin has a
destructive, cytotoxic effect on the small-bowel epithelium, causing gross injury to the bowel
surface. It does not activate adenylate cyclase. E coli 0157:H7, the organism associated with
consumption of undercooked chopped meat, also produces a Shiga-like toxin; it causes
bloody Diarrhea and colitis. An organism that produces a different type of cytotoxic is Vibrio
parahaemolyticus, a bacterium associated with seafood. Food-poisoning strains of
Staphylococcus aureus and Clostridium perfringens both produce enterotoxins that are
cytotoxic. The staphylococcal enterotoxin also has a direct effect on the vomiting center in
the brain.
Gastrointestinal Disease Caused by Invasive Bacteria
Unlike the enterotoxigenic organisms, invasive bacteria exert their main impact on the host by causing
gross destruction of the epithelial architecture; histological findings include mucosal ulceration and an
inflammatory reaction in the lamina propria. The principal pathogens in this group are Salmonella,
Shigella, Campylobacter, invasive E coli, and Yersinia. The enteric viruses also invade intestinal
epithelial cells, but the extent of mucosal destruction is considerably less than that caused by invasive
bacterial pathogens.
Salmonella Enteritis
Salmonella species are a common cause of food poisoning. The main site of attack is the lower ileum,
where the salmonellae cause mucosal ulceration. They rapidly make their way through the epithelial
surface into the lamina propria and enter the lymphatic stream and bloodstream. At least two
virulence factors are associated with intestinal infection: one responsible for mucosal invasion, and
the other causing secretion of fluid and electrolytes into the bowel.
Shigella Dysentery
Shigella organisms cause bacillary dysentery, an invasive Diarrhea disease of the lower bowel in
which the stool contains inflammatory exudates composed of polymorpho-nuclear leukocytes. The
bacilli invade the epithelium of the colon and cause superficial ulceration. This invasive process
depends on the presence of two virulence factors. The first mediates the initial penetration of the
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
mucosal surface by destroying the brush border; the bacteria are subsequently engulfed by
invagination of the plasma membrane. The second virulence factor allows the organism to multiply
within the mucosal tissue. Mucosal ulceration accompanied by an intense inflammatory response in
the lamina propria results. The infection is usually restricted to the mucosa and lymph node
involvement; Bacteremia is uncommon.
REFERENCES
Finegold S (ed): Centennial symposium on anaerobes: A memorial to Andre' Veillon. Clin Infect Dis
Goldin BR, Lichtenstein AH, Gorbach SL: The role of the intestinal flora. p. 500. In Shils M.E,
Young VR (eds.): Modern Nutrition in Health and Disease. Lea & Febiger, Philadelphia, 1994
Gorbach SL: Infectious Diarrhea and bacterial food poisoning. p. 1128 In Sleisenger MH, Fordtran JS
(eds.): Gastrointestinal Diseases. WB Saunders, Philadelphia, 1993.
Simon GL, Gorbach SL: Normal alimentary tract micro flora. p. 53. In Blaser MJ, Smith PD, Ravdin
JI, Greenberg HB, Guerrant RL (eds.): Infections of the Gastrointestinal Tract, Raven Press, New
SUMMARY AND CONCLUSION
SUMMARY: The objective of this study was to assess the in-vitro effect of Oxy-Powder® on the
normal Probiotic strains and colonies of microbes generally present in the flora of human gig tract.
The study was designed to include 3 strains of pathogenic bacteria namely Escherichia coli,
Staphylococcus aureus and Enterobacter faecalis; one Probiotic organism Lactobacillus bifidigus and
one species of a parasite, Candida albicans. The experimental work involved use of Cup plate
technique in two sets (one for the test substance and the other for reference control) employing
relevant media previously inoculated with the specific culture. Positive control plate comprising of
inoculated medium in Petri plates was also incubated to indicate suitability of media to support the
growth of cultures along with Negative control plates containing sterilized medium to validate
sterility of the medium. All the operations were performed under sterile conditions to avoid entry of
contaminating microbes. The procedure used (a)contents of one capsule of Oxy-Powder® (715.5 mg)
dissolved in 60 mL sterile distilled water and (b)25 mg citric acid dissolved in 60 mL sterile distilled
water as a control since citric acid present in Oxy-Powder® could also inhibit growth of microbes.
Since Oxy-Powder® acted in vivo by liberation of nascent oxygen, prepared solution of Oxy-
Powder® was added to the cups at five different intervals namely 0 minute, 15 minutes, 30 minutes,
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
45 minutes and 60 minutes. The plates were incubated at 37OC for 72-96 hours and recording growth
CONCLUSION: The in vitro experiments did not exhibit inhibition at the given concentration of
Oxy-Powder® against the five test cultures Escherichia coli, Staphylococcus aureus, Lactobacillus
bifidigus, Enterobacter faecalis and Candida albicans at the given time intervals indicating thereby
that even the Probiotic culture, Lactobacillus bulgaricus will also probably not be killed by Oxy-
Powder® when the latter is used in the patients suffering from constipation and IBS.
NOTE: 1) The results relate only to the items tested.
2) This report shall not be reproduced except in full, without the written approval of the
Title: ANTIMICROBIAL ACTIVITY OF OXY-POWDER® AGAINST 5 CULTURES
Sponsor: Mayfair Clinical Education and Research Centre, Mumbai
Monitoring Scientist: Dr. J. K. Lalla
Testing Facility: THE MICRO CHEM LABORATORY
125, VARDHMAN INDUSTRIAL ESTATE,
GOKUL NAGAR, THANE (W) 400 601
Project No. 9165
Test Substance Oxy-Powder®
Schedule:
15-05-2006 Date of receipt 0f Samples
22-05-2006, Preparation and sterilization of Media,
24-05-2006, Inoculation with relevant organism, transfer to sterile Petri Plates and boring of
25-05-2006, Test solution preparation, addition to cups in LF unit and incubation.
29-05-2006, Incubation Results
31-05-2006 Raw data audit:
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
03-06-2006 Final report audit:
Objective
The objective of this study was to assess the in-vitro effect of Oxy-Powder® on the normal Probiotic
strains and colonies of microbes generally present in the flora of human gig tract
MATERIALS AND METHODS
TEST SUBSTANCE
Sponsor: Mayfair Clinical Education and Research Centre, Mumbai
Label on Sample: Oxy-Powder®
Characteristics of Sample :
Consistency: Solid (Capsule)
Color: White
Disclaimer: The above physicochemical data of test substance is supplied by the Sponsor. All
responsibility with regards to the accuracy and authenticity of this information remains with the
Sponsor. The test laboratory is not responsible for any variations with the batch number supplied.
SUMMARY REPORT ON IN-VITRO ANTI BACTERIAL ACTIVITY OF
OXY-POWDER® (4 ORGANISMS + 1 PARASITE)
The Microbiological testing was done by observing following conditions:
Test Organisms:
Pathogens: Escherichia coli, Staphylococcus aureus, Enterobacter faecalis, Candida
albicans,
Probiotic organism: Lactobacillus bifidigus
Test Method: Cup plate technique.
Concentrations: 1 capsule dissolved in 60 ml sterile distilled water.
25 mg citric acid dissolved in 60 ml sterile distilled water.
1 (Citric acid was included since Oxy-Powder® generates O2 and is active only in acidic
Frequency of analysis:
0 minute, 15 minutes, 30 minutes, 45 minutes and 60 minutes.

MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
No inhibition was observed at the given concentration against the five test cultures
Escherichia coli, Staphylococcus aureus, Lactobacillus bifidigus, Enterobacter faecalis and
Candida albicans at the given time intervals.
Conclusion:
The results very clearly indicate that Oxy-Powder® is ineffective in killing the test cultures.
It is very encouraging to see that the Probiotic organisms Lactobacillus bulgaricus is also not
killed by Oxy-Powder® indicating thereby the survival of Probiotic organisms even when Oxy-
Powder® is acting in large intestine and colon region against constipation. Other normal
physiological processes including generation of B complex factors by the Probiotic organisms
shall continue in routine and would avoid administration of B complex factors externally to the
patients suffering from constipation and undergoing treatment with Oxy-Powder®.
Signed /-
Prof. J. K. Lalla, Ph.D.
Study Director
REPORT FOR
CLINICAL TRIAL PHASE III (CONSTIPATION)
SAFETY AND EFFICACY OF OXY-POWDER®
DOCUMENT NO.: MCERC/REPT-CLTR/OXY/1205/001
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
May 30th 2007
TRIAL TO STUDY THE SAFETY AND EFFECTIVENESS
OF OXY-POWDER® IN TREATING CONSTIPATION AND IBS.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE, (A KALTHIA GROUP ORGANIZATION)
Mohan Mill Compound, Ghodbunder Road, Thane-400 607 Ph: No. 91-022-2589 5856 Fax: 91-022-2589 5854 Email: [email protected] / [email protected]
Part – 4 A
CLINICAL STUDY REPORT
ON OXY-POWDER®
CLINICAL STUDY REPORT ON OXY-POWDER®―CONSTIPATION
Table of Contents
TITLE PAGE
ABSTRACT
TABLE OF CONTENTS
SYNOPSIS
ADMINISTRATIVE STATEMENTS
(A) Glossary
(B) Regulatory Approvals
(C) Statement of final approval of the report by Study
director, statistician, investigators, etc.
1.0 INTRODUCTION
1.1 Constipation
1.2 IBS
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
1.3 Introduction to Rome II Criteria
1.31 Rome II Criteria for Constipation
1.32 Rome II Criteria for IBS
2.1-2.2 IBS diagnosis
2.3 Red Flag Symptoms(not of IBS)
3.1 Oxy-Powder®
3.1.1 Germanium-132
3.2 Bisacodyl
4.0 RATIONALE
4.1 OBJECTIVES OF THE STUDY
5.0 METHODOLOGY
5.1-5.1.1 Conduct ( Including Ethical Conduct ) of Study
5.1.2 Subject Information and Consent
6.0 Investigators, Study Centres and Admin. Structure
7.0-7.1 Study Design, Duration and Conduct of Study
7.2 Study Population
7.3 No. of Patients enrolled
8.0 Patient selection, inclusion and Exclusion Criteria
8.3 Other Eligibility Criteria
9.0Treatment and Timings
9.1 Dosage and Administration
9.2 Comparative Product (B)
9.3 Study Population
9.4 Study Assessment
9.4.1 Study Procedure and Treatment
9.5 End Points
10.0 Demography
Grading of Response
11.0Efficacy
12.0 Safety
13.0 Withdrawal from study
14.0 Statistics and data handling
16.0 Ethics
17.0 Ethical Conduct and Approval of Studies
17.1 Informed Consent
Protocol compliance
10 Results
(a) Descriptive
(b) Efficacy
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
(c) Safety
11 Discussions
12 Conclusions
LIST OF TABLES (Constipation)
1 Demographic
3 Smoking
Duration of Constipation (in months)
No. Of Bowels in a Week for OP and DL on day 0
for Classifying Patients before study commenced
Severity of Constipation
7 Randomization
Comparison of Weight (kg) (Day 0-Day 42)
No. Of Bowels in a Week (Day 0, 21 and 42) to evaluate
Efficacy
Oxygen Content of Blood (Day 0, 21 and 42)
Straining During >25% of Bowel Movement [ (a) Day
0,(b)Day21,(c) Day 42) ]
Lumpy Stools [(a) Day 0, (b) Day21 and (c) Day42]
13 Sensation
incomplete
evacuation for >25% of Bowel
Movement[(a)Day 0, (b) Day 21 and (c) Day 42)]
Sensation of Anorectal Blockage for >25% of Bowel
Movement.[(a)Day 0, (b) Day 21 and (c) Day 42)]
Manual Manoeuvres to facilitate >25% of Bowel
Movements[(a)Day 0, (b) Day 21 and (c) Day 42)]
Overall Efficacy-(A) Assessment By Investigators
(B) Assessment By Patients
Comparison of Efficacy of Oxy-Powder® with Dulcolax
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
APPENDICES
World Medical Association – Declaration of Helsinki,1964
IRB Bhatia Hospital
Protocol Oxy-Powder®– Version 02
5 Randomization
Patient's Informed Consent
ADMINISTRATIVE STATEMENTS
(A)GLOSSARY
ADVERSE EVENT: An unwanted effect caused by the administration of drugs. Onset may be
sudden or develop over time
BASELINE: 1. Information gathered at the beginning of a study from which variations found in the
study are measured. 2. A known value or quantity with which an unknown is compared when
measured or assessed. 3. The initial time point in a clinical trial, just before a participant starts to
receive the experimental treatment which is being tested. At this reference point, measurable values
such as CD4 count are recorded. Safety and efficacy of a drug are often determined by monitoring
changes from the baseline values.
BIAS: When a point of view prevents impartial judgment on issues relating to the subject of that point
of view. In clinical studies, bias is controlled by blinding and randomization.
BLIND: A randomized trial is "Blind" if the participant is not told which arm of the trial he is on. A
clinical trial is "Blind" if participants are unaware on whether they are in the experimental or control
arm of the study; also called masked.
CENTRAL DRUGS STANDARD CONTROL ORGANIZATION (CDSCO): Regulatory
authority under Directorate General of Health Services, Ministry of Health and Family Welfare,
Government of India responsible for (1)laying down standards of drugs, cosmetics, diagnostics and
devices and (2) regulating market authorization of new drugs and clinical research in India.
CLINICAL: Pertaining to or founded on observation and treatment of participants, as distinguished
from theoretical or basic science.
CLINICAL INVESTIGATOR: A medical researcher in charge of carrying out a clinical trial's
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
COMPLEMENTARY AND ALTERNATIVE THERAPY: Broad range of healing philosophies,
approaches, and therapies that Western (conventional) medicine does not commonly use to promote
well-being or treat health conditions. Examples include acupuncture, herbs, etc.
CONFIDENTIALITY REGARDING TRIAL PARTICIPANTS: Refers to maintaining the
confidentiality of trial participants including their personal identity and all personal medical
information. The trial participants' consent to the use of records for data verification purposes
should be obtained prior to the trial and assurance must be given that confidentiality will be
CONTRAINDICATION: A specific circumstance when the use of certain treatments could be
CONTROL: A control is the nature of the intervention control.
CONTROL GROUP: The standard by which experimental observations are evaluated. In many
clinical trials, one group of patients will be given an experimental drug or treatment, while the control
group is given either a standard treatment for the illness or a placebo
CONTROLLED TRIALS: Control is a standard against which experimental observations may be
evaluated. In clinical trials, one group of participants is given an experimental drug, while another
group (i.e., the control group) is given either a standard treatment for the disease or a placebo.
DOUBLE-BLIND STUDY: A clinical trial design in which neither the participating individuals nor
the study staff knows which participants are receiving the experimental drug and which are receiving
a placebo (or another therapy). Double-blind trials are thought to produce objective results, since the
expectations of the doctor and the participant about the experimental drug do not affect the outcome;
also called double-masked study.
EFFICACY: (Of a drug or treatment). The maximum ability of a drug or treatment to produce a
result regardless of dosage. A drug passes efficacy trials if it is effective at the dose tested and against
the illness for which it is prescribed. In the procedure mandated by the FDA, Phase II clinical trials
gauge efficacy, and Phase III trials confirm it
ELIGIBILITY CRITERIA: Summary criteria for participant selection; includes Inclusion and
Exclusion criteria.
ENDPOINT: Overall outcome that the protocol is designed to evaluate. Common endpoints are
severe toxicity, disease progression, or death.
FOOD AND DRUG ADMINISTRATION (FDA): The U.S. Department of Health and Human
Services agency responsible for ensuring the safety and effectiveness of all drugs, biologics, vaccines,
and medical devices, including those used in the diagnosis, treatment, and prevention of HIV
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
infection, AIDS, and AIDS-related opportunistic infections. The FDA also works with the blood
banking industry to safeguard the nation's blood supply.
HYPOTHESIS: A supposition or assumption advanced as a basis for reasoning or argument, or as a
guide to experimental investigation.
INCLUSION/EXCLUSION CRITERIA: The medical or social standards determining whether a
person may or may not be allowed to enter a clinical trial. These criteria are based on such factors as
age, gender, the type and stage of a disease, previous treatment history, and other medical conditions.
It is important to note that inclusion and exclusion criteria are not used to reject people personally, but
rather to identify appropriate participants and keep them safe.
IND: Investigational New Drug.
INFORMED CONSENT: The process of learning the key facts about a clinical trial before deciding
whether or not to participate. It is also a continuing process throughout the study to provide
information for participants. To help someone decide whether or not to participate, the doctors and
nurses involved in the trial explain the details of the study.
INFORMED CONSENT DOCUMENT: A document that describes the rights of the study
participants, and includes details about the study, such as its purpose, duration, required procedures,
and key contacts. Risks and potential benefits are explained in the informed consent document. The
participant then decides whether or not to sign the document. Informed consent is not a contract, and
the participant may withdraw from the trial at any time.
INSTITUTIONAL REVIEW BOARD (IRB): 1. A committee of physicians, statisticians,
researchers, community advocates, and others that ensures that a clinical trial is ethical and that the
rights of study participants are protected. All clinical trials in the U.S. must be approved by an IRB
before they begin. 2. Every institution that conducts or supports biomedical or behavioral research
involving human participants must, by federal regulation, have an IRB that initially approves and
periodically reviews the research in order to protect the rights of human participants.
INTENT TO TREAT: Analysis of clinical trial results that includes all data from participants in the
groups to which they were randomized even if they never received the treatment.
IRRITABLE BOWEL SYNDROME: Irritable bowel syndrome (IBS), a functional gastrointestinal
disorder characterized by the interplay of altered motility, abnormal visceral sensation, and
psychosocial factors, is one of the most common reasons for referral to a gastroenterologist.
MCERC: Mayfair Clinical, Education and Research Centre, Thane.
OPEN-LABEL TRIAL: A clinical trial in which doctors and participants know which drug or
vaccine is being administered.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
PHASE II TRIALS: Controlled clinical studies conducted to evaluate the effectiveness of the drug
for a particular indication or indications in patients with the disease or condition under study and to
determine the common short-term side effects and risks.
PHASE III TRIALS: Expanded controlled and uncontrolled trials after preliminary evidence
suggesting effectiveness of the drug has been obtained, and are intended to gather additional
information to evaluate the overall benefit-risk relationship of the drug and provide and adequate
basis for physician labelling.
PLACEBO: A placebo is an inactive pill, liquid, or powder that has no treatment value. In clinical
trials, experimental treatments are often compared with placebos to assess the treatment's
PLACEBO CONTROLLED STUDY: A method of investigation of drugs in which an inactive
substance (the placebo) is given to one group of participants, while the drug being tested is given to
another group. The results obtained in the two groups are then compared to see if the investigational
treatment is more effective in treating the condition.
PHARMACOVIGILANCE: Despite all the tests and precautions taken during the development and
authorisation of a pharmaceutical product, medicines still sometimes produce side effects under
certain conditions. Monitoring use and effects of a given medication to detect and prevent these
adverse drug reactions (ADR) is the domain of Pharmacovigilance.
It is regarded as all post-authorisation scientific and data gathering activities relating to the detection,
assessment, understanding and prevention of adverse events or any other product related problems.
PROTOCOL: A study plan on which all clinical trials are based. The plan is carefully designed to
safeguard the health of the participants as well as answer specific research questions. A protocol
describes what types of people may participate in the trial; the schedule of tests, procedures,
medications, and dosages; and the length of the study. While in a clinical trial, participants following
a protocol are seen regularly by the research staff to monitor their health and to determine the safety
and effectiveness of their treatment.
RANDOMIZATION: A method based on chance by which study participants are assigned to a
treatment group. Randomization minimizes the differences among groups by equally distributing
people with particular characteristics among all the trial arms. The researchers do not know which
treatment is better. From what is known at the time, any one of the treatments chosen could be of
benefit to the participant
RANDOMIZED TRIAL: A study in which participants are randomly (i.e., by chance) assigned to
one of two or more treatment arms of a clinical trial. Occasionally placebos are utilized.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
RISK-BENEFIT RATIO: The risk to individual participants versus the potential benefits. The
risk/benefit ratio may differ depending on the condition being treated.
SERIOUS ADVERSE EVENT: A Serious adverse event is any untoward medical occurrence that at
any dose a) results in death b) is life threatening c) requires hospitalization or prolongation of existing
hospitalisation.
SIDE EFFECTS: Any undesired actions or effects of a drug or treatment. Negative or adverse effects
may include headache, nausea, hair loss, skin irritation, or other physical problems. Experimental
drugs must be evaluated for both immediate and long-term side effects.
SINGLE-BLIND STUDY: A study in which one party, either the investigator or participant, is
unaware of what medication the participant is taking; also called single-masked study.
STATISTICAL SIGNIFICANCE: The probability that an event or difference occurred by chance
alone. In clinical trials, the level of statistical significance depends on the number of participants
studied and the observations made, as well as the magnitude of differences observed.
STUDY ENDPOINT: A primary or secondary outcome used to judge the effectiveness of a
STUDY TYPE: The primary investigative techniques used in an observational protocol; types are
Purpose, Duration, Selection, and Timing.
(B) REGULATORY APPROVALS
The study protocol, the informed consent, and other information that required pre-approval were
reviewed and approved by the Independent Ethics Committee (IEC) of Mayfair Clinical, Education
and Research Centre and Institutional Review Board (IRB) of Bhatia General Hospital. A letter along
with the Protocol and IEC approval letter was sent to Drugs Controller General of India at Central
Drugs Standard Control Organization (CDSCO) office, New Delhi informing him about MCERC
conducting Multicentric Clinical Trial, Phase III studies
In this study, Good Clinical Practices described under ICH E6 document, IEC notifications pertaining
to Good Clinical Practice (GCP) Guidelines issued by CDSCO and Ethical Guidelines for Biomedical
Research on Human Subjects, issued by Indian Council of Medical Research, have been followed.
Appendixes 2–4 contain the study protocol, and details pertaining to the IECs.
(C) INVESTIGATOR'S DECLARATION
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Statement of Final Approval of Clinical Report
PROTOCOL NO.: MCERC/REP.CLTR/OXY/1207/001
We, the undersigned, have read and understood this report and hereby assure that the study
was conducted in accordance with the approved protocol and SOP's in compliance with all
the requirements regarding the obligations of investigators and all other pertinent
requirements of the ICH (E-3 and E-6 Guidelines) 'Guidance on Good Clinical Practice',
Declaration of Helsinki (Hong Kong, 1989) and national guidelines. We further undertake
that all the essential documents and the Investigational product pertaining to this study will be
archived for a period of 3 years on submission of the report to the sponsor.
Investigator-1 Investigator-2 Statistician
Name Prof. J. K.
Dr.Chetan Bhatt Mr. Vinayak
(D) QA STATEMENT
Protocol No.: MCERC/REP.CLTR/OXY/1207/001
Title: Efficacy & Safety of Oxy-Powder®
Objective: To study the safety and efficacy of Oxy-Powder® in patients of chronic constipation and IBS.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Randomized, open, comparative study involving
1) 40 patients, both females and males [having non-vegetarians, and vegetarian food habits] suffering
from constipation
2) 20 patients, both females and males (having non-vegetarians, and vegetarian food habits) suffering
from IBS associated with constipation
The Quality Assurance Auditor of Mayfair Clinical, Education & Research Centre audited conduct of
clinical Trial PROTOCOL NO,MCERC/REP.CLTR/OXY/1207/001 and verified that it was
conducted in accordance with the Protocol approved by the IEC and the sponsor, Good Clinical
Practice, Good Laboratory Practices and other applicable regulations and implemented internal
standard operating procedures. The study commenced only after the Regulatory and other approvals
The study was audited and data verified on the following dates:
06, 07, 08, 14, 16, 30 and 31 August 2006,
01, 11 and September 2006 and
13, 14 and 15 March 2007.
Dr. Mrs Meena U. Shah
QA Auditor Date: 30th May 2007
(E) APPROVAL OF REPORT BY STUDY DIRECTOR
Title of the Study:
Randomized, open, comparative trial to study Safety and Efficacy of Oxy-Powder® Marketed by
Global Healing Centre, Inc. USA in treating constipation and IBS to be compared with Dulcolax.
I have read this report and confirm that to the best of my knowledge, it accurately describes the
conduct and results of study.
Prof. J.K. Lalla, PhD Date: 30th May 2007
Study Director
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
(F) APPROVAL OF STUDY REPORT BY CO-COORDINATOR AND MONITOR,
CLINICAL PHARMACOLOGIST, AND Q.A. DIRECTOR
Title of the Study:
Randomized, open, comparative trial to study Safety and Efficacy of Oxy-Powder® Marketed
by Global Healing Centre, Inc. USA in treating constipation and IBS to be compared with
I have read this report and confirm that to the best of my knowledge, it accurately
describes the conduct and results of study.
Dr. (Mrs.) Meena U. Shah Date: 30th May 2007
[Co-Coordinator, Monitor, Clin. Pharmacologist and Q.A. Director]
(G) APPROVAL OF STUDY REPORT BY BIOSTATISTICIAN
Title of the Study
Randomized, open, Multicentric, comparative trial to study Safety and Efficacy of Oxy-Powder®
Marketed by Global Healing Centre, Inc. USA in treating constipation and IBS to be compared
I have read this report and confirm that to the best of my knowledge, it accurately describes the
results of study.
Vinayak Deshpande Date: 30th May 2007
(Biostatistician)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Contributors to the Study
Prof. J.K. Lalla, Ph.D. – Study Director
CLINICAL TRIAL
1) Dr. Sharad C. Shah – Gastroenterologist and Clinical Investigator – Jaslok Hospital
2) Dr. Chetan B. Bhatt – Gastroenterologist and Clinical Investigator – Bhatia General
3) Chairperson and members – Independent Ethics Committee of MCERC
4) Chairperson and members – Institutional Review Board of Bhatia General Hospital
5) Dr. Meena U. Shah – Mayfair Clinical, Education and Research Centre
6) Dr. Deven Parmar – Mayfair Clinical, Education and Research Centre
7) Ms. Neeta Mote– CRA, Mayfair Clinical, Education and Research Centre
8) Mr. Kamlesh Mote– Documentation Assistant, Mayfair Clinical, Education and
1.0 Introduction
1.1 Constipation:
Constipation is the slow movement of faeces (stool or body wastes) through the large intestine
resulting in infrequent bowel movements and the passage of dry, hard stools. The longer it takes for
the stool to move through the large intestine, the more fluid is absorbed and the drier and harder the
stool becomes. Constipation is annoying and uncomfortable, but fecal impaction (a collection of dry,
hard stool in the colon or rectum) can be life-threatening. Patients with a faecal impaction may not
have gastrointestinal symptoms; instead they may have circulation, heart, or breathing problems. If
fecal impaction is not recognized, the signs and symptoms will get worse and the patient could die.
Chronic constipation is one of the most frequent gastrointestinal symptoms in the Unites States,
accounting for nearly 2.5-2.7 million physician visits and 3900-90000 hospitalizations per year.
1.2 Irritable Bowel Syndrome (IBS):
Irritable bowel syndrome (IBS), a functional gastrointestinal disorder is characterized by the interplay
of altered motility, abnormal visceral sensation, and psychological factors. It is one of the most
common reasons for referral to a gastroenterologist. It is associated with bouts of constipation and
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
1.3 Introduction to Rome II criteria:
At the 13th International Congress of Gastroenterology in Rome, Italy in 1988, a group of physicians
defined criteria to more accurately diagnose constipation and IBS. Known as the "Rome Criteria," this
set of guidelines that outlines symptoms and applies parameters such as frequency and duration make
possible a more accurate diagnosis of Constipation and IBS.
The Rome Criteria were not widely accepted when originally presented, but were better received after
their first revision. This second version, created in 1992 and known as Rome II, added a length of
time for symptoms to be present and pain as an indicator. The second revision, known as Rome III, is
currently underway
1.31 Rome II Criteria for Constipation:
Two or more of the following for at least 12 wk (not necessarily consecutive) in the preceding 12 mo:
Straining during >25% of bowel movements;
Lumpy or hard stools for >25% of bowel movements;
Sensation of incomplete evacuation for >25% of bowel movements;
Sensation of anorectal blockage for >25% of bowel movements;
Manual maneuvers (digital evacuation, support of the pelvic floor) to facilitate >25% of
bowel movements;
Less than 3 bowel movements per week;
Loose stools are not present, and there are insufficient criteria for irritable bowel syndrome
Acceptable form of birth control being followed in female patients
1.32 Rome II criteria for IBS:
The Rome II diagnostic criteria of Irritable Bowel Syndrome always presumes the absence of a
structural or biochemical explanation for the symptoms and is made only by a physician.
Irritable Bowel Syndrome can be diagnosed based on at least 12 weeks (which need not be
consecutive) in the preceding 12 months, of abdominal discomfort or pain that has two out of three of
these features:
1. Relieved with defecation; and/or
2. Onset associated with a change in frequency of stool; and/or
3. Onset associated with a change in form (appearance) of stool.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
2.1 Symptoms that Cumulatively Support the Diagnosis of IBS:
1. Abnormal stool frequency (may be defined as greater than 3 bowel movements per day and less
than 3 bowel movements per week);
2. Abnormal stool form (lumpy/hard or loose/watery stool);
3. Abnormal stool passage (straining, urgency, or feeling of incomplete evacuation);
4. Passage of mucus;
5. Bloating or feeling of abdominal distension.
2.2 Supportive Symptoms of IBS:
1. Fewer than three bowel movements a week
2. More than three bowel movements in a day
3. Hard or lumpy stools
4. Loose (mushy) or watery stools
5. Straining during a bowel movement
6. Urgency (having to rush to have a bowel movement)
7. Feeling of incomplete bowel movement
8. Passing mucus (white material) during a bowel movement
9. Abdominal fullness, bloating, or swelling
2.3 Red Flag symptoms which are NOT typical of IBS:
Pain that often awakens/interferes with sleep
Diarrhoea that often awakens/interferes with sleep
Blood in your stool (visible or occult)
Abnormal physical examination
3.1 OXY-POWDER®: Oxy-Powder® is marketed by Global Healing Centre, Inc. USA
Category: Dietary Supplement
Composition: Ozonated Magnesium Oxides: (685 mg per capsule)
A combination of USP grade Magnesium Oxide mixed with a small amount USP grade Magnesium
Peroxide. This combination is then pressurized at subzero temperatures and Ozone gas is the
stabilizing molecule. The final product contains Stabilized monatomic oxygen, which is released by
an acid based catalyst i.e. HCl in the stomach.
Organic Germanium 132: (5.5 mg per capsule)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Does not contain the harmful form of Germanium (Germanium Dioxide)
Natural Citric acid: (25 mg per capsule)
Filled in Kosher certified "00" Vegetarian Capsules
Oxy-Powder® is a specifically designed compound which has been ozonated and stabilized to release
beneficial free monatomic oxygen into the intestinal tract. The time-release delivery ensures that Oxy-
Powder will provide an adequate amount of oxygen, slowly, for better utilization by the body. Oxy-
Powder is a non-toxic, sate, effective and non-allergic. By using Oxy-Powder, the compaction from
the small intestine, large intestine and colon gets oxidized safely and effectively. Organic Germanium
– 132 has demonstrated in multiple scientific studies to be a powerful oxygen facilitator and immune
system stimulant. Oxy-Powder is also harmless to the good bacteria in the intestinal tract and Natural
citric acid has been added to facilitate oxygen release.
There is only one true way to clean the digestive tract. This is through an oxidation/reduction reaction
or a clean raw food diet. As we age, we accumulate toxic substances in our digestive tract. The
pancreas, the organ which produces the necessary enzymes to break down the food we eat, is limited.
At birth our pancreas has a limited supply of enzymes. Some doctors say we only have enough
enzymes to breakdown 1 cooked meal daily for 120 years. This means 80% of our diet should be raw
fruits and vegetables.
With the poor diet, particularly non-vegetarian food i.e. eating high fat meals daily, which the body
cannot utilize, tremendous strain is put on pancreas that secrete digestive enzymes by the time one is
30-40 years old. It can take the body up to 8 hours to break down proteins, and up to 48-72 hours to
digest fats and carbohydrates. Thus, one constantly has undigested food particles in the intestinal tract.
It has been estimated that the average person by the age of 40 has between 10-20 pounds of hard
compacted faecal matter lodged in their intestinal tract. Human intestinal tract is 30-35 feet in length.
In order to fully cleanse the digestive tract, the solid compaction gets into a liquid or gas, using time
released oxygen and ozone (oxidation/reduction). By using Oxy-powder, the toxic residue gets
oxidized from the small intestine, large intestine and colon, safely and effectively. This is important
because a clean intestinal tract is the beginning of obtaining optimal health.
Oxy-Powder is harmless to the Probiotic (helpful) bacteria in the intestinal tract. When the intestinal
tract is fully cleansed, the urine becomes cloudy and the stools become semi-solid. When this occurs,
a maintenance dose of Oxy-Powder® is recommended. This helps provide oxygen directly into the
bloodstream. By staying on a Maintenance Dosage of Oxy-Powder, the intestinal tract is kept clean
and provides body with much needed oxygen.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
OCCUPATIONAL SAFETY
Investigational product is not expected to pose significant occupational safety risk to site staff under
normal conditions of use and administration. A Material Safety Data Sheet (MSDS) describing
occupational hazards and recommended handling precautions was available upon request from
MCERC. End of Required Standard Wording.
However, precautions were expected to be taken to avoid direct contact with skin, eyes and generated
aerosols or mists. In case of unintentional occupational exposure, it was the responsibility of the
investigator to treat the patient or the staff in the normal course and report the incidence to the Study
Director, MCERC.
Concomitant Medications and Non-Drug Therapies
There are no contraindications reported when taking Oxy-powder with prescription medicines as long
as the Oxy-Powder® is taken 6 hours before or 6 hours after the. Permitted Medications
Investigators were requested to record all concomitant medications taken during the study by the
patient in the CRF with indication, dose information, and dates of administration.
Prohibited Medications
Laxatives, anti-diarrhoels and anti-spasmodics
3.1.1 GERMANIUM-132
Germanium is a metalloid element with atomic number 32 and atomic symbol Ge. Germanium is
found in the earth's crust, in certain minerals and in living matter such as plants and the human body.
Germanium is not an essential nutrient for humans.Organic germanium was first successfully
synthesized by Dr. Kazuhiko Asai of Tokyo, Japan. Dr. Asai found that organic germanium protects
against cancer by stimulating the production of interferon, a substance that stimulates the production
of natural killer (NK) cells, which directly combat cancer cells.
Typical daily dietary intakes of germanium range from about 0.4 to 1.5 milligrams. Plant foods, such
as wheat, vegetables, bran and leguminous seeds, are rich sources of germanium. Animal foods are
low in germanium.
The main nutritional supplement form of germanium is known as Ge-132, Germanium-132,
germanium sesquioxide or bis-carboxyethyl germanium sesquioxide. This is a synthetic organic
product. It has not been found naturally.
Bis-carboxyethyl germanium sesquioxide, Ge-132, may have antiproliterative activity. Ge-132 may
also have antioxidant activity and hence, useful in treatment of cancer.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
PHARMACOKINETICS
Organic Germanium compounds are rapidly absorbed and eliminated from the body without
undergoing metabolic alteration. Within one hour of administration, 50% of the compound is in the
gastrointestinal tract; after twelve hours, only 5% is there. Organic Germanium is reabsorbed by the
vena portae. One hour after administration, 50% is in the vena portae; after 8 hours, this figure rises to
85%, and by twelve hours, it is quasi complexed. Serum plasma levels reach a maximum two hours
after administration; in eight hours, Germanium is reduced by 80% of the maximum. Organic
Germanium, administered orally, has also been shown to be absorbed by about 30%, distributed
evenly throughout the body, leaving almost no residual concentration after twelve hours. It is
excreted, unchanged metabolically, in the urine in twenty-four hours. Germanium is ubiquitously
distributed in all organs - there are no specific target organs, and no differences in distribution patterns
detected between sexes. Organic Germanium is also eliminated at quite a rapid, linear rate, of
approximately 8% of the dose per hour, during the first eight hours. It is completely eliminated after
three days, mainly via the kidneys (85%). Germanium is soluble in the interstitial fluids, and is not
protein-bound. Germanium does not accumulate in any organ - no Germanium can be found in
animals one week after their removal from treatment.
Human Toxicity Studies
In human clinical trials with healthy volunteers, as well as patients who have participated in all the
studies described throughout this book, the toxicity of the particular organic Germanium compound
was assessed. One of the outstanding features of organic Germanium is its virtual non-toxicity and its
ability to be tolerated, in contrast to most highly toxic drugs. Organic germanium may cause minor
side effects, including skin rash and diarrhea.
Organic Germanium - Oxygen Enricher and Antioxidant
Stress, anxiety, fear, all can promote oxygen deficiency within the body Organic Germanium enriches
the body's oxygen supply and is also a potent antioxidant, properties which contribute to this trace
element's widespread beneficial effects upon many inter-related metabolic process in the body
Organic Germanium Enriches Oxygen Supply
The structure of organic Germanium, a crystalline lattice network extensively bonded with negative
oxygen ions, is said to actually substitute for oxygen, and to enable the attraction and elimination of
acidifying hydrogen ions, which detoxifies the blood. In the electron transport scheme during
oxidative metabolism, electrons are transferred along a set of electron acceptors, ending up, ultimately
with the combination of hydrogen and oxygen to form water. However, when there is an oxygen
deficiency, the loss of electrons can result in the accumulation of positive hydrogen ions, which lead
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
to blood acidification. Ge-132 has negatively charged oxygen ions, which can clear away these
hydrogen ions, and thus detoxify the blood.
3.2 Bisacodyl (Dulcolax):
Bisacodyl is a popular non-prescription type of stimulant laxative. The drug reduces short-term
constipation and is also used for preparing the colon or rectum for an examination or surgical
procedure. This over-the-counter laxative can be taken by mouth or per rectum for treating
Brand Name: Dulcolax, Fleet, Alophen, Correctol
Chemical Description: [4-[(4-acetyloxyphenyl)-pyridin-2-yl-methyl] phenyl] acetate
Structure of Bisacodyl:
WORKING:
Bisacodyl is a stimulant laxative. It causes muscles in the colon to contract and stools to pass.Bisacodyl
works by stimulating colon movement (peristalsis). Constipation is generally relieved within 15 minutes to
60 minutes after administration of a suppository form and in six to twelve hours after oral administration
The drug is taken at night, if administered orally, and during morning if taken through the rectum. The
drug is usually sold as 5mg tablets, 10mg suppositories, or 5mg pediatric suppositories
SIDE EFFECTS: This medication may cause stomachache, cramping, weakness, sweating, irritation of
the rectal areadizziness. Notify your doctor if you experience: chest pain, fainting, rectal
bleeding, lack of a bowel movement (especially after using this medicine). If you notice other effects not
listed above, contact your doctor or pharmacist.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
PRECAUTIONS: If you have any of the following conditions, do not take Bisacodyl without
consulting your doctor: severe nausea, vomiting, stomach/intestinal problems, recent abdominal
surgery, rectal bleeding, vitamin/mineral deficiencies, appendicitis, gastritis, an allergic reaction to
this medication. Frequent use of laxatives can cause
Symptoms can include muscle weakness or dizziness. Maintain adequate fluid intake
while using this medication. Before using Bisacodyl, tell your doctor if you are pregnant. It is not
known if Bisacodylmilk. Consult your doctor.
Note: Nursing and pregnant women should consult a doctor before taking the drug.
DRUG INTERACTIONS: Tell your doctor of all prescription and nonprescription drugs you may
use, especially of: potassium supplements, antacids, acid blockers (e.g., cimetidine, famotidine, and
ranitidine), other laxatives. Do not start or stop any medicine without doctor or pharmacist approval
OVERDOSE: If overdose is suspected, contact your local poison control center or emergency room
immediately. US residents can call the US national poison hotline at 1-800-222-1222. Canadian
residents should call their local poison control center directly. Symptoms of overdose may include
vomiting and loss of appetite, severe weakness, extreme
NOTES:drink 4 to 6 glasses of water daily, eat dietary
leafy substances and exercise regularly.
MISSED DOSE: If you miss a dose, skip the missed dose. Do not double the dose
STORAGE: Store at room temperature between 59 and 86o F (between 15 and 30o C) away from
moisture and sunlight. Do not store in the bathroom
USES: This medication is used to treat or to clean out the intestinal tract before bowel
examinations or bowel surgery.
HOW TO USE: Swallow the tablets whole with a full glass of water or juice. Do not crush or chew
the tablets. The tablets should work within 6 to 10 hours. Do not take the tablets within one hour of
taking any milk or dairy products. Severe stomach cramps and vomiting may occur. Bisacodyl should
not be used longer than seven days without consulting your doctor. Prolonged use can lead to laxative
dependence. Because this medication must be swallowed whole, do not give it to a child less than 6
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
4.0 Rationale:
The effectiveness of the product in treating constipation and IBS in patients following
Recording loss of weight
The effectiveness of the product for Oxygen delivery in patients
The effects Oxy-Powder has on the 4 microbes + 2 parasites present in the digestive
tract including normal Probiotic strain and colonies in the digestive tract.
Safety studies involving acute and sub-acute toxicity in rats/ mice (including
4.1 Objectives of the study:
To find the effectiveness and safety of Oxy-Powder® in treating constipation
5.0 METHODOLOGY:
5.1 Conduct of study:
Randomized, open, Multicentric, comparative trial to study Safety and Efficacy of Oxy-
Powder® Marketed by Global Healing Centre, Inc. USA in treating constipation to be
compared with Dulcolax.
The present study was conducted to clinically evaluate safety and effectiveness of Oxy-
Powder® in treating constipation and IBS–associated constipation precipitating loss of
weight & improving oxygen delivery in patients of constipation and IBS–associated
5.1.1 Ethical Conduct of the Study:
This study was conducted in accordance with the International Conference on Harmonisation
(ICH) Guidelines for GCP and all applicable regulatory requirements, including the
Declaration of Helsinki
5.1.2 Subject Information and Consent:
Written informed consent was obtained from each subject before the performance of any
study-specific procedures. The subject informed consent form used for this study is included
6.0 Investigators and Administrative Structure:
6.1 Investigators and Study Centres:
Subjects were enrolled in 2 centres. Following table presents the names of the investigators
and their respective centres.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Dr.Sharad.C.Shah
Dr.Sharad.C.Shah's Clinic
Dr. Chetan B. Bhatt
Bhatia General Hospital
6.2 Study Administrative structure:
The study was sponsored by Dr. Edward Group III, CEO, and Global Healing Center, Inc. &
contracted to Mayfair Clinical, Education & Research Centre, a Clinical Research
Organisation (CRO) for conduct of the study.
7.0 Design and conduct of the study:
7.1 Study Design and Duration:
RANDOMIZED, OPEN, MULTICENTRIC, COMPARATIVE TRIAL
The study was done as Multicentric, Open, Randomized study comparing efficacy and safety
of Oxypowder developed by Global Healing Centre Inc. USA with Dulcolax tablets
containing 5 mg Bisacodyl manufactured by Cadila Health Care Ltd.
The duration of study was 6 weeks from the date of administration of the study products.
7.2 STUDY POPULATION
Any subject, who has given informed consent to participate in the clinical study and has met
all the criteria required for inclusion into the clinical study, may take part in the research.
Subject participation in the research project is voluntary and refusal to participate will not
indicate withdrawal from the clinical study. Refusal to participate will involve no penalty or
loss of benefits to which the subject would otherwise be entitled.
No additional administration of investigational product beyond the dose detailed in the clinical study
7.3 Number of Patients enrolled:
40 patients (females + males+ geriatric patients), suffering from constipation
20 patients (females + males), suffering from IBS.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
8.0 PATIENT SELECTION
8.1 Inclusion Criteria for Constipation and IBS:
Patients suffering from constipation and IBS
Age - 18 to 60 yrs
Height & Weight conforming to Height/Weight chart of Life Insurance
Corporation of India
Sex – Patients belonging to both sexes were eligible
Food habits-both non-vegetarians and vegetarian patients were eligible (More of
the non-vegetarian patients were preferred).
Satisfied Rome II Criteria for Constipation and IBS
8.2 Exclusion Criteria for Constipation and IBS:
A subject was not considered eligible for inclusion in this study if any of the following
conditions were observed in the patient
1. Evidence of Malignancy on colonoscopy / having diagnosed organic gig disorder
2. Pregnant and lactating women
3. Evidence of lactose intolerance to explain bowel symptoms
4. History of cardiac arrhythmias or heart disease
5. History of Glaucoma
6. History of urine retention
7. History of schizophrenia
8. History of substances of abuse/dependency
9. Intellectually unable or unwilling to complete daily gig ratings
8.3 Other Eligibility Criteria Considerations:
To assess any potential impact on subject eligibility with regard to safety, the investigator
must refer to the following document(s) for detailed information regarding warnings,
precautions, contraindications, adverse events, and other significant data pertaining to the
investigational product(s) being used in this study.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
9.0 Treatment and Timings:
Test Product (A) – Oxy-Powder® capsules marketed by Global Healing Centre, Inc. USA
containing 715.5 mg Active in each capsule
Comparative Product (B) – Dulcolax tablets marketed by Cadila Healthcare Ltd, India
containing 5 mg Bisacodyl in each tablet.
9.1 DOSAGE & ADMINISTRATION:
The patients were divided in two (2) groups as per the Randomization schedule. Group1
was administered Product A while Group 2 was administered Product B
9.1.1 Test Product (A):
For first time, patients started with a seven-day initial cleansing procedure. After the initial
cleanse, a maintenance dose was continued for keeping intestinal tract clean and deliver
oxygen into the system. Patients were advised to take Oxy-Powder with plenty of potable
water during the day and eat healthy diet.
(a) For Cleansing:
Patients were directed by the investigators to take four (4) capsules in the evening on an
empty stomach with 240 mL water. If 3-5 bowel movements were not achieved the following
day, the dosage was increased by adding two (2) capsules every night until 3-5 bowel
movements were achieved the following day. The day on which the dosage was finalized was
considered as "day one (1)" of the seven (7) day cleansing cycle. This dosage was continued
for seven (7) consecutive days. After the seven (7) day cleansing cycle, the maintenance dose
(b) Maintenance Dose:
Patients were given capsules supplies for seven (7) days with instructions that they had be
taken as they did during cleansing cycle. For following 5 weeks, the same dosage was to be
repeated by the patients every other day. They were assured that the capsules were not habit
forming or harmful to the body and could be taken indefinitely.
9.2 Comparative Product (B):
Patients in this Group were directed by the investigators to take two tablets of Dulcolax (comparative
formulation) as per the Randomization scheme with plenty of water every day, for first 7 days, in the
evening on empty stomach. Thereafter, the subjects were instructed to take the same dose of Dulcolax
tablets on alternate days on empty stomach in the evening for 6 weeks.Administration on day ‘0', ‘3
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
weeks' and ‘6 weeks' was done on empty stomach (to enable measuring Oxygen levels) in the
morning. Subjects were asked to report to the hospital on empty stomach in the morning for
administration of Investigational products and Oxygen level in the blood was measured 15 minutes
and 30 minutes after administration of tablets/ capsules.On the remaining days, the subjects were
asked to take same dose of the Investigational product at their residence in the evening on empty
stomach followed by Dinner two hours post-administration of the dose.
9.3 Study Population:
40 patients (females + males+ geriatric patients), suffering from constipation
9.4 Study Assessments and General Procedure for both Products:
Treatment period– 6 weeks
9.4.1 Study Procedure and Treatment:
After selection the patients were subjected to detailed medical History and clinical
examination Patients then were subjected to the following pre-study evaluation :-
I.Record of weight,
II.Oxygen content of Blood This was done by using pulse oxcimeter,
III.Stool examination,
IV.Barium meal to rule out any Bowel organic lesion leading to constipation,
V.Colonoscopy to rule out any colonic organic lesion and any faecal impaction,
After ruling out the presence of any organic lesion, the patients were included in the study.
They were instructed to take four capsules of Oxy-Powder® (Test formulation) or two tablets
of Dulcolax (Comparative formulation), as per the Randomization scheme, with plenty of
water, every day, for first 7 days, in the evening on empty stomach. Thereafter, subjects were
instructed to take the same dose of either test of reference formulation on alternate days, on
empty stomach, in the evening, for period of 6 weeks.Administration on day '0', '3 weeks' and
'6 weeks' were done on empty stomach in the morning. Subjects were asked to report to the
hospital with empty stomach; in the morning for administration of investigational products
and Oxygen level in the blood were measured 15 minutes and 30 minutes after administration
of tablets/capsules.
On the remaining days, the subjects were instructed to take investigational product at home at
the same dose levels in the evening on empty stomach. They were told to take Dinner at least
two hours post-administration of Drug.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Along with Oxypowder, drinking of lots pure water was suggested. This was not only healthy
for the body but was necessary to aid the body in eliminating toxins from the bowel at a faster
rate. Oxy-Powder works with stomach acid; if the level of HCl is below normal, it may
hinder the effectiveness of the Oxy-Powder; hence it was suggested to take an organic lemon
wedge squeezed into glassful of purified water with the Oxy-Powder® in the evening.
During the study, prescription medicines were not contraindicated as long as Oxypowder was
taken 6 hours before or 6 hours after the medicine.
Laxatives, anti-diarhoeals and anti-spasmodics were prohibited during the study.
After starting the study medication, patients were initially called every day in the morning to
check their daily weight for 7 days
After doing the oxygen content on Day 0, all the patients were asked to visit on 3rd week and
the 6th week. They were called in the morning in fasting state.
Patients in Group 1 were administered Oxy-Powder® capsules and their oxygen levels were
measured at 15 and 30 minutes post– administration of the dose. In case of Patients in Group
2, their oxygen levels were measured at 15 and 30 minutes after their arrival at the clinical
site without administering Dulcolax, since they were comparative group.
On 3rd and the 6th week of treatment, the patients were inquired about their feeling of well
being as a result of taking treatment and whether they experienced any adverse effects during
the treatment period described to them by the investigators during counselling.
Stool analysis was repeated at the end of 6 weeks period.
During the course of treatment, the patients were instructed to report ADR's immediately to
the investigator at the study centre. This information was also collected during personal
interview the investigators had during their visits to the study centre on 7th day and at the end
of 3rd week and the 6th week.
9.5 ENDPOINT(S):
a) Findings of (i) Stool Examination (ii) Barium Meal and (iii) Colonoscopy
b) Relief of Constipation and IBS resulting in improvement in "Quality of life" of the patient.
10.0 DEMOGRAPHY:
Demographic data including Height, Weight, Age, and Sex was collected for all the subjects
in different groups at the time of their inclusion in the study simultaneous to recording of
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
their Medical History including their Food Habits, Smoking History, Details and Quantity of
consumption of alcoholic drinks and other beverages in a day or frequency thereof and
consumption of Tobacco in other forms or any Drug of Abuse.
As regards the symptom of constipation, duration of its existence, its severity, No. of Bowels
/ Week and type of stools were also recorded.
GRADING OF RESPONSE
The evaluated parameters were compared with those obtained with Dulcolax administered to
the patients belonging to the constipation group.
11.0 EFFICACY:
a) Overall therapeutic response was graded individually by the investigator with each patient
as ‘Excellent', ‘Good', ‘Fair' & ‘Poor'.
b) Therapeutic efficacy was correlated and graded as ‘Complete Cure', ‘Improvement' and
12.0 SAFETY:
Severity of each Adverse Event was rated as ‘Mild' (no limitation of usual activity),
‘Moderate' (some limitation of usual activity), and ‘Severe' (inability to carry out usual
13.0 WITHDRAWAL FROM STUDY:
One patient in Oxypowder group had severe diarrhoea on the 2nd day of treatment. He could
not carry out his usual activities and felt dehydrated. He voluntarily withdrew from the study
on 3rd day. Remaining 26 patients continued with the study.
14.0 STATISTICS AND DATA HANDLING:
14.1 STATISTICAL ANALYSIS– DERIVED AND TRANSFORMED DATA:
Out of 40 patients, 39 patients completed the study & were included in the final analysis. The
patients from two centres were pooled for analysis. Their demographic features were
compared at baseline using appropriate tests (Student's T-Test and Chi-square or Fisher's
exact test). Efficacy parameters in two treatment groups were compared by using Fisher's
14.2 DATA ANALYSIS:
14.2.1 Hypotheses
Oxy-Powder® is both, safe and effective in patients with constipation
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
14.2.2 Sample Size Consideration
The study design had been examined and approved by a qualified statistician with respect to
14.2.3 Primary Comparisons of Interest
Oxy-Powder® is compared for effectiveness in relieving constipation vis-à-vis Dulcolax
tablets in the same group.
14.2.4 Other Comparisons of Interest
Comparison of safety of Oxy-Powder® has been done vià safety achieved post-administering
of Dulcolax tablets.
14.2.5 Interim Analysis
Data from patients was collected regularly but analyzed at the end of the study for safety and
effectiveness of the Oxy-Powder®.
14.2.6 Analysis Population
After the dropouts, it was assumed to have a minimum of 30 patients (out of 40) in
constipation group completing the study. Number of patients who actually completed 6
weeks of study was 39. The population analysis for safety and effectiveness of Oxy-Powder®
and Dulcolax has been done for these 39 patients at the end of the study.
14.2.7 Withdrawal
One patient who voluntarily withdrew from the study has not been included in the report
14.2.8 Missing Data
There has been no Missing data of any patient.
15.0 OTHER ISSUES:
Results of Barium Meal test conducted at the commencement of study at pre– dose
administration indicated that none of the patients exhibited any signs of organic lesions.
In 7 patients completing the study, no organic lesions were seen in Barium meal test even 6
weeks post– dose administration at the completion of the study.
In the same 7 patients completing the study (of Oxy-Powder® as well as Dulcolax) , pre–
dose colonoscopy as well as 6 weeks post dose administration colonoscopy studies showed
similar findings in patients under study in having multiple spasmodic contractions in sigmoid
and descending colon but with slight reduction in impacted faecal material shown in
post– administration colonoscopy. This is perhaps one of the factors responsible for
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
efficacy of Oxy-Powder® in the treatment of constipation with and without IBS. Six weeks
period of study was perhaps short to see greater reduction in impacted faecal material
The investigators recommended that since conduct of these two tests after 6 weeks of
completion of the study did not show any significant differences that could lead to any
conclusions, they should be dropped at the conclusion of the study. However, the patients
should continue to be subjected to these two tests at the commencement of study.
These recommendations were forwarded to the sponsor by e-mail who gave his consent to
follow the recommendations of the investigator and permitted waiving of conduct of these
two tests at the end of 6 weeks period of the study in each of the rest of the patients.
16.0 ETHICS:
The design of the protocol conformed to the Declaration of Helsinki adopted by the 18th
World Medical Assembly (WMA), Helsinki, Finland (1964) and all amendments. All the
patients were informed of the nature and the purpose of the study and their consent to
participate was obtained. They were also informed of their freedom to withdraw from the
study at anytime and at any stage of the trial.
The study was conducted only after the protocol was approved by IEC of MCERC and IRB
of Bhatia General Hospital.
Since Oxy-Powder® was marketed in the USA and other countries for almost a decade with
no reported ADR's, and the present study was designed and conducted for global markets
(other than India), the study director prudently and by way of abundant precaution informed
Indian Regulatory Authority, Drugs Controller General of India at CDSCO, New Delhi, of
intention of MCERC to conduct the clinical trial Phase loll on Oxy-Powder® in Indian
16.1 ETHICAL CONDUCT OF THE STUDY AND ETHICS APPROVAL
This study was conducted in accordance with "Good Clinical Practice" (GCP) guidelines and
all other applicable regulatory requirements, including WMA's Declaration of Helsinki –VI
on Ethical Principles for Medical Research Involving Human Subjects, as adopted by the
52nd WMA General Assembly, Edinburgh, October 2000.
The investigator was assigned the responsibility for ensuring that this protocol, the site's
informed consent form, and any other information that will be presented to potential subjects
(e.g. advertisements or information that supports or supplements the informed consent) were
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
reviewed and approved by the appropriate IEC/IRB. The investigator agreed to allow the IEC
/ IRB direct access to all relevant documents. MCERC provided the investigator, IEC and
IRB with relevant document(s)/data that were needed for IEC/IRB review and approval of the
protocol for conducting the study. After receiving copies of the IEC/IRB approval, the
investigational product(s), blank copies of the approved informed consent forms, CRF's and
any other information that the IEC/IRB had approved for presentation to potential subjects.
were sent to the trial centre sites, No further amendments were made in the above formats by
17.1 INFORMED CONSENT
Informed consent was obtained from each participant before the subject was permitted to participate
in the study. The contents and process of obtaining informed consent was in accordance with all
applicable regulatory requirements.
18.0 PROTOCOL COMPLIANCE:
There were three deviations in the protocol.
1) Due to non-availability of suitable patients, request was made to sponsor to reduce the number in
constipation group to 40 in place of 60 (as described in the Protocol). This was necessary to avoid
delay in completing the study. The sponsor gave his consent. Consequently, 27 patients were assigned
to Oxy-Powder® group and remaining 13 patients to Dulcolax.
2) Age of the patients for enrollment was raised to 65 years to include geriatric patients in whom
constipation is more prevalent. There was shortage of patients suffering from constipation in the age
group specified in the protocol.
Permission from the sponsor was obtained to include patients suffering from constipation up to the
age of 65 years.
3) During course of the study, both the investigators independently made following observation:
a) Pre- and post-colonoscopy showed multiple spasmodic contractions in sigmoid and descending
colon with large amount of fecal impaction in entire colon.
b) In Barium meal test, no organic lesions were seen before and after Barium meal administration.
These observations were made in case of type1and type 2 patients.
Both the investigators recommended that in view of these observations, post-colonoscopy and post-
administration of Barium meal should not be done since they do not significantly contribute to the
results of the study. Instead, they were causing discomfort discouraging the patients from continuing
with the treatment. They recommended that both the tests must be done at the time of enrolling the
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
These recommendations were forwarded to the sponsor who, while agreeing with the suggestions of
the investigators permitted to waive conduct of post- colonoscopy as well as post administration of
19.0 RESULTS:
(a) DESCRIPTIVE:
(i) Demography:
The baseline demographic characteristics of patients were similar in two treatment groups of the study
(P> .05). Summary of patient's characteristics including sex, age & weight is presented in Table 1
Table 1– Demographic Characteristics.
Drug & No. of
Age ( yrs )
Wt. ( Kg. )
Patients
Mean ( SD)
Mean ( SD )
Male Female
(ii) Patient's living style
The food habits of the patients are given in Table 3. Both Non-Vegetarian and Vegetarian patients
were included in the study.
Table 2 Food Habits.
Drug
Non veg (%)
Veg. (%)
A (Oxypowder) – 27
B (Dulcolax) – 13
In both the groups, some patients were smokers – Table 3.
Table 3 Smoking History
Drug Yes No
A (Oxypowder )– 27
B (Dulcolax) – 13
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
(iii) Medical History:
According to Rome II criteria for constipation, all patients were suffering from constipation for 12
weeks (3 months) or more. They were grouped as follows – Table 4
Table 4– Duration of constipation in months (Group wise)
A (Oxypowder)
B (Dulcolax)
3 months – 12 months
12 months – 24 months
After grouping the patients according to duration of constipation, they were further grouped according
to number of bowels passed in a week (Table 5). This was done to grade the patients in terms of
severity of constipation (Table 6)
Table 5. No. Of Bowels in a Week for OP and DL on day 0 for Classifying Patients before study
commenced
Groups A(Oxypowder)
B
Table 6 Severity of Constipation.
A (Oxypowder)
B (Dulcolax)
All above groups were statistically compared by using appropriate tests & there was no statistically
significant difference between the two groups indicating they were comparable at the base line values
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
(IV) Study Medication:
The randomization of the patients was done as 2:1 i.e. 2 patients were given Oxypowder & 1 patient
was given Dulcolax. Out of 40 patients, 27 patients received Oxypowder (A) & 13 patients received
Dulcolax (B). Their disposition for the study is presented in Table 7.
Table 7 – Randomization
(V) Non–Study Medication:
None of the patients received any medication other than the Test or the Reference formulation.
(VI) Patient Withdrawal:
One patient receiving Test formulation (Oxy-Powder®) withdrew on the second day of treatment as
he had severe diarrhoea. He could not carry out his usual activities and felt dehydrated and hence
withdrew from the study on the 3rd day. He withdrew mainly because of Safety Reasons.
All the patients were checked for their daily weight for 7 days (0 + 6 days) & then on 3rd week & 6th
Table 8 shows comparison of their weights From Day 0 to day 42.
Table 8 – Comparison of weight (kg) (Day 0 – Day 42)
Drug No
Mean (∀ S.D.)
A(OP) Day 0
65.19 ( 12.670% )
64.96 ( 12.820% )
64.89 ( 12.845% )
65.10 ( 13.081% )
65.13 ( 13.016% )
65.00 ( 13.159% )
65.02 ( 13.196% )
65.23 ( 13.240% )
65.33 ( 13.217% )
B (DL) Day 0
64. 00 ( 11.255% )
63.65 ( 11.557% )
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Drug No
Mean (∀ S.D.)
63.42 ( 11.310 % )
63.50 ( 11.673% )
63.31 ( 11.494% )
63.19 ( 11.640% )
63.23 ( 11.499% )
63.23 ( 11.263% )
63.81 ( 11.426% )
One patient from Oxypowder (A) groups was dropped from the study on 3rd day & hence not included
in the final assessment.
As seen from the table, there is no reduction in the weight of the patients after 42 days as compared to
base line (0 day) indicating administration of Oxypowder did not lead to reduction of weight in the
Similarly there was no reduction in the weight in Dulcolax group.
In both groups, after starting administration of the study drug; frequency of stools
(Number of Bowels in a week) increased as shown in Table 9.
Table 9 – Number of Bowels in a week (grouped)
Day 0
Day 21
Day 42
11 (40.7% ) 8 ( 61.5%)
12 (44.4% ) 4 ( 30.8% ) 10 ( 30.5% ) 7 (53.8% ) 6 (23.1% ) 2 ( 15.4% )
Note: OP = Oxy-Powder®, DL= Dulcolax
As seen from Table 9 in Oxypowder group, 11 patients had frequency of stools as 1-4 / week on Day
0. After starting Oxypowder, frequency increased and on Day 42, 19(73.1%) patients had frequency
Increase in the frequency of stools observed in A Group was more than in B Group.
Oxypowder releases nascent oxygen for its action and the objective of the study was to seen whether
Oxypowder increases oxygen saturation of blood. As seen from Table 10, there was marginal increase
in oxygen delivery after taking Oxypowder for 6 weeks (42 days) as compared to Day 0.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table 10 – Oxygen content of blood (Day 0, Day 21, and Day 42)
Drug No
Mean (∀S.D)
Drug A (OP) Oxygen Content of Blood Day 0
Oxygen Content of Blood Day 21 after 15 Min.
Oxygen Content of Blood Day 21 after 30 Min.
Oxygen Content of Blood Day 42 after 15 Min.
Oxygen Content of Blood Day 21 after 30 Min.
Drug B (DL) Oxygen Content of Blood Day 0
Oxygen Content of Blood Day 21 after 15 Min.
Oxygen Content of Blood Day 21 after 30 Min.
Oxygen Content of Blood Day 21 after 15 Min.
Oxygen Content of Blood Day 21 after 15 Min.
During the study, the patients in both groups showed significant reduction in various symptoms as
shown in Tables 11, 12, 13, 14, 15 ( P < .05 )
Table 11 (a) Straining During >25% of Bowel Movement (Day 0)
Drug
No. of patients (%)
B (DL)
Table 11(b) Straining During > 25% of Bowel Movement (Day 21).
Drug
No. of patients (%)
A (OP)
B (DL)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table 11(c) Straining During > 25% of Bowel Movement (Day42).
Drug
No. of patients (%)
A (OP)
B (DL)
Table12 (a) Lumpy Stools (Day 0).
Drug
No. of patients (%)
A (OP)
B (DL)
Table 12 (b) Lumpy Stools (Day 21).
Drug
No. of patients (%)
A (OP)
B (DL)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table 12(c) Lumpy Stools (Day 42).
Drug
No. of patients (%)
A (OP)
B (DL)
Table 13(a) Sensation of incomplete evacuation for >25% of Bowel movement (Day 0)
Drug
No. of patients (%)
A (OP)
B (DL)
Table 13(b) Sensation of incomplete evacuation for >25% of Bowel movement (Day21).
Drug
No. of patients (%)
A (OP)
B (DL)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table 13(c) Sensation of incomplete evacuation for >25% of Bowel movement Day 42.
Drug
No. of patients (%)
A (OP)
B (DL)
Table 14(a) Sensation of Anorectal Blockage for >25% of Bowel Movement (Day 0).
Drug
No. of patients(%)
A (OP)
B (DL)
Table 14(b) Sensation of Anorectal Blockage for >25% of Bowel Movement (Day 21).
Drug
No. of patients (%)
A (OP)
B (DL)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table 14(c) Sensation of Anorectal Blockage for >25% of Bowel Movement (Day 42).
Drug
No. of patients(%)
B (DL)
Table 15 (a) Manual Manoeuvres to facilitate >25% of Bowel Movements (Day 0).
Drug
No. of patients(%)
A (OP)
B (DL)
Table 15(b) Manual Manoeuvres to facilitate >25% of Bowel Movements (Day 21).
Drug
No. of patients(%)
B (DL)
Table 15(c) Manual Manoeuvres to facilitate >25% of Bowel Movements (Day 42).
Drug
No. of patients (%)
A (OP
B (DL)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Drug
No. of patients (%)
As seen from Table 11, in group A, 25 patients (92.6 %) had straining on Day 0 as compared to this
on Day 42 only 2 (7.7%) patients had this symptom.
Similarly, in Table 12, in group A, 26 patients (96.3%) passed hard and lumpy stools on Day 0 where
as on day 42 it was reported only in two patients (7.7%). Above parameters indicate that there was
significant reduction in the symptoms (P<05) in both groups.
Routine stool examination done before and after the drug treatment showed no abnormality in all 40
patients in this study.
Overall Efficacy:
Overall Efficacy was independently judged by the Investigators & the patients. It was graded as
excellent, Good, Fair and Poor. The results were statistically analysed using Fisher's Exact Test.
Table 16–Overall Efficacy
(A) ASSESSMENT BY INVESTIGATORS
ASSESSMENT– InvestigatorS
DRUG
A (OP)
B (DL)
(P < 0.05)
INVESTIGATORS INVESTIGATORS
INVESTIGATORS
INVESTIGATORS
(P<0.05)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
(B) ASSESSMENT BY PATIENTS * DRUG CODE Cross tabulation
DRUG
ASSESSMENT– PATIENTS
A (OP)
B (DL)
(P < 0.05)
In group a out of 26 completed patients investigator assessment was excellent for 13 ( 50% ) Good for
12(46.2% ) Fair for 1 ( 3.8% ), where as in group B out of 13 patients it was excellent for 1 (7.7% )
Good for 6 ( 46.2% ), Fair for 4 ( 30.8% ) and poor for 2 ( 15.4% ).
Efficacy of Oxypowder in treating constipation was significantly (P<.05) more than Dulcolax and
hence this indicates Oxypowder was more efficacious in treating constipation than Dulcolax.
Overall efficacy was also judged as complete cure, Improvement and Failure. Table 17 shows that in
group A, out of 26 patients 11 patients ( 42.3% ) had complete cure, ( 57.7% ) had improvement and
there was no failure where as in group B, out of 13 patients,1 patient (7.7%) had complete cure, 10
patients (76.9% ) had improvement and 2 patients ( 15.9% ) had failure.
Table 17 –
Comparison of Efficacy of Oxy-Powder® with Dulcolax
Efficacy
A (OP)
B (DL)
(P< 0.05)
Results in above Table indicate that efficacy of Oxypowder is significantly more (P < .05) than
Dulcolax in treating patients of constipation.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
(c) SAFETY:
Adverse events
Regarding Adverse events, 1 patient in Oxypowder group had severe diarrhoea on the 2nd day of
treatment. He could not carry out his usual activities and felt dehydrated and hence withdrew from the
study on 3rd day. In the remaining 26 patients, 2 patients had abdominal fullness after taking
Oxypowder for 2-3 days and then they were symptom– free. Remaining 24 patients had no ADR.
In Dulcolax group, 1 patient had mild abdominal pain which disappeared without medication;
remaining 12 patients did not have any ADR.
DISCUSSION AND SUMMARY
SUMMARY:
The present study titled
"Multicentric Randomized, Open, Comparative study to evaluate the safety and efficacy of Oxy-
Powder® in patients of chronic constipation and IBS"was conducted to evaluate effectiveness of
Oxypowder in treating constipation and IBS with constipation precipitating loss of weight &
improving oxygen delivery in patients of constipation and IBS with constipation The study was
sponsored by Dr. Edward Group III, CEO, Global Healing Center, Inc. & contracted to Mayfair
Clinical, Education & Research Centre (MCERC), a Clinical Research Organisation (CRO) for
conduct of the study.
For evaluating effectiveness of Oxy-Powder® in patients of constipation, the study was conducted in
Bhatia General Hospital and Sharad Shah's Clinic, both located in Mumbai. However, for evaluating
effectiveness of Oxy-Powder® in patients of IBS with constipation, the study was conducted in
Bhatia General Hospital. The Study Protocol was carefully designed and got approved from the
sponsor by MCERC. The respective investigators were Dr. Chetan Bhatt and Dr. Sharad Shah.
The study commenced after MCERC obtained approvals from IEC of MCERC, IRB of Bhatia
Hospital and other Regulatory authorities. The study proposed to enrol 60 patients according to
inclusion and exclusion criteria given in the protocol but ultimately culminated with 40 patients (one
patient out of these had ADR and withdrew from the study from 3rd day). The randomisation of the
patients was done as 2:1 i.e. 2 patients were given Oxypowder & 1 patient was given Dulcolax, the
comparative product. Thus, there were 27 patients in Oxy-Powder® group and 13 patients in Dulcolax
group. All the patients were counselled before enrolment and their "Informed Consent" was taken.
Their Medical History was recorded by the investigators They were subjected to clinical examination
and pre-study evaluation including recording of weight, oxygen content of blood using pulse
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
oxcimeter, stool examination, Barium meal (to rule out any Bowel organic lesion leading to
constipation) and colonoscopy (to rule out any colonic organic lesion and any faecal impaction).
Duration of the trial was 42 days i.e. 6 weeks out of which the first week administration of the
treatment products was for bowel cleansing followed by 5 weeks of maintenance. The patients were
instructed to take four capsules of Oxy-Powder® (Test formulation) or two tablets of Dulcolax
(Comparative formulation), as per the Randomization scheme, with plenty of water every day for first
7 days, in the evening on empty stomach. Thereafter, subjects were instructed to take the same dose of
either test of reference formulation on alternate days, on empty stomach, in the evening, for period of
Administration on day '0', '3 weeks' and '6 weeks' were done on empty stomach in the morning.
Subjects were asked to report to the hospital with empty stomach in the morning for administration of
investigational products and Oxygen level in the blood were measured 15 minutes and 30 minutes
after administration of tablets/capsules.
On the remaining days, the subjects were instructed to take investigational product at home at the
same dose levels in the evening on empty stomach. They were told to take Dinner at least two hours
post-administration of Drug. Patients were emphatically told to report to the investigators any
ADR's that they experience during or after the study.
DISCUSSION OF THE RESULTS:
The Demographic Characteristics recorded in Table-1 indicate that among 27 patients enrolled in
Oxy-Powder® (OP) group, there were 19 male patients (70.4%) and 8 female patients (29.6%) while
in 13 patients in Dulcolax group (DL), there were 8 male patients (61.5%) and 5 female patients
(38.5%).They conformed to the age and the weight as given in the protocol. 13(48.1%) in OP group
were non-vegetarians and 14 (51.9%) were vegetarians as compared to 7(53.8%) non-vegetarians and
6(46.2%) vegetarians in DL group. Majority of patients in both the groups were non-smokers.
MEDICAL HISTORY: Their medical history indicated that in OP group, among the patients
enrolled,13 (48.1%) patients suffered from constipation problem for a period ranging between 3
months to 12 months, 6 (22.2%) between 12 months to 24 months and 8 (29.6%) for more than 24
months. In DL group, 6 (46.2%) patients suffered from constipation problem for a period ranging
between 3 months to 12 months, 4 ( 30.8% ) between 12 months to 24 months and 3 ( 23.1% ) for
more than 24 months.
These and the above figures indicate that enrolment was in full conformance with the
requirements of the protocol.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
As regards the severity of constipation based on number of bowels in a week, in OP group, 9(33.3%)
patients suffered from Severe constipation, 17(63.0%) from Moderate constipation and 1(3.7%)
from Mild constipation,
In DL group, 5(38.5%) patients suffered from Severe constipation, 8(61.5%) from Moderate
constipation and none from Mild constipation,
IN OTHER WORDS, THE TWO GROUPS OF PATIENTS ENROLLED WERE EVENLY
BALANCED WITH RESPECT TO SEVERITY OF CONSTIPATION.
POST ADMINISTRATION CHANGES:
As seen from the results recorded in Table 8, there is no reduction in the weight of the patients in OP
group after 42 days of administration of Oxy-Powder® as compared to Base line (0 day) indicating
that administration of Oxypowder did not lead to reduction of weight in the patients. Similarly, there
was no reduction in the weight in Dulcolax group. In both the groups, after starting the investigating
drug; frequency of stools (No. of Bowels in a week) increased as is shown by the results recorded in
Table 9. Comparing the two groups, the percentage performance of Oxy-Powder® was better than
Dulcolax on the 21st and the 42nd Day.
As stated in the "Introduction", Oxypowder releases nascent oxygen for its action; the objective of
this study was to see whether Oxypowder increases oxygen saturation of blood. As seen from Table
10, there was marginal increase in oxygen delivery after taking Oxypowder for 6 weeks (42 days) as
compared to Day 0. It thus appears that the study period was little short and should have been
extended approximately to 180 days to get more conclusive results.
During the study, the patients in both the groups showed significant reduction in various symptoms as
shown in Tables 11, 12, 13, 14, 15 (Straining During >25% of Bowel Movement during 0-42 days,
Lumpy Stools during 0-42 days, Sensation of incomplete evacuation for >25% of Bowel movement
during 0-42 days, Sensation of Anorectal Blockage for >25% of Bowel Movement during 0-42 days
and Manual Manoeuvres to facilitate >25% of Bowel Movements during 0-42 days). As can be seen
from the results in Table 11 in Oxypowder group, 25 patients (92.6%) had straining on Day 0 as
compared to only 2 (7.7%) patients on Day 42. Similarly, in Table 12, in the same group, 26 patients
96.3%) passed hard and lumpy stools on Day 0 where as on day 42, it was reduced only to two
patients (7.7%). The above parameters indicate that there is significant reduction in the symptoms
(P<05) in both groups. However, In this case also, the results were better in case of Oxypowder as
compared to Dulcolax Routine stool examination done before and after the drug treatment showed no
abnormality in all 40 patients in this study
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
EFFICACY JUDGED:
Efficacy was independently judged by the Investigators & the patients. It was graded as excellent,
Good, Fair and Poor. The results were statistically analysed using Fisher's Exact Test. In Oxypowder
group, out of 26 completed patients, investigator assessment was excellent for 13 (50%) Good for
12(46.2%) Fair for 1 (3.8%), where as in Dulcolax group, out of 13 patients, it was excellent for 1
(7.7%) Good for 6 (46.2%), Fair for 4 (30.8%) and poor for 2 (15.4%).
Overall efficacy was also judged as complete cure, Improvement and Failure. Table 17 shows that in
Oxypowder group , out of 26 patients, 11 patients ( 42.3% ) had complete cure, 15 patients ( 57.7% )
had improvement and there was no failure where as in Dulcolax group, out of 13 patients, 1 patient (
7.7% ) had complete cure, 10 patients ( 76.9% ) had improvement and 2 patients ( 15.9% )
experienced failure
CONCLUSION:
Efficacy of Oxypowder in treating constipation was significantly (P<.05) higher than Dulcolax thus
indicating that Oxypowder was more efficacious in treating constipation than Dulcolax.
No adverse event was reported other than one patient in Op group withdrawing from the study.
Oxy-Powder® was well tolerated by all the patients under treatment of this product.
Helsinki's Declaration -1964, World Medical Association
(Subsequently revised Tokyo 1975, Venice 1983, Hong Kong 1991, Edinburgh 2000)
Recommendations guiding physicians in biomedical research involving human subjects
Adopted by the 18th World Medical Assembly Helsinki, Finland, June 1964 and amended by
the 29th World Medical Assembly, Tokyo, Japan, October 1975 35th World Medical
Assembly, Venice, Italy, October 1983 41st World Medical Assembly, Hong Kong,
September 1989 and the 48th General Assembly, Somerset West, Republic of South Africa,
It is the mission of the physician to safeguard the health of the people. His or her knowledge
and conscience are dedicated to the fulfillment of this mission. The Declaration of Geneva of
the World Medical Association binds the physician with the words, "The Health of my
patient will be my first consideration," and the International Code of Medical Ethics declares
that, "A physician shall act only in the patient's interest when providing medical care which
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
might have the effect of weakening the physical and mental condition of the patient."
The purpose of biomedical research involving human subjects must be to improve diagnostic,
therapeutic and prophylactic procedures and the understanding of the etiology and
pathogenesis of disease.
In current medical practice, most diagnostic, therapeutic or prophylactic procedures involve
hazards. This applies especially to biomedical research.
Medical progress is based on research, which ultimately must rest in part on experimentation
involving human subjects. In the field of biomedical research, a fundamental distinction must
be recognized between medical research in which the aim is essentially diagnostic or
therapeutic for a patient, and medical research, the essential object of which is purely
scientific and without implying direct diagnostic or therapeutic value to the person subjected
to the research.
Special caution must be exercised in the conduct of research, which may affect the
environment, and the welfare of animals used for research must be respected.
Because it is essential that the results of laboratory experiments be applied to human beings
to further scientific knowledge and to help suffering humanity, the World Medical
Association has prepared the following recommendations as a guide to every physician in
biomedical research involving human subjects. They should be kept under review in the
future. It must be stressed that the standards as drafted are only a guide to physician all over
the world. Physicians are not relieved from criminal, civil and ethical responsibilities under
the laws of their own countries.
I. BASIC PRINCIPLES:
1. Biomedical research involving human subjects must conform to generally accepted
scientific principles and should be based on adequately performed laboratory and animal
experimentation and on a thorough knowledge of the scientific literature.
2. The design and performance of each experimental procedure involving human subjects
should be clearly formulated in an experimental protocol which should be transmitted for
consideration, comment and guidance to a specially appointed committee independent of the
investigator and the sponsor provided that this independent committee is in conformity with
the laws and regulations of the country in which the research experiment is performed.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
3. Biomedical research involving human subjects should be conducted only by scientifically
qualified persons and under the supervision of a clinically competent medical person. The
responsibility for the human subject must always rest with a medically qualified person and
never rest on the subject of the research, even though the subject has given his or her consent.
4. Biomedical research involving human subjects cannot legitimately be carried out unless
the importance of the objective is in proportion to the inherent risk to the subject.
5. Every biomedical research project involving human subjects should be preceded by careful
assessment of predictable risks in comparison with foreseeable benefits to the subjects or to
others. Concern for the interests of the subject must always prevail over the interests of
science and society.
6. The rights of the research subject to safeguard his or her integrity must always be
respected. Every precaution should be taken to respect the privacy of the subject and to
minimize the impact of the study on the subject's physical and mental integrity and on the
personality of the subject.
7. Physicians should abstain from engaging in research projects involving human subjects
unless they are satisfied that hazards involved are believed to be predictable. Physicians
should cease any investigation if the hazards are found to outweigh the potential benefits.
8. In publication of the results of his or her research, the physician is obliged to preserve the
accuracy of the results. Reports of experimentation not in accordance with the principles laid
down in this Declaration should not be accepted for publication.
9. In any research on human beings, each potential subject must be adequately informed of
the aims, methods, anticipated benefits and potential hazards of the study and the discomfort
it may entail. He or she should be informed that he or she is at liberty to abstain from
participation in the study and that he or she is free to withdraw his or her consent to
participation at
any time. The physician should then obtain the subject's freely given informed consent,
preferably in writing.
10. When obtaining informed consent for the research project the physician should be
particularly cautious if the subject is in a dependent relationship to him or her or may consent
under duress. In that case, the informed consent should be obtained by a physician who is not
engaged in the investigation and who is completely independent of this official relationship.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
11. In case of legal incompetence, informed consent should be obtained from the legal
guardian in accordance with the national legislation. Where physical or mental incapacity
makes it impossible to obtain informed consent, or when the subject is a minor, permission
from the responsible relative replaces that of the subject in accordance with national
Whenever the minor child is in fact able to give consent, the minor's consent must be
obtained in addition to the consent of the minor's legal guardian.
12. The research protocol should always contain a statement of the ethical considerations
involved and should indicate that the principles enunciated in the present Declaration are
II. MEDICAL RESEARCH COMBINED WITH PROFESSIONAL CARE (Clinical
Research)
1. In the treatment of the sick person, the physician must be free to use a new diagnostic and
therapeutic measure, if in his or her judgment it offers hope of saving life, reestablishing
health or alleviating suffering.
2. The potential benefits, hazards and discomfort of a new method should be weighed against
the advantages of the best current diagnostic and therapeutics methods.
3. In any medical study, every patient - including those of a control group, if any - should be
assured of the best-proven diagnostic and therapeutic method. This does not exclude the use
of inert placebo in studies where no proven diagnostic or therapeutic method exists.
4. The refusal of the patient to participate in a study must never interfere with the physician-
patient relationship.
5. If the physician considers it essential not to obtain informed consent, the specific reasons
for this proposal should be stated in the experimental protocol for transmission to the
independent committee (I, 2).
6. The physician can combine medical research with professional care, the objective being
the acquisition of new medical knowledge, only to extent that medical research is justified by
its potential diagnostic value for the patient.
II. NON-THERAPEUTIC BIOMEDICAL RESEARCH INVOLVING
HUMAN SUBJECTS
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
(Non-Clinical Biomedical Research)
1. In the purely scientific application of medical research carried out on a human being, it is
the duty of the physician to remain the protector of the life and health of that person on whom
biomedical research is being carried out.
2. The subject should be a volunteer - either healthy persons or patients for whom the
experimental design is not related to the patient's illness.
3. The investigator or the investigating team should discontinue the research if in his/her or
their judgment it may, if continued, be harmful to the individual.
4. In research on man, the interest of science and society should never take precedence over
considerations related to the wellbeing of the subject.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506

MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
IEC– MCERC APPENDIX– 2
IRB of Bhatia Hospital APPENDIX– 3
APPENDIX– 4
VERSION – 02
PROTOCOL FOR
CLINICAL TRIAL PHASE III
SAFETY AND EFFICACY OF OXY-POWDER®
DOCUMENT NO.: MCERC/PROT-CLTR/OXY/1205/001
December 20, 2005
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
(A KALTHIA GROUP ORGANIZATION)
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Ph. No. 91-022-2589 5856 Fax. 91-022-2589 5854
e-mail [email protected]
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Division:
Clinical Research
Document Number:
CLTR/OXY/1205/001
Document Type: Protocol
Study Identifier:
Mfair/oxy/2005-06
Site of Issue:
Thane, Maharashtra
Document Date:
Title: Efficacy & Safety of Oxy-Powder®
The effectiveness of the Oxy-Powder® in treating constipation and IBS.
Abstract:
Constipation is the slow movement of feces (stool or body wastes) through the large intestine
resulting in infrequent bowel movements and the passage of dry, hard stools. The longer it takes for
the stool to move through the large intestine, the more fluid is absorbed and the drier and harder the
stool becomes. Constipation is annoying and uncomfortable, but fecal impaction (a collection of dry,
hard stool in the colon or rectum) can be life threatening. Patients with a fecal impaction may not have
gastrointestinal symptoms. Instead, they may have circulation, heart, or breathing problems. If fecal
impaction is not recognized, the signs and symptoms will get worse and the patient could die.
Irritable bowel syndrome (IBS), a functional gastrointestinal disorder characterized by the interplay of
altered motility, abnormal visceral sensation, and psychosocial factors, is one of the most common
reasons for referral to a gastroenterologist. It is associated with bouts of constipation and diarrhoea.
‘Oxy-Powder®' used universally as a dietary supplement for relieving constipation is being taken up
for the study under Clinical Trials Phase III in 60 constipation and 20 IBS patients in Open,
Randomized, Comparative study in 3 Centres. The Study protocol includes exclusion and inclusion
criteria, mode of administration of test and reference products, evaluation of effectiveness and safety
and data analysis and management. The GCP guidelines shall be followed for the conduct of the
studies. Reporting of AEs and SAR has been emphasized. The duration of the study, post
administration is 6 weeks.
Authors: Prof. J K Lalla, Ph.D., Dr Meena Shah, M.D., Dr Deven Parmar, M.D.
Compound Numbers/Keywords (if applicable): Oxy-Powder®
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
1. Dr. Edward Group-Sponsor from US
2. Dr. Mahesh Patel-Consultant from US
3. Prof. J. K. Lalla, Ph.D. – Study Director
4. Dr. Sharad Shah – Gastroenterologist – Jaslok Hospital
5. Dr. Chetan Bhatt – Clinical Investigator – Bhatia Hospital
6. Dr. Philip Ibrahim – Clinical Investigator – Hinduja Hospital
7. Chairpersons – Hospital Ethics Committee
8. Dr. Meena Shah – Mayfair Clinical, Education and Research Centre
9. Dr. Deven Parmar – Mayfair Clinical, Education and Research Centre
10. CRA's of Mayfair Clinical, Education and Research Centre
Objective:
To study the safety and efficacy of Oxy-Powder® in patients of chronic constipation and IBS.
Randomized, open, comparative study.
Document Number: MCERC/PRTO-CLTR/OXY/1205/001
Study Identifier: Mfair/oxy/2005-06
Approval Date: dd Mmm yyyy
Author(s): Prof. J K Lalla, Ph.D., Dr Meena Shah, M.D., Dr Deven Parmar, M.D.
Sponsor Signatory:
Signature:
Dr. Edward Group III
CEO, Global Healing Center,
Copyright 2XXX the Mayfair. All rights reserved.
Unauthorized copying or use of this information is prohibited.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
SPONSOR INFORMATION PAGE:
Title: Randomized, open, comparative study To study the
safety and efficacy of Oxy-Powder® in patients of chronic
constipation and IBS.
Document Number: MCERC/PRTO-CLTR/OXY/1205/001
Study Identifier: Mfair/oxy/2005-06
Mfair/oxy/2005-06
Investigator Protocol Agreement Page:
• To assume responsibility for the proper conduct of the study at this site. • To conduct the study in compliance with this protocol, any future amendments, and with any
other study conduct procedures provided by Mayfair. Not to implement any changes to the protocol
without agreement from the sponsor and prior review and written approval from the Institutional
Review Board (IRB) or Independent Ethics Committee (IEC), except where necessary to eliminate an
immediate hazard to the subjects, or for administrative aspects of the study (where permitted by all
applicable regulatory requirements).
• That I am thoroughly familiar with the appropriate use of the investigational product(s), as
described in this protocol, and any other information provided by the sponsor including, but not
limited to, the following: the current Clinical Investigator's Brochure / Investigator's Brochure
(CIB/IB) or equivalent document, CIB/IB supplement (if applicable), and approved product label (if
the product is marketed in this country and the label is not already provided as an equivalent to a
• That I am aware of, and will comply with, "good clinical practices" (GCP) and all applicable
regulatory requirements.
• To ensure that all persons assisting me with the study are adequately informed about the
investigational product(s) and of their study-related duties and functions as described in the protocol.
• That I have been informed that certain regulatory authorities require the Sponsor to obtain and
supply, as necessary, details about the investigator's ownership interest in the Sponsor or the
investigational product, and more generally about his/her financial ties with the Sponsor. Mayfair will
use and disclose the information solely for the purpose of complying with regulatory requirements.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
• Agree to supply MAYFAIR with any necessary information regarding ownership interest and
financial ties (including those of my spouse and dependent children);
• Agree to promptly update this information if any relevant changes occur during the course of the
study and for 1 year following completion of the study; and
• Agree that MAYFAIR may disclose any information it has about such ownership interests and
financial ties to regulatory authorities.
Investigator Name: _
Investigator Signature
The following co-signature is required only when the investigator is not a [insert the appropriate
wording such as "physician" or "dentist"]
Physician Name: _
Physician Signature
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
TABLE OF CONTENTS
1.0 PROTOCOL SUMMARY
3.0. OBJECTIVE(S)
4.0 STUDY DESIGN
5.0 STUDY POPULATION
6.0 NUMBER OF SUBJECTS
7.0 ELIGIBILITY CRITERIA
8.0 STUDY ASSESSMENTS AND PROCEDURES
9.0 GENERAL LITERATURE DATA
10.0 STUDY DESIGN
11.0 EVALUATIONS
12.0 TREATMENT OF INVESTIGATIONAL PRODUCT
14.0 HANDLING AND STORGE OF INVESTIGATIONAL PRODUCT
15.0 SUBJECT COMPLETION AND WITHDRAWAL
16.0 ADVERSE EVENTS (AE) AND SERIOUS ADVERSE EVCENTS (SAE)
17.0 PROMPT REPORTING OF SAEs TO MAYFAIR
18.0 DATA ANALYSIS AND STATISTICAL CONSIDERATIONS
19.0 REGULATORY AND ETHICAL CONSIDERATIONS
20.0 INVESTIGATOR REPORTING REQUIREMENTS
21.0 STUDY MONITORING
22.0 QUALITY ASSSURANCE
23.0 STUDY AND SITE CLOSURE
24.0 RECORDS RETENTION
25.0 PROVISION OF STUDY RESULTS AND INFORMATION TO MAYFAIR
26.0 INFORMATION DISCLOSURE AND INVENTIONS
27.0 DATA MANAGEMENT
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
GLOSSARY
ADVERSE EVENT: An unwanted effect caused by the administration of drugs. Onset may be
sudden or develop over time
BASELINE: 1. Information gathered at the beginning of a study from which variations found in the
study are measured. 2. A known value or quantity with which an unknown is compared when
measured or assessed. 3. The initial time point in a clinical trial, just before a participant starts to
receive the experimental treatment which is being tested. At this reference point, measurable values
such as CD4 count are recorded. Safety and efficacy of a drug are often determined by monitoring
changes from the baseline values.
BIAS: When a point of view prevents impartial judgment on issues relating to the subject of that point
of view. In clinical studies, bias is controlled by blinding and randomization.
BLIND: A randomized trial is "Blind" if the participant is not told which arm of the trial he is on. A
clinical trial is "Blind" if participants are unaware on whether they are in the experimental or control
arm of the study; also called masked.
CLINICAL: Pertaining to or founded on observation and treatment of participants, as distinguished
from theoretical or basic science.
CLINICAL INVESTIGATOR: A medical researcher in charge of carrying out a clinical trial's
COMPLEMENTARY AND ALTERNATIVE THERAPY: Broad range of healing philosophies,
approaches, and therapies that Western (conventional) medicine does not commonly use to promote
well-being or treat health conditions. Examples include acupuncture, herbs, etc.
CONFIDENTIALITY REGARDING TRIAL PARTICIPANTS: Refers to maintaining the
confidentiality of trial participants including their personal identity and all personal medical
information. The trial participants' consent to the use of records for data verification purposes should
be obtained prior to the trial and assurance must be given that confidentiality will be maintained.
CONTRAINDICATION: A specific circumstance when the use of certain treatments could be
CONTROL: A control is the nature of the intervention control.
CONTROL GROUP: The standard by which experimental observations are evaluated. In many
clinical trials, one group of patients will be given an experimental drug or treatment, while the control
group is given either a standard treatment for the illness or a placebo
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
CONTROLLED TRIALS: Control is a standard against which experimental observations may be
evaluated. In clinical trials, one group of participants is given an experimental drug, while another
group (i.e., the control group) is given either a standard treatment for the disease or a placebo.
DOUBLE-BLIND STUDY: A clinical trial design in which neither the participating individuals nor
the study staff knows which participants are receiving the experimental drug and which are receiving
a placebo (or another therapy). Double-blind trials are thought to produce objective results, since the
expectations of the doctor and the participant about the experimental drug do not affect the outcome;
also called double-masked study.
EFFICACY: (Of a drug or treatment). The maximum ability of a drug or treatment to produce a
result regardless of dosage. A drug passes efficacy trials if it is effective at the dose tested and against
the illness for which it is prescribed. In the procedure mandated by the FDA, Phase II clinical trials
gauge efficacy, and Phase III trials confirm it
ELIGIBILITY CRITERIA: Summary criteria for participant selection; includes Inclusion and
Exclusion criteria.
ENDPOINT: Overall outcome that the protocol is designed to evaluate. Common endpoints are
severe toxicity, disease progression, or death.
FOOD AND DRUG ADMINISTRATION (FDA): The U.S. Department of Health and Human
Services agency responsible for ensuring the safety and effectiveness of all drugs, biologics, vaccines,
and medical devices, including those used in the diagnosis, treatment, and prevention of HIV
infection, AIDS, and AIDS-related opportunistic infections. The FDA also works with the blood
banking industry to safeguard the nation's blood supply.
HYPOTHESIS: A supposition or assumption advanced as a basis for reasoning or argument, or as a
guide to experimental investigation.
INCLUSION/EXCLUSION CRITERIA: The medical or social standards determining whether a
person may or may not be allowed to enter a clinical trial. These criteria are based on such factors as
age, gender, the type and stage of a disease, previous treatment history, and other medical conditions.
It is important to note that inclusion and exclusion criteria are not used to reject people personally, but
rather to identify appropriate participants and keep them safe.
INFORMED CONSENT: The process of learning the key facts about a clinical trial before deciding
whether or not to participate. It is also a continuing process throughout the study to provide
information for participants. To help someone decide whether or not to participate, the doctors and
nurses involved in the trial explain the details of the study.
INFORMED CONSENT DOCUMENT: A document that describes the rights of the study
participants, and includes details about the study, such as its purpose, duration, required procedures,
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
and key contacts. Risks and potential benefits are explained in the informed consent document. The
participant then decides whether or not to sign the document. Informed consent is not a contract, and
the participant may withdraw from the trial at any time.
INSTITUTIONAL REVIEW BOARD (IRB): 1. A committee of physicians, statisticians,
researchers, community advocates, and others that ensures that a clinical trial is ethical and that the
rights of study participants are protected. All clinical trials in the U.S. must be approved by an IRB
before they begin. 2. Every institution that conducts or supports biomedical or behavioral research
involving human participants must, by federal regulation, have an IRB that initially approves and
periodically reviews the research in order to protect the rights of human participants.
INTENT TO TREAT: Analysis of clinical trial results that includes all data from participants in the
groups to which they were randomized even if they never received the treatment.
IRRITABLE BOWEL SYNDROME: Irritable bowel syndrome (IBS), a functional gastrointestinal
disorder characterized by the interplay of altered motility, abnormal visceral sensation, and
psychosocial factors, is one of the most common reasons for referral to a gastroenterologist.
OPEN-LABEL TRIAL: A clinical trial in which doctors and participants know which drug or
vaccine is being administered.
PHASE II TRIALS: Controlled clinical studies conducted to evaluate the effectiveness of the drug
for a particular indication or indications in patients with the disease or condition under study and to
determine the common short-term side effects and risks.
PHASE III TRIALS: Expanded controlled and uncontrolled trials after preliminary evidence
suggesting effectiveness of the drug has been obtained, and are intended to gather additional
information to evaluate the overall benefit-risk relationship of the drug and provide and adequate
basis for physician labelling.
PLACEBO: A placebo is an inactive pill, liquid, or powder that has no treatment value. In clinical
trials, experimental treatments are often compared with placebos to assess the treatment's
PLACEBO CONTROLLED STUDY: A method of investigation of drugs in which an inactive
substance (the placebo) is given to one group of participants, while the drug being tested is given to
another group. The results obtained in the two groups are then compared to see if the investigational
treatment is more effective in treating the condition.
PHARMACOVIGILANCE: Despite all the tests and precautions taken during the development and
authorisation of a pharmaceutical product, medicines still sometimes produce side effects under
certain conditions. Monitoring use and effects of a given medication to detect and prevent these
adverse drug reactions (ADR) is the domain of Pharmacovigilance.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
It is regarded as all post-authorisation scientific and data gathering activities relating to the detection,
assessment, understanding and prevention of adverse events or any other product related problems.
PROTOCOL: A study plan on which all clinical trials are based. The plan is carefully designed to
safeguard the health of the participants as well as answer specific research questions. A protocol
describes what types of people may participate in the trial; the schedule of tests, procedures,
medications, and dosages; and the length of the study. While in a clinical trial, participants following
a protocol are seen regularly by the research staff to monitor their health and to determine the safety
and effectiveness of their treatment.
RANDOMIZATION: A method based on chance by which study participants are assigned to a
treatment group. Randomization minimizes the differences among groups by equally distributing
people with particular characteristics among all the trial arms. The researchers do not know which
treatment is better. From what is known at the time, any one of the treatments chosen could be of
benefit to the participant
RANDOMIZED TRIAL: A study in which participants are randomly (i.e., by chance) assigned to
one of two or more treatment arms of a clinical trial. Occasionally placebos are utilized.
RISK-BENEFIT RATIO: The risk to individual participants versus the potential benefits. The
risk/benefit ratio may differ depending on the condition being treated.
SERIOUS ADVERSE EVENT: A Serious adverse event is any untoward medical occurrence that at
any dose a) results in death b) is life threatening c) requires hospitalization or prolongation of existing
hospitalisation.
SIDE EFFECTS: Any undesired actions or effects of a drug or treatment. Negative or adverse effects
may include headache, nausea, hair loss, skin irritation, or other physical problems. Experimental
drugs must be evaluated for both immediate and long-term side effects.
SINGLE-BLIND STUDY: A study in which one party, either the investigator or participant, is
unaware of what medication the participant is taking; also called single-masked study.
STATISTICAL SIGNIFICANCE: The probability that an event or difference occurred by chance
alone. In clinical trials, the level of statistical significance depends on the number of participants
studied and the observations made, as well as the magnitude of differences observed.
STUDY ENDPOINT: A primary or secondary outcome used to judge the effectiveness of a
STUDY TYPE: The primary investigative techniques used in an observational protocol; types are
Purpose, Duration, Selection, and Timing.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
1.0 PROTOCOL SUMMARY
1.1 Rationale of conducting this study:
The effectiveness of the product in treating constipation and IBS in patients
Recording loss of weight
The effectiveness of the product for Oxygen delivery in patients
The effects Oxy-Powder has on the 4 microbes + 2 parasites present in the digestive tract
including normal Probiotic strain and colonies in the digestive tract.
Safety studies involving acute and sub-acute toxicity in rats/ mice (including histo-pathology)
1.2 OBJECTIVE(S):
Primary:The effectiveness and safety of Oxy-Powder® in treating constipation and IBS
Secondary: The in-vitro effect of Oxy-Powder® on the normal Probiotic strain and colonies in the
Safety studies involving acute and sub-acute toxicity in rats/mice (including histopathology)
1.3 ENDPOINT(S):
Primary: In patients
Finding of i) stool examination ii) Barium Meal and iii) Colonoscopy
Relief of constipation and IBS, improvement of Quality of life
Secondary: in-vitro findings of effectiveness of Oxy-Powder® on normal Probiotic and pathogenic
strain of microbes in digestive tract.
Safety studies involving acute and sub-acute toxicity in rats/mice (including histopathology)
1.4 Study Design: Open, Comparative, randomized study
1.5 Study Population:
1. 60 patients (60% females + 40% males, more number of non-vegetarians, less number of
vegetarians) suffering from constipation
2. 20 patients (60% females + 40% males, more number of non-vegetarians, less number of
vegetarians) suffering from IBS.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
1.6 Study Assessments and Procedures:
6 weeks duration study
Start with a current physical examination
Check height and weight daily for 7 days
Oxygen content in the blood (pulse oxcimeter) on day 0, week 3, week 6 in the morning, on
Fasting Patient called to the hospital, capsule administered & O2 level measured at 15 & 30
minutes post administration
Barium meal, colonoscopy with minimal cleaning done to see how fecal infarction is in the
bowel before and after the study (0 & 6 weeks)
INVESTIGATIONAL PRODUCT(S):
1.7.1 Test Product: (A)
Oxy-Powder® marketed by Global Healing Centre, Inc. USA
Category:
Dietary Supplement
Ozonated Magnesium Oxides: A combination of USP grade Magnesium Oxide mixed with a small
amount USP grade Magnesium Peroxide. This combination is then pressurized at subzero
temperatures and Ozone gas is the stabilizing molecule. The final product contains Stabilized
monatomic oxygen, which is released by an acid based catalyst i.e. HCl in the stomach acid.
Per capsule dosage: 685 mg
Organic Germanium 132:
Does not contain the harmful form of Germanium (Germanium Dioxide)
Per capsule dosage: 5.5 mg
Natural Citric acid:
25 mg per capsule
Other Ingredients:
Kosher certified 00 Vegetarian capsules
1.7.2 Reference Product: (B)
Dulcolax tablets manufactured by Cadila Healthcare Ltd., India.
(Each tablet containing 5 mg Bisacodyl)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Category: Drug belonging to GI therapeutic group
2.0 BACKGROUND
Constipation is the slow movement of feces (stool or body wastes) through the large intestine
resulting in infrequent bowel movements and the passage of dry, hard stools. The longer it takes for
the stool to move through the large intestine, the more fluid is absorbed and the drier and harder the
Constipation is annoying and uncomfortable, but fecal impaction (a collection of dry, hard stool in the
colon or rectum) can be life threatening. Patients with a fecal impaction may not have gastrointestinal
symptoms. Instead, they may have circulation, heart, or breathing problems. If fecal impaction is not
recognized, the signs and symptoms will get worse and the patient could die.
Chronic constipation is one of the most frequent gastrointestinal symptoms in the Unites States,
accounting for nearly 2.5-2.7 million physician visits and 39000-90000 hospitalizations per year in the
United States. Constipation may be stratified, with considerable overlap, into issues of stool
consistency vs defecatory behavior.
Irritable bowel syndrome (IBS), a functional gastrointestinal disorder characterized by the interplay of
altered motility, abnormal visceral sensation, and psychosocial factors, is one of the most common
reasons for referral to a gastroenterologist. It is associated with bouts of constipation and diarrhea.
3.0 OBJECTIVE(S)
To study the safety and effectiveness of Oxy-Powder®
4.0 STUDY DESIGN
Open randomized comparative study
5.0 STUDY POPULATION
Any subject who has given informed consent to participate in the clinical study and has met all the
criteria required for inclusion into the clinical study may take part in the research.
Subject participation in the research project is voluntary and refusal to participate will not indicate
withdrawal from the clinical study. Refusal to participate will involve no penalty or loss of benefits to
which the subject would otherwise be entitled.
No additional administration of investigational product beyond the dose detailed in the clinical study
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
6.0 NUMBER OF SUBJECTS:
a) 60 for constipation
7.0 ELIGIBILITY CRITERIA:
• Patients suffering from constipation and IBS • Age - 18 to 60 yrs • Height & Weight conforming to Height/Weight chart of Life Insurance Corporation of India • Sex – Patients belonging to both sexes are eligible • Food habits-both non-vegetarians and vegetarian patients are eligible • More of the non-vegetarian patients will be preferred.
7.1 INCLUSION CRITERIA
A subject will be eligible for inclusion in this study only if all of the following criteria are satisfied:
1. 18 to 60 years of both sexes (60% females + 40% males)
2. Food habits: Vegetarians are eligible but Non-vegetarians preferred
3. Satisfying the Rome II Criteria for Constipation and IBS
Introduction to Rome II criteria:
At the 13th International Congress of Gastroenterology in Rome, Italy in 1988, a group of physicians
defined criteria to more accurately diagnose constipation and IBS. Known as the "Rome Criteria," this
set of guidelines that outlines symptoms and applies parameters such as frequency and duration make
possible a more accurate diagnosis of Constipation and IBS.
The Rome Criteria were not widely accepted when originally presented, but were better received after
their first revision. This second version, created in 1992 and known as Rome II, added a length of
time for symptoms to be present and pain as an indicator. The second revision, known as Rome III, is
currently underway and shall be released in 2006.
Rome II Criteria for constipation:
Two or more of the following for at least 12 wk (not necessarily consecutive) in the preceding 12 mo:
Straining during >25% of bowel movements;
Lumpy or hard stools for >25% of bowel movements;
Sensation of incomplete evacuation for >25% of bowel movements;
Sensation of anorectal blockage for >25% of bowel movements;
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Manual maneuvers (digital evacuation, support of the pelvic floor) to facilitate >25% of
bowel movements;
Less than 3 bowel movements per week;
Loose stools are not present, and there are insufficient criteria for irritable bowel syndrome
Acceptable form of birth control being followed in female patients
Rome II criteria for IBS
The Rome II diagnostic criteria of Irritable Bowel Syndrome always presumes the absence of a
structural or biochemical explanation for the symptoms and is made only by a physician.
Irritable Bowel Syndrome can be diagnosed based on at least 12 weeks (which need not be
consecutive) in the preceding 12 months, of abdominal discomfort or pain that has two out of three of
these features:
1. Relieved with defecation; and/or
2. Onset associated with a change in frequency of stool; and/or
3. Onset associated with a change in form (appearance) of stool.
Symptoms that Cumulatively Support the Diagnosis of IBS:
1. Abnormal stool frequency (may be defined as greater than 3 bowel movements per day and less
than 3 bowel movements per week);
2. Abnormal stool form (lumpy/hard or loose/watery stool);
3. Abnormal stool passage (straining, urgency, or feeling of incomplete evacuation);
4. Passage of mucus;
5. Bloating or feeling of abdominal distension.
Supportive Symptoms of IBS:
1. Fewer than three bowel movements a week
2. More than three bowel movements a day
3. Hard or lumpy stools
4. Loose (mushy) or watery stools
5. Straining during a bowel movement
6. Urgency (having to rush to have a bowel movement)
7. Feeling of incomplete bowel movement
8. Passing mucus (white material) during a bowel movement
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
9. Abdominal fullness, bloating, or swelling
Red Flag symptoms which are NOT typical of IBS:
Pain that often awakens/interferes with sleep
Diarrhea that often awakens/interferes with sleep
Blood in your stool (visible or occult)
Abnormal physical examination
7.2 EXCLUSION CRITERIA FOR CONSTIPATION AND IBS
A subject will not be eligible for inclusion in this study if any of the following conditions are
observed in the patient
Evidence of Malignancy on colonoscopy / having diagnosed organic GI disorder
Pregnant and lactating women
Evidence of lactose intolerance to explain bowel symptoms
History of cardiac arrhythmias or heart disease
History of Glaucoma
History of urine retention
History of schizophrenia
History of substances of abuse/dependency
intellectually unable or unwilling to complete daily GI ratings
Other Eligibility Criteria Considerations
To assess any potential impact on subject eligibility with regard to safety, the investigator must refer
to the following document(s) for detailed information regarding warnings, precautions,
contraindications, adverse events, and other significant data pertaining to the investigational
product(s) being used in this study.
8.0 STUDY ASSESSMENTS AND PROCEDURES
8.1 Demographic and Baseline Assessments
Physical examination, stool examination, pulse oxcimeter, Barium meal and colonoscopy
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
8.2 Safety in Clinical Trials
Action to be taken if pregnancy occurs
During the study, if the female subject becomes pregnant, she will be withdrawn from the study. She
will be considered as ‘drop-out' in the report which shall be documented in the raw data.
INVESTIGATIONAL PRODUCT - OXY-POWDER®
9.0 GENERAL LITERATURE DATA
9.1 INTRODUCTION:
Oxy-Powder is a specifically designed compound which has been ozonated and stabilized to release
beneficial free monatomic oxygen into the intestinal tract and body. The time-release delivery ensures
that Oxy-Powder will provide an adequate amount of oxygen, slowly, for better utilization by the
body. Oxy-Powder is a non-toxic, safe, effective and non-allergic. By using Oxy-Powder, the
compaction from the small intestine, large intestine and colon is oxidized safely and effectively.
Organic Germanium-132 has demonstrated in multiple scientific studies to be a powerful oxygen
facilitator and immune system stimulant. Oxy-Powder is also harmless to the good bacteria in the
intestinal tract. Natural citric acid has been added to facilitate oxygen release.
Oxygen Enhancement and Intestinal Cleansing Formula
There is only one true way to clean the digestive tract. This is through an oxidation/reduction reaction
or a clean raw food diet. As we age, we accumulate toxic substances in our digestive tract. The
pancreas, the organ which produces the necessary enzymes to break down the food we eat, is limited.
At birth, our pancreas has a limited supply of enzymes. Some doctors say we only have enough
enzymes to breakdown 1 cooked meal daily for 120 years. This means 80% of our diet should be raw
fruits and vegetables.
With the poor diet, particularly non-vegetarian food i.e. eating high fat meals daily, which the body
cannot utilize, most of us put tremendous strain on our pancreas and run out of enzymes by the time
we are 30-40 years old. It can take the body up to 8 hours to break down protein, and up to 48-72
hours to digest fats and carbohydrates. So now, you see that you constantly have undigested food
particles in the intestinal tract.
It has been estimated that the average person by the age of 40 has between 10-20 pounds of hard
compacted fecal matter lodged in their intestinal tract. Our intestinal tract is 30-35 feet in length. In
order to fully cleanse the digestive tract the solid compaction gets into a liquid or gas, using time
released oxygen and ozone (oxidation/reduction). By using Oxy-Powder, the toxic residue is oxidized
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
from the small intestine, large intestine and colon, safely and effectively. This is important because a
clean intestinal tract is the beginning of obtaining optimal health.
Oxy-Powder is harmless to the good bacteria in the intestinal tract. When the intestinal tract is fully
cleansed, the urine will become cloudy and the stools will become semi-solid. When this occurs, a
maintenance dose is recommended. This helps provide oxygen directly into the bloodstream. By
staying on a Maintenance Dosage of Oxy-Powder, the intestinal tract is kept clean and provides body
with much needed oxygen.
9.2 DOSAGE & ADMINISTRATION
For first time, it is recommended starting with a seven day initial cleanse. After the initial cleanse, a
maintenance dose is to be continued for keeping your intestinal tract clean and deliver oxygen into the
system. Patients are advised to take Oxy-Powder with plenty of purified water during the day and eat
healthy diet. The exact number of capsules to take will vary depending on body weight, previous
dietary habits, exercise patterns, and stress levels.
For Cleansing:
It is recommended to take four (4) capsules in the evening on an empty stomach with 240 mL water.
If 3-5 bowel movements are not achieved the following day, the dosage is increased by adding two (2)
capsules every night until 3-5 bowel movements are achieved the following day. Once the dosage is
finalized, it is day one (1) of the seven (7) day cleanse. This dosage is continued for seven (7)
consecutive days. After the seven (7) day cleanse, the maintenance dose is started.
Maintenance Dose:
The same dosage is to be taken same as that taken for seven (7) day cleanse, every other day. This can
be taken indefinitely without becoming habit forming or harmful to the body.
Drinking of lots of pure water is suggested. This is not only healthy for the body but will aid the body
in eliminating toxins from the bowel at a faster rate.
Oxy-Powder works with stomach acid; if the level of HCL is below normal, it may hinder the
effectiveness of the Oxy-Powder. It is suggested to take an organic lemon wedge squeezed into
glassful of purified water with the Oxy-Powder® in the evening.
• These statements are based upon the literature reports on patient results, clinical observation, and
customer feedback
9.3 DOSE RATIONALE
Dose of 4 capsules per day for first 7 days administered for cleansing followed by administration of 4
capsules on alternate days as maintenance dose is found to be effective.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
9.4 OVERDOSE:
No toxicity has been reported in the literature caused by overdose of Oxy-Powder®
9.5 PRECAUTIONS:
This product causes watery and gaseous stools which could cause the patient to feel the urge to pass
gas. If patient is not able to control bowels, he/she has to be careful when using this product. Close
availability to a bathroom is recommended during the 7-day cleanse. Oxy-Powder will cause watery,
gaseous stools. This is not diarrhea; this is the by-product of oxidation since a solid is turned into a
liquid or gas. To help the cleansing process, it is advised to drink plenty of purified water daily while
taking the Oxy-Powder; even though there has never been a documented case of dehydration or
electrolyte imbalances.
9.6 OCCUPATIONAL SAFETY
Investigational product is not expected to pose significant occupational safety risk to site staff under
normal conditions of use and administration. A Material Safety Data Sheet (MSDS) describing
occupational hazards and recommended handling precautions either will be provided to the
investigator (where this is required by local laws) or is available upon request from MCERC
However, precautions are to be taken to avoid direct skin contact, eye contact, and generating aerosols
or mists. In the case of unintentional occupational exposure, treat as if the substance contains the
active pharmaceutical even though it is absent from placebo formulations, and notify the monitor.
Precaution will be taken to avoid direct contact with the investigational product. A Material Safety
Data Sheet (MSDS) describing occupational hazards and recommended handling precautions will be
provided to the investigator.
9.7 CONCOMITANT MEDICATIONS AND NON-DRUG THERAPIES
There are no contraindications reported when taking Oxy-powder with prescription medicines as long
as the Oxy-Powder® is taken 6 hours before or 6 hours after the. permitted medications
All concomitant medications taken during the study will be recorded in the CRF with indication, dose
information, and dates of administration.
Prohibited Medications
Laxatives, anti-diarrhoels and anti-spasmodics
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
10.0 STUDY DESIGN:
Multicentric, Open, Comparative, Randomized, Phase III, Clinical trial comparing Oxy-powder
developed by Global Healing Centre Inc., USA with Dulcolax tablets (containing 5 mg Bisacodyl)
manufactured by Cadila Health Care Ltd.
10.1 STUDY DURATION:
6 weeks from the date of administration of study products.
11.0 EVALUATIONS
IN-VITRO EVALUATION OF INVESTIGATIONAL PRODUCT:
Toxicological studies:
Sub-acute: 28 days
2. Anti-microbial activity against 4 bacteria (including a Probiotic strain) and 1 parasite from amongst
the colonies present in GIT
11.2 PRE-STUDY EXAMINATION OF INCLUDED SUBJECTS FOR THE FOLLOWING:
Height and weight
Oxygen content of blood
Barium meal X-ray
Colonoscopy with minimal cleansing to see how mucoid plaque is present in the bowel.
Stool examination for dead parasites, toxic compounds etc.
11.3 PARAMETERS FOR POST-ADMINISTRATION EVALUATIONS IN ‘INCLUDED'
SUBJECTS FOR THE FIRST SEVEN DAYS:
1. Height and Weight check every day
2. Oxygen content of blood On Day ‘0', ‘3 Week' And ‘6 Week' both for test and control group.
The subjects from both the groups shall be called in the morning on empty stomach. Group
administered "Oxy-Powder®' shall be administered capsules and their Oxygen levels shall be
determined at '15 min' and '30 min.' post administration of the dose. In Dulcolax group of patients,
based on the enrollment days, they shall be called exactly on the days as decided for Oxy-Powder® on
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
days ‘0', ‘3 weeks' and ‘6 weeks'. Since they are comparative group, their Oxygen level shall be
measured without administering Dulcolax, '15 min' and '30 min' after their arrival.
3. Colonoscopy (after completion of the study at the end of 6 weeks)
4. Barium meal X-ray (after completion of the study at the end of 6 weeks)
5. Stool analysis (at the end of 3 weeks and at the end of 6 weeks)
6. The effectiveness of the product in treating constipation
7. The effectiveness of the product in body detoxification
8. The effectiveness of the product for Oxygen delivery and amount of oxygen delivered per
12.0 TREATMENT OF INVESTIGATIONAL PRODUCT:
Subject shall be instructed to take four capsules of Oxy-Powder® (Test formulation) or two tablets of
Dulcolax (Reference formulation), as per the Randomization scheme, with plenty of water, every day,
for first 7 days, in the evening on empty stomach.Thereafter, subjects shall be instructed to take the
same dose of either test or reference formulation on alternate days, on empty stomach, in the evening,
for 6 weeks. Administration on day ‘0', ‘3 weeks' and ‘6 weeks' shall be done on empty stomach (to
enable measuring Oxygen levels) in the morning. Subjects shall be asked to report to the hospital with
empty stomach; in the morning for administration of Investigational Products and Oxygen level in the
blood shall be measured 15 minutes and 30 minutes after administration of tablets/ capsules.
On the remaining days, the subjects shall take Investigational product at home at the same dose levels
in the evening on empty stomach. Dinner shall follow at least two hours post-administration of
13.0 Blinding
Treatment Assignment
Subjects will be assigned to study treatment in accordance with the randomization schedule.
14.0 HANDLING AND STORAGE OF INVESTIGATIONAL PRODUCT:
Investigational product must be dispensed or administered according to procedures described herein.
Only subjects enrolled in the study may receive investigational product, in accordance with all
applicable regulatory requirements. Only authorized site staff may supply or administer
investigational product. All investigational products must be stored in a secure area with access
limited to the investigator and authorized site staff and under physical conditions that are consistent
with investigational product-specific requirements.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
14.1 Product Accountability
The investigator is responsible for investigational product accountability, reconciliation, and record
maintenance. In accordance with all applicable regulatory requirements, the investigator or designated
site staff must maintain investigational product accountability records throughout the course of the
study. This person(s) will document the amount of investigational product received from MCERC, the
amount supplied and/or administered to and returned by subjects, if applicable.
14.2 Assessment of Compliance
A diary card will be given to the patients during the entire course of the clinical trial which will record
the number of capsules/ tablets taken and number of stools passed. Diary card will be issued at day
‘0', week 3 and week 6 after collecting the previously completed diary filled every day from the
concerned patient. Patient shall be required to contact his physician.
15.0 SUBJECT COMPLETION AND WITHDRAWAL
15.1 Subject Completion
All subjects completing six weeks of treatment will be included in the final report.
15.2 Subject Withdrawal from Study
If a subject who has consented to participate in research withdraws from the clinical study for any
reason other than lost to follow-up, the subject will be asked to give consent for withdrawal with or
without the reason for withdrawal. Such subject shall be taken as ‘drop-out'.
15.3 Screen and Baseline Failures:
Not applicable since the study is non-invasive
16.0 ADVERSE EVENTS (AE) AND SERIOUS ADVERSE EVENTS (SAE)
The investigator is responsible for the detection and documentation of events meeting the criteria and
definition of an AE or SAE as provided in this protocol. During the study, when there is a safety
evaluation, the investigator or site staff will be responsible for detecting AEs and SAEs, as detailed in
this section of the protocol.
16.1 Definition of an AE
Any untoward medical occurrence in a patient or clinical investigation subject, temporally associated
with the use of a medicinal product, whether or not considered related to the medicinal product.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
An AE can therefore be any unfavorable and unintended sign (including an abnormal laboratory
finding), symptom, or disease (new or exacerbated) temporally associated with the use of a medicinal
product. For marketed medicinal products, this also includes failure to produce expected benefits (i.e.
lack of efficacy), abuse or misuse.
Examples of an AE include:
Significant or unexpected worsening or exacerbation of the condition/indication under study. See
Section 10.3., "Lack of Efficacy", for additional information.
Exacerbation of a chronic or intermittent pre-existing condition including either an increase in
frequency and/or intensity of the condition.
New conditions detected or diagnosed after investigational product administration even though it
may have been present prior to the start of the study.
Signs, symptoms, or the clinical sequel of a suspected interaction.
Signs, symptoms, or the clinical sequel of a suspected overdose of either investigational product
or a concurrent medication (overdose per se should not be reported as an AE/SAE).
Significant failure of expected pharmacological or biological action. See Section 10.3., "Lack of
Efficacy" for additional information.
Lack of Efficacy
"Lack of efficacy" per se will not be reported as an AE. The signs and symptoms or clinical sequel
resulting from lack of efficacy will be reported if they fulfill the AE or SAE definition (including
clarifications).
The signs and symptoms, clinical sequel resulting from lack of efficacy, or both will be reported. In
this study, failure of expected pharmacological action also constitutes an AE and will be reported as
such in addition to the signs and symptoms.
Examples of an AE does not include a/an:
Medical or surgical procedure (e.g., endoscopy, appendectomy); that leads to the condition
Situations where an untoward medical occurrence did not occur (social and/or convenience
admission to a hospital).
Anticipated day-to-day fluctuations of pre-existing disease(s) or condition(s) present or
detected at the start of the study that do not worsen.
The disease/disorder being studied or expected progression, signs, or symptoms of the
disease/disorder being studied, unless more severe than expected for the subject's condition.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
For MCERC clinical studies, AEs may include pre- or post-treatment events that occur as a result of
protocol-mandated procedures (i.e. invasive procedures, modification of subject's previous
therapeutic regimen).
16.3 Definition of a SAE
A serious adverse event is any untoward medical occurrence that, at any dose:
a) Results in death.
b) Is life threatening.
NOTE: The term 'life-threatening' in the definition of 'serious' refers to an event in which the subject
was at risk of death at the time of the event. It does not refer to an event, which hypothetically might
have caused death, if it were more severe.
c) Requires hospitalization or prolongation of existing hospitalization.
NOTE: In general, hospitalization signifies that the subject has been detained (usually involving at
least an overnight stay) at the hospital or emergency ward for observation and/or treatment that would
not have been appropriate in the physician's office or out-patient setting. Complications that occur
during hospitalization are AEs. If a complication prolongs hospitalization or fulfills any other serious
criteria, the event is serious. When in doubt as to whether "hospitalization" occurred or was
necessary, the AE should be considered serious.
Hospitalization for elective treatment of a pre-existing condition that did not worsen from baseline is
not considered an AE.
d) Results in disability/incapacity, or
NOTE: The term disability means a substantial disruption of a person's ability to conduct normal life
functions. This definition is not intended to include experiences of relatively minor medical
significance such as uncomplicated headache, nausea, vomiting, diarrhea, influenza, and accidental
trauma (e.g. sprained ankle) which may interfere or prevent everyday life functions but do not
constitute a substantial disruption.
e) Is a congenital anomaly/birth defect.
Medical or scientific judgment should be exercised in deciding whether reporting is appropriate in
other situations, such as important medical events that may not be immediately life threatening or
result in death or hospitalization but may jeopardize the subject or may require medical or surgical
intervention to prevent one of the other outcomes listed in the above definition. These should also be
considered serious. Examples of such events are invasive or malignant cancers, intensive treatment in
an emergency room or at home for allergic bronchospasm, blood dyscrasias or convulsions that do not
result in hospitalization, or development of drug dependency or drug abuse.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
16.4 Disease-Related Events or Outcomes Not Qualifying as SAEs
16.5 Clinical Laboratory Abnormalities and Other Abnormal Assessments as AEs and SAEs
Abnormal laboratory findings (e.g., clinical chemistry, hematology, urinalysis) or other abnormal
assessments (e.g., [Insert relevant examples of assessments applicable to the study, such as ECG's, X-
rays, vital signs, etc.] that are judged by the investigator as clinically significant will be recorded as
AEs or SAEs if they meet the definition of an AE, as defined in Section 10.1. ("Definition of an AE")
or SAE, as defined in Section10.2. ("Definition of a SAE"). Clinically significant abnormal laboratory
findings or other abnormal assessments that are detected during the study or are present at baseline
and significantly worsen following the start of the study will be reported as AEs or SAEs. However,
clinically significant abnormal laboratory findings or other abnormal assessments that are associated
with the disease being studied, unless judged by the investigator as more severe than expected for the
subject's condition, or that are present or detected at the start of the study and do not worsen, will not
be reported as AEs or SAEs.The investigator will exercise his or her medical and scientific judgment
in deciding whether an abnormal laboratory finding or other abnormal assessment is clinically
As defined by the protocol in Section 10.2., "Definition of a SAE", all Grade 4 laboratory
abnormalities will be reported as SAEs.
Time Period, Frequency, and Method of Detecting AEs and SAEs
16.6 Recording of AEs and SAEs
When an AE/SAE occurs, it is the responsibility of the investigator to review all documentation (e.g.,
hospital progress notes, laboratory, and diagnostics reports) relative to the event. The investigator will
then record all relevant information regarding an AE/SAE on the CRF. It is not acceptable for the
investigator to send photocopies of the subject's medical records to MCERC in lieu of completion of
the appropriate AE/SAE CRF pages. However, there may be instances when copies of medical
records for certain cases are requested by MCERC. In this instance, all subject identifiers will be
blinded on the copies of the medical records prior to submission to MCERC.
The investigator will attempt to establish a diagnosis of the event based on signs, symptoms, and/or
other clinical information. In such cases, the diagnosis should be documented as the AE/SAE and not
the individual signs/symptoms.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
AEs and subject-completed questionnaires are independent components of the study. Responses to
each question in the questionnaires will be treated in accordance with standard scoring and statistical
procedures detailed by the scale's developer. The use of a single question from a multidimensional
health survey to designate a cause-effect relationship to an AE is inappropriate.
16.7 Evaluating AEs and SAEs
16.7.1 Assessment of Intensity
The investigator will make an assessment of intensity for each AE and SAE reported during the study.
The assessment will be based on the investigator's clinical judgment. The intensity of each AE and
SAE recorded in the CRF should be assigned to one of the following categories:
Mild: An event that is easily tolerated by the subject, causing minimal discomfort and not interfering
with everyday activities.
Moderate: An event that is sufficiently discomforting to interfere with normal everyday activities.
Severe: An event that prevents normal everyday activities.
An AE that is assessed as severe should not be confused with a SAE. Severity is a category utilized
for rating the intensity of an event; and both AEs and SAEs can be assessed as severe. An event is
defined as ‘serious' when it meets one of the pre-defined outcomes as described in Section 10.2.,
"Definition of a SAE".
16.7.2 Assessment of Causality
The investigator is obligated to assess the relationship between investigational product and the
occurrence of each AE/SAE. The investigator will use clinical judgment to determine the relationship.
Alternative causes, such as natural history of the underlying diseases, concomitant therapy, other risk
factors, and the temporal relationship of the event to the investigational product will be considered
and investigated. The investigator will also consult the CIB/IB and/or Product Information, for
marketed products, in the determination of his/her assessment.
There may be situations when an SAE has occurred and the investigator has minimal information to
include in the initial report to MCERC. However, it is very important that the investigator always
make an assessment of causality for every event prior to transmission of the SAE CRF to MCERC
The investigator may change his/her opinion of causality in light of follow-up information, amending
the SAE CRF accordingly. The causality assessment is one of the criteria used when determining
regulatory reporting requirements.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
The investigator will provide the assessment of causality as per instructions on the SAE form in the
16.7.3 Follow-Up of AEs and SAEs
After the initial AE/SAE report, the investigator is required to proactively follow each subject and
provide further information to MCERC on the subject's condition.
All AEs and SAEs documented at a previous visit/contact and are designated as ongoing, will be
reviewed at subsequent visits/contacts.
All AEs and SAEs will be followed until resolution, until the condition stabilizes, until the event is
otherwise explained, or until the subject is lost to follow-up. Once resolved, the appropriate AE/SAE
CRF page(s) will be updated. The investigator will ensure that follow-up includes any supplemental
investigations as may be indicated to elucidate the nature and/or causality of the AE or SAE. This
may include additional laboratory tests or investigations, Histopathological examinations, or
consultation with other health care professionals.
MCERC may request that the investigator perform or arrange for the conduct of supplemental
measurements and/or evaluations to elucidate as fully as possible the nature and/or causality of the AE
or SAE. The investigator is obligated to assist. If a subject dies during participation in the study or
during a recognized follow-up period, MCERC will be provided with a copy of any post-mortem
findings, including histopathology.
New or updated information will be recorded on the originally completed "SAE" CRF, with all
changes signed and dated by the investigator. The updated SAE CRF should be resent to MCERC
within the timeframes outlined in Section 10.9.
17.0 Prompt Reporting of SAEs to MCERC Required Standard Wording:
SAEs will be reported promptly to MCERC as described in the following table once the investigator
determines that the event meets the protocol definition of an SAE.
17.1 Timeframes for Submitting SAE Reports to MCERC
Initial SAE Reports
Follow-up Information on a
Previously Reported SAE
"SAE" CRF
"SAE" CRF
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Initial SAE Reports
Follow-up Information on a
Previously Reported SAE
17.2 Completion and Transmission of the SAE Reports
Once an investigator becomes aware that an SAE has occurred in a study subject, she/he will report
the information to MCERC within 24 hours as outlined in Section 10.9., "Prompt Reporting of SAEs
to MCERC. The SAE CRF will always be completed as thoroughly as possible with all available
details of the event, signed by the investigator (or designee), and forwarded to MCERC within the
designated time frames. If the investigator does not have all information regarding an SAE, he/she
will not wait to receive additional information before notifying MCERC of the event and completing
the form. The form will be updated when additional information is received.
The investigator will always provide an assessment of causality at the time of the initial report as
described in Section 10.7.2., "Assessment of Causality".
Facsimile transmission of the "SAE" CRF is the preferred method to transmit this information to the
project contact for SAE receipt. In rare circumstances and in the absence of facsimile equipment,
notification by telephone is acceptable, with a copy of the "SAE" CRF sent by overnight mail. Initial
notification via the telephone does not replace the need for the investigator to complete and sign the
SAE CRF within the timeframes outlined in Section 10.9., "Prompt Reporting of SAEs to MCERC".
MCERC will provide a list of project contacts for SAE receipt, fax numbers, telephone numbers, and
mailing addresses.
The following pages of the CRF must accompany the SAE forms that are forwarded to MCERC:
"Demography", "Medical History", "Concomitant Medications", "Study Medication Records", and
"Form D" (if applicable).
17.3 Regulatory Reporting Requirements for SAEs
The investigator will promptly report all SAEs to MCERC in accordance with the procedures detailed
in Section 10.9., "Prompt Reporting of SAEs to MCERC." MCERC has a legal responsibility to
notify, as appropriate, both the local regulatory authority and other regulatory agencies about the
safety of a product under clinical investigation. Prompt notification of SAEs by the investigator to the
appropriate project contact for SAE receipt is essential so that legal obligations and ethical
responsibilities towards the safety of other subjects are met.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
The investigator, or responsible person according to local requirements, will comply with the
applicable local regulatory requirements related to the reporting of SAEs to regulatory authorities and
the Institutional Review Board (IRB)/Independent Ethics Committee (IEC).
This protocol may be filed under an Investigational New Drug (IND) application / dietary supplement
with the US Food and Drug Administration (FDA). A given SAE may qualify as an IND Safety
Report if the SAE is both attributable to the investigational product and unexpected. In this case, all
investigators filed to the IND (and associated IND's for the same compound) will receive an
Expedited Investigator Safety Report (EISR), identical in content to the IND Safety Report submitted
Ears are prepared according to MCERC policy and are forwarded to investigators as required. An
EISR is prepared for a SAE that is both attributable to investigational product and unexpected. The
purpose of the EISR is to fulfill specific regulatory and Good Clinical Practice (GCP) requirements,
regarding the product under investigation.
When a site receives from MCERC an Initial or Follow-up EISR or other safety information (e.g.,
revised Clinical Investigator's Brochure/Investigator's Brochure), the responsible person according to
local requirements is required to promptly notify his or her IRB or IEC.
Expedited Investigator Safety Reports (EISR) are prepared according to MCERC policy and are
forwarded to investigators as necessary. An EISR is prepared for a SAE that is both attributable to
investigational product and unexpected. The purpose of the EISR is to fulfill specific regulatory and
Good Clinical Practice (GCP) requirements, regarding the product under investigation.
An investigator who receives an EISR describing a SAE or other specific safety information from
MCERC will file it with the Investigator Brochure and will notify the IRB or IEC, if appropriate
according to local requirements.
17.4 Post-study AEs and SAEs
A post-study AE/SAE is defined as any event that occurs outside of the AE/SAE detection period
defined in Section 10.5., "Time Period, Frequency, and Method of Detecting AEs and SAEs", of the
protocol. Investigators are not obligated to actively seek AEs or SAEs in former study participants.
However, if the investigator learns of any SAE, including a death, at any time after a subject has been
discharged from the study, and he/she considers the event reasonably related to the investigational
product, the investigator will promptly notify MCERC
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
17.5 SAEs Related to Study Participation
An SAE considered related to study participation (e.g., procedures, invasive tests, a change in existing
therapy), even if it occurs during the pre- or post-treatment period, will be reported promptly to
MCERC (see Section 10.9., "Prompt Reporting of SAEs to MCERC ").
18.0 DATA ANALYSIS AND STATISTICAL CONSIDERATIONS
18.1 Hypotheses
Oxy-Powder® is both, safe and effective in patients with constipation and constipation in presence
18.2 Treatment Comparisons of Interest
18.3Primary Comparisons of Interest
This dietary supplement is to be compared for effectiveness in relieving constipation and IBS in two
groups of patients versus Dulcolax tablets in another two groups.
1.1 Other Comparisons of Interest
Comparison of safety of this product shall be done with safety of administering Dulcolax
18.5 Interim Analysis
Data shall be collected regularly but analyzed at the end of the study for safety and effectiveness of
the Oxy-Powder®.
18.6 Sample Size Considerations
The study design has been examined and approved by a qualified statistician with respect to sample
18.7 Analysis Populations
After the drop outs, it is assumed to have a minimum of 35 patients (out of 60) in constipation group
and 15 patients (out of 20) in constipation + IBS group.
18.8 Data Sets
Data set 1: for Constipation group
It shall be prepared at the end of the study, 1 each for Oxy-Powder® and Dulcolax
Data set 2: for IBS with Constipation group
This shall be prepared separately at the end of the study, 1 each for Oxy-Powder® and Dulcolax
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
18.9 Withdrawal
The patients voluntarily withdrawn from the study (dropouts) shall be documented but shall not be
included in the report.
1.0 Missing Data
Missing data not recorded by the patient shall be submitted separately by Mayfair
18.11 Statistical Analysis - Derived and Transformed Data
The pooled included in the report shall be statistically analysed for establishing its validity.
18.12 Other
Any other issues arising during conduct of the study informed by the investigator / CRA shall be
notified to the Sponsor.
1.1 Efficacy Analyses
Keeping in view, the evaluated parameters shall be compared with that obtained with Dulcolax
administered to the group of patients.
1.2 Safety Analyses (Adverse Events and Serious Adverse Events)
Any AEs and SAEs shall be reported immediately.
1.3 Clinical Laboratory Evaluations
Colonoscopy, Barium Meal X-ray, Stool analysis, Oxygen levels
1.4 Other Safety Measures
Observations on side effects including Diarrhea.
1.5 Health Outcomes Analyses
Loss of weight: Patient feels more fit.
19.0 REGULATORY AND ETHICAL CONSIDERATIONS
• Approval of Ethics Committee of Hospitals where study is conducted • IRB of MCERC
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
• Approval of DCGI for conducting study • Other regulatory agencies e.g. USFDA etc.
19.1 REGULATORY
AUTHORITY
APPROVAL
MAYFAIR will obtain approval to conduct the study from the appropriate regulatory agency e.g.
Drugs Controller General of India, in accordance with any applicable regulatory requirements prior to
a site initiating the study in India.
19.2 ETHICAL CONDUCT OF THE STUDY AND ETHICS APPROVAL
This study will be conducted in accordance with "good clinical practice" (GCP) and all applicable
regulatory requirements, including, where applicable, the [insert the appropriate date] version of the
Declaration of Helsinki.
The investigator (or sponsor, where applicable) is responsible for ensuring that this protocol, the site's
informed consent form, and any other information that will be presented to potential subjects (e.g.,
advertisements or information that supports or supplements the informed consent) are reviewed and
approved by the appropriate IEC/IRB. The investigator agrees to allow the IEC/IRB direct access to
all relevant documents. The IEC/IRB must be constituted in accordance with all applicable regulatory
requirements. MCERC will provide the investigator with relevant document(s)/data that are needed
for IEC/IRB review and approval of the study. Before investigational product(s) and CRF's can be
shipped to the site, MCERC must receive copies of the IEC/IRB approval, the approved informed
consent form, and any other information that the IEC/IRB has approved for presentation to potential
If the protocol, the informed consent form, or any other information that the IEC/IRB has approved
for presentation to potential subjects is amended during the study, the investigator is responsible for
ensuring the IEC/IRB reviews and approves, where applicable, these amended documents. The
investigator must follow all applicable regulatory requirements pertaining to the use of an amended
informed consent form including obtaining IEC/IRB approval of the amended form before new
subjects consent to take part in the study using this version of the form. Copies of the IEC/IRB
approval of the amended informed consent form/other information and the approved amended
informed consent form/other information must be forwarded to MCERC promptly.
IEC/IRB approval of the consent forms must be obtained in addition to the approval given for the
clinical study. Regulatory review and approval may be required in some countries before IEC/IRB
approval can be sought.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
19.3 INFORMED CONSENT
Informed consent will be obtained before the subject can participate in the study. The contents and
process of obtaining informed consent will be in accordance with all applicable regulatory
Subjects who do not wish to participate in the PGX research may still participate in the clinical study.
For each subject, informed consent must be obtained prior to any blood being taken for research. The
informed consent for the research must be obtained in addition to the subject's consent to participate
in the clinical study.
20.0 INVESTIGATOR REPORTING REQUIREMENTS
As indicated earlier, the investigator (or sponsor, where applicable) is responsible for reporting SAEs
to the IEC/IRB, in accordance with all applicable regulations. Furthermore, the investigator may be
required to provide periodic safety updates on the conduct of the study at his or her site and
notification of study closure to the IEC/IRB. Such periodic safety updates and notifications are the
responsibility of the investigator and not of MCERC
21.0 STUDY MONITORING
In accordance with applicable regulations, GCP, and MCERC procedures, MCERC monitors will
contact the site prior to the subject enrollment to review the protocol and data collection procedures
with site staff. In addition, the monitor will periodically contact the site, including conducting on-site
visits. The extent, nature and frequency of on-site visits will be based on such considerations as the
study objective and/or endpoints, the purpose of the study, study design complexity, and enrollment
During these contacts, the monitor will:
Check the progress of the study.
Review study data collected.
Conduct source document verification.
Identify any issues and address their resolution.
This will be done in order to verify that the:
Data are authentic, accurate, and complete.
Safety and rights of subjects are being protected.
Study is conducted in accordance with the currently approved protocol (and any amendments),
GCP, and all applicable regulatory requirements.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
The investigator agrees to allow the monitor direct access to all relevant documents and to allocate
his/her time and the time of his/her staff to the monitor to discuss findings and any relevant issues.
At study closure, monitors will also conduct all activities described in Section 23 "Study and Site
The monitor will also review subject-completed health outcomes questionnaire(s) for extraneous
written comments that could indicate possible AEs. Information collected in the CRF and in the
subject-completed health outcomes questionnaire(s) are independent components of this study. Except
for header section information (e.g., subject number, treatment number, visit date) and other
information as defined in the standard clarification agreement (SCA), neither the monitor nor the
investigator will attempt to reconcile responses to individual questions/items recorded on the subject-
completed health outcomes questionnaire(s) or health outcomes portions of diary cards (if applicable)
with other data recorded in the CRF's. Subject-completed health outcome questionnaires generally
serve as the source document; therefore, unless otherwise specified elsewhere, no other source
document is available for data validation.
22.0 QUALITY ASSURANCE
To ensure compliance with GCP and all applicable regulatory requirements, MCERC may conduct a
quality assurance audit. Regulatory agencies may also conduct a regulatory inspection of this study.
Such audits/inspections can occur at any time during or after completion of the study. If an audit or
inspection occurs, the investigator and institution agree to allow the auditor/inspector direct access to
all relevant documents and to allocate his/her time and the time of his/her staff to the auditor/inspector
to discuss findings and any relevant issues.
23.0 STUDY AND SITE CLOSURE
Upon completion of the study, the monitor will conduct the following activities in conjunction with
the investigator or site staff, as appropriate: [Insert relevant activities, including but not limited to the
following, if they are applicable to the study:
• Return of all study data to MCERC data queries.
• Accountability, reconciliation, and arrangements for unused investigational product(s). • Review of site study records for completeness. • Return of treatment codes to MCERC In addition, MCERC reserves the right to temporarily
suspend or prematurely discontinue this study either at a single site or at all sites at any time for
reasons including, but are not limited to, safety or ethical issues or severe non-compliance. If MCERC
determines such action is needed, MAYFAIR will discuss this with the Investigator (including the
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
reasons for taking such action) at that time. When feasible, MCERC will provide advance notification
to the investigator of the impending action prior to it taking effect.
MAYFAIR will promptly inform all other investigators and/or institutions conducting the study if the
study is suspended or terminated for safety reasons, and will also inform the regulatory authorities of
the suspension or termination of the study and the reason(s) for the action. If required by applicable
regulations, the investigator must inform the IEC/IRB promptly and provide the reason for the
suspension or termination.
If the study is prematurely discontinued, all study data must be returned to MCERC. In addition,
arrangements will be made for all unused investigational product(s) in accordance with the applicable
MCERC procedures for the study.
Financial compensation to investigators and/or institutions will be in accordance with the agreement
established between the investigator and MCERC
24.0 RECORDS RETENTION
Following closure of the study, the investigator must maintain all site study records in a safe and
secure location. The records must be maintained to allow easy and timely retrieval, when needed (e.g.,
audit or inspection), and, whenever feasible, to allow any subsequent review of data in conjunction
with assessment of the facility, supporting systems, and staff. Where permitted by local
laws/regulations or institutional policy, some or all of these records can be maintained in a format
other than hard copy (e.g., microfiche, scanned, electronic); however, caution needs to be exercised
before such action is taken. The investigator must assure that all reproductions are legible and are a
true and accurate copy of the original and meet accessibility and retrieval standards, including re-
generating a hard copy, if required. Furthermore, the investigator must ensure there is an acceptable
backup of these reproductions and that an acceptable quality control process exists for making these
MCERC will inform the investigator of the time period for retaining these records to comply with all
applicable regulatory requirements. The minimum retention time will meet the strictest standard
applicable to that site for the study, as dictated by any institutional requirements or local laws or
regulations of MCERC standards/procedures; otherwise, the retention period will default to 15 years.
The investigator must notify MCERC of any changes in the archival arrangements, including, but not
limited to, the following: archival at an off-site facility, transfer of ownership of the records in the
event the investigator leaves the site.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
25.0 PROVISION OF STUDY RESULTS AND INFORMATION TO INVESTIGATORS
When a clinical study report is completed, MCERC will provide the major findings of the study to the
In addition, details of the study treatment assignment will be provided to the investigator to enable
him/her to review the data to determine the outcome of the study for his/her subject.
MCERC may list and summarize the PGX research results from coded samples by subject number in
the clinical study report. In this event, the investigator and study staff would have access to the
research results and would be able to link the results to a particular subject. The investigator and study
staff would be directed to hold this information confidentially.
26.0 INFORMATION DISCLOSURE AND INVENTIONS
26.1 Ownership:
All information provided by MCERC and all data and information generated by the site as part of the
study (other than a subject's medical records) are the sole property of MCERC All rights, title, and
interests in any inventions, know-how or other intellectual or industrial property rights which are
conceived or reduced to practice by site staff during the course of or as a result of the study are the
sole property of MCERC and are hereby assigned to MCERC.
If a written contract for the conduct of the study which includes ownership provisions inconsistent
with this statement is executed between MCERC and the study site, that contract's ownership
provisions shall apply rather than this statement.
This includes the results of the PGX assessments included in the study.
26.2 Confidentiality:
All information provided by MCERC and all data and information generated by the site as part of the
study (other than a subject's medical records) will be kept confidential by the investigator and other
site staff. This information and data will not be used by the investigator or other site personnel for any
purpose other than conducting the study. These restrictions do not apply to: (1) information which
becomes publicly available through no fault of the investigator or site staff; (2) information which it is
necessary to disclose in confidence to an IEC or IRB solely for the evaluation of the study;
(3) information which it is necessary to disclose in order to provide appropriate medical care to a
study subject; or (4) study results which may be published as described in the next paragraph. If a
written contract for the conduct of the study which includes confidentiality provisions inconsistent
with this statement is executed, that contract's confidentiality provisions shall apply rather than this
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
26.3 Publication:
For multicentric studies, the first publication or disclosure of study results shall be a complete, joint
multicentric publication or disclosure coordinated by MCERC. Thereafter, any secondary publications
will reference the original publication(s).
Prior to submitting for publication, presentation, use for instructional purposes, or otherwise
disclosing the study results generated by the site (collectively, a "Publication"), the investigator shall
provide MCERC with a copy of the proposed Publication and allow MCERC a period of at least thirty
(30) days [or, for abstracts, at least five (5) working days] to review the proposed Publication.
Proposed Publications shall not include either MCERC confidential information other than the study
results or personal data on any subject, such as name or initials.
At MCERC's request, the submission or other disclosure of a proposed Publication will be delayed a
sufficient time to allow MCERC to seek patent or similar protection of any inventions, know-how or
other intellectual or industrial property rights disclosed in the proposed Publication.
If a written contract for the conduct of the study, which includes publication provisions inconsistent
with this statement is executed, that contract's publication provisions shall apply rather than this
It is mandatory to inform and register with the Association of publishers of Medical General, the
Clinical trial details, before commencement of the study.
Ref: The International Committee of Medical Journal Editors (ICMJE) Policy dtd. May 23, 2004,
27.0 DATA MANAGEMENT
Subject data are collected by the investigator or designee using the Case Report Form (CRF) defined
by MCERC Subject data necessary for analysis and reporting will be entered / transmitted into a
validated database or data system. Clinical data management will be performed in accordance with
applicable MCERC standards and data cleaning procedures. Database freeze will occur when data
management quality control procedures are completed. Original CRF's will be retained by MCERC,
while the investigator will retain a copy.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
MAYFAIR CLINICAL, EDUCATION & RESEARCH CENTRE, THANE
Clinical Study Report– Constipation
Randomization Schedule
No. of Patients: 40 A = Oxy-Powder® B = Dulcolax
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
CASE REPORT FORM
DOCUMENT NO.: MCERC/PROT-CLTR/OXY/1205/001
Version 02, December 20, 2005
CLINICAL TRIAL PHASE III
SAFETY AND EFFICACY OF
Mayfair Clinical, Education and Research Centre, Thane
Confidentiality Statement:
The information provided in this document is strictly confidential and is available for review to
Investigators, potential investigators and appropriate Ethics committees. No disclosure should take
place without written authorization from the Sponsor except to the extent necessary to obtain
Informed Consent from potential subjects.
Procedures at each Visit:
Procedures Visit
Remarks:
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
BHATIA HOSPITAL
PRINCIPAL INVESTIGATOR
DR. SHARAD SHAH'S CLINIC
CO INVESTIGATOR
DR. ADITI
INSTRUCTIONS FOR THE INVESTIGATORS:
1. Please enter all the data in black ball-point pen only.
2. Please enter the Subject no. on the Case Record Form (CRF)
3. Please complete all entries in CRF and do not leave any blank spaces. Please (x) in the
appropriate boxes. If data in not applicable, please enter NA, or if not done, enter ND
4. Do not rub, erase or use correction fluid for incorrect entries. For correction, if any, strike out
the incorrect answer and enter the correct entry alongside, initial the correction with date.
5. Use only standard abbreviations, if required.
6. In case of any further query, kindly contact:
Mayfair Clinical, Education and Research Centre, Thane
Tel: 91-22-2589 5856 Fax: 2589 5854 E-mail:
Dr. J.K. Lalla: Res: 91-22-28701161 Mob: 98205 23127
Dr. (Mrs.) Meena Shah Res: 91-22-22021296 Mob: 98203 17747
SCREENING VISIT (VISIT 0)
DATE: -----------------------------
SUBJECT CONSENT TAKEN: YES NO
(CONSENT FORM ENCLOSED)
Signature: _ Date: _
Subject
Signature: _ Date: _
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Investigator
Subject No. :
Subject Initials: _
Gender: Male Female
(Please cross ‘X')
Date of Birth: _ _
DD MM YY
Height: cm
Weight: kg
*LMP: _ _ _ Not applicable
DD MM YY
(* Last Menstruation Period)
Birth control measures taken: Give in brief
Educational Status:
School dropout: YES NO
If ‘Yes' give details:
High School College Graduate Post graduate
(If the subject has dropped out somewhere in between e.g. between Std. X and Std. XII then the box
corresponding to the last education completed has to be crossed.)
Subject No.:
SUBJECT HISTORY
(Please cross ‘X' in the appropriate box)
Constipation alone Constipation with IBS For Constipation with or without IBS, give following details:
1. Food habits: Vegetarian Non-vegetarian
2. Duration of Constipation: Weeks and Months
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
3. No. of bowel movements in a week:
4. Severity of disease: Mild Moderate: Severe:
5. Straining during bowel movement: Yes No
6. Urgency for passing stools: Yes No
7. Type of Constipation / IBS: Intermittent Persistent
8. Lumpy or hard stools Yes No
9. Loose or watery stools Yes No
10. Sensation of incomplete evacuation: Yes No
11. Sensation of anorectal blockage: Yes No
12. Passing mucus during bowel movement Yes No
13. Abdominal fullness / Yes No
14. Smoking History: Yes No
Diagnosis:
[III] HISTORY OF SIGNIFICANT ILLNESS
(Mention any significant/major illness or surgery)
Condition
(for a past illness, date when the event
stopped can also be mentioned here)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
[IV] HISTORY OF MEDICATIONS USE (PREVIOUS AND ONGOING)
Continued
Duration
If ‘No' period since
Drugs Condition
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
FAMILY HISTORY:
[V] CLINICAL EXAMINATION
VITAL SIGNS
(RIGHT ARM SITTING POSITION)
Respiratory rate:
Any abnormal finding (s) present? (please cross X)
YES COMMENTS
Respiratory System
Cardiovascular System
Abdominal System
Central Nervous System
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
[VI] SELECTION CRITERIA
(Please (X) Yes or No)
Subject aged 18-60 years
Rome II criteria for Constipation
Rome II criteria for IBS
Subject signing informed consent document.
Has the subject met the selection criteria:
(Note: If any of the shaded boxes is ticked ( √ ) the subject will be excluded from the study)
Investigator's name:
Investigator's signature and Date:
Subject No. Day
CLINICAL LABORATORY INVESTIGATIONS
PARAMETERS FINDING NORMAL RANGE
1. Oxygen content of blood after 15 minutes
2. Oxygen content of blood after 15 minutes
3. Stool examination
STUDY DRUG SHEET
Randomization code no.:
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Study drug dispensed:
Test (Oxy-Powder®) Reference (Dulcolax tablets)
Administration instructions:
For cleansing:
Take four capsules in the evening on empty stomach with plenty of water for seven days (from day 1,
every day up to 7th day)
Take two capsules in the evening on empty stomach for seven days (from day 1, every day up to 7th
For maintenance:
Take four capsules in the evening on empty stomach with plenty of water every alternate day for next
5 weeks (from day 8 to day 42)
Take two capsules in the evening on empty stomach with plenty of water every alternate day for next
5 weeks (from day 8 to day 42)
SUBJECT EVALUATION
(Please cross ‘X' in the appropriate box)
Constipation alone: Constipation with IBS: For Constipation with or without IBS, give following details:
1. Severity of disease: Mild Moderate: Severe:
2. Straining during bowel movement: Yes No
3. Urgency for passing stools: Yes No
4. Type of Constipation / IBS: Intermittent Persistent
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
5. Lumpy or hard stools Yes No
6. Loose or watery stools Yes No
7. Sensation of incomplete evacuation Yes No
8. Sensation of anorectic blockage: Yes No
9. Passing mucus during bowel movement Yes No
10. Abdominal fullness / bloating / swelling Yes No
11. Red flag symptoms Yes No (Page 21 of protocol)
ADVERSE EVENTS – after 1 week
Were there any adverse events? Yes No
Please complete all sections below, cross appropriate number(s)
Adverse Events, specify,
Description of AE Description of AE Description of AE
Please list ONE event per column. Give 1.
diagnosis if possible
2 Yes* (if yes fill the Serious Adverse Events form)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
(several statements are possible)
1. Results in death
2. Life threatening 3. In subject hospitalization or
prolongation of existing 4. Congenital anomaly/birth defect
5. Persistent or significant disability incapacity 6. Important medical event
A DATE & TIME
A Date & Time
C. 1. Continuous
If ongoing update at next visit
Severity
1. Mild: awareness of symptoms but
interfere with routine activities
2. Moderate: discomfort enough to
interfere with routine activities.
3. Severe: Impossible to perform
routine activities.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Relation to study design**
1. Certain. 2. Probable. 3. Possible. 1 2 3 4 5 6
4. Unlikely 5. Unclassified-conditional 6.
Unclassified-inaccessible
Action taken
(several statements are possible)
3. Dose of study drug reduced
3. Study drug discontinued and restarted
4. Study drug discontinued permanently
5. Remedial drug therapy, specify on
concomitant medication page
6. Other (specify below)
7. Hospitalization required or prolonged
ACTION TAKEN
1. Resolved
2. Improved
3. Unchanged
4. Worsened
6. Insufficient follow-up
ADR WAS EXPECTED?
1. Yes 2. No
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
ADVERSE EVENTS
*Any Serious Adverse Events seen: Yes No
If yes, please fill the form of Serious Adverse Event and notify the sponsor and Ethics Committee of the institute within 24 hrs.
Time & Date of notification to sponsor
Time & Date of notification to Ethics Committee
**Relationship to the drug in the investigational device.
1. Certain: a clinical event, including laboratory test abnormality, occurring in a plausible time
relationship to drug administration, and which cannot be explained by concurrent disease or other
drugs or chemicals. The response to withdrawal of the drug (dechallenge) should be clinically
plausible. The event must be definite pharmacologically or phenomenologically, using a
satisfactory rechallenge procedure is necessary.
1. Probable/ likely: a clinical event, including laboratory test abnormality, with a reasonable time
sequence to administration of the drug, unlikely to be attributed to reasonable response or
withdrawal (dechallenge). Rechallenge information is not required to fulfill this criterion.
2. Possible: a clinical event, including laboratory test abnormality, with a reasonable time
sequence to administration of the drug, but which could also be explained by concurrent disease
or other drug or chemicals. Information on drug withdrawal may be lacking or unclear.
3. Unlikely: a clinical event, including laboratory test abnormality, reported as an adverse
reaction about which more data is essential for a proper assessment or the additional data are
under examination.
4. Unclassified / inaccessible: A report suggesting an adverse reaction, which cannot be judged
because information is insufficient or contradictory, and which cannot be supplemented or
verified.
INVESTIGATOR'S SIGNATURE AND DATE
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
"EVALUATION AND ADR AND FINDINGS OF LAB INVESTIGATIONS" PAGES TO BE COPY
PASTED FOR THE END OF 3 WEEKS AND END OF 6 WEEKS FOR EVERY SUBJECT.
SUBJECT COMPLETION STATUS
Did the subject complete the study period?
To be completed only for subjects prematurely terminated
Primary reasons for termination:
Subject Non-compliance
Consent Withdrawn
Subject lost to follow up
Protocol violation
II. To be completed in all cases of death
Date of Death:
Cause of Death:
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
OVERALL THERAPEUTIC EFFECTIVENESS
ASSESSMENT BY THE INVESTIGATOR
ASSESSMENT BY THE PATIENT:
SIDE EFFECTS:
OVERALL EFFICACY RESPONSE
INVESTIGATOR'S SIGNATURE
Statement:
I certify that the entries on all pages of the case report form accurately and completely represent results of the examination, tests and evaluations performed on the dates specified. I was personally familiar with the clinical presentation and progress of the study subject.
Investigator's name:
Investigator's Signature and Seal Date
Patient Informed Consent
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506

MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
REPORT FOR
CLINICAL TRIAL PHASE III
SAFETY AND EFFICACY OF OXY-POWDER®
VERSION 01
DOCUMENT NO.: MCERC/REPT-CLTR/OXY/1205/001 ghanima
May 30th 2007
TRIAL TO STUDY SAFETY AND EFFECTIVENESS OF OXY-POWDER® IN TREATING
IBS with related constipation.
MAYFAIR CLINICAL EDUCATION RESEARCH CENTRE,
(A KALTHIA GROUP ORGANIZATION)
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Ph. No. 91-022-2589 5856 Fax. 91-022-2589 5854
e-mail [email protected]
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Part–4 B
CLINICAL STUDY REPORT
ON OXY-POWDER®
CLINICAL STUDY REPORT ON OXYPOWDER-CONSTIPATION+IBS
Table of Contents
2 ABSTRACT
CONTENTS
4 SYNOPSIS
5 ADMINISTRATIVE
STATEMENTS
a) Glossary
(b) Regulatory Approvals
c) Statement of final approval of the report
director, statistician, investigators, etc.
1.0 INTRODUCTION
1.1 Constipation
1.2 IBS
1.3 Introduction to Rome II Criteria
1.31 Rome II Criteria for Constipation
1.32 Rome II Criteria for IBS
2.1-2.2 IBS diagnosis
2.3 Red Flag Symptoms(not of IBS)
3.1 Oxy-Powder®
3.1.1 Germanium-132
3.2 Bisacodyl
RATIONALE
4.1 OBJECTIVES OF THE STUDY
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
5.0 METHODOLOGY
5.0.1 Conduct (including Ethical conduct) of Study
5.0.2 Subject Information and Consent
5.0.3 Investigator& Study Centre
5.1.1Study Design, and Duration
5.2 Procedure for Conduct of study
5,2.1 Study Population
5,2.2 No. of Patients enrolled
5.3–5.4 Patient selection and inclusion Criteria
5.4.1 Rome II Criteria for IBS
5.4.2 Symptoms that cumulatively support the diagnosis of
5.5 Supportive symptoms of IBS
5.6 Red flag symptoms which are not typical of IBS
5.7 Diagnosis of IBS
5.8 Subject Exclusion Criteria
6.0 Study Procedure and Treatment
7.0Treatment and Timings
7.1 Dosage and Administration
7.2 Study Assessment
7.3 End Points
8.0 Demography
Grading of Response
9.0 Efficacy
10.0 Safety
11.0 Withdrawal from study
12.0 Statistics and data handling
13.0 Other Issues
14.0 Ethics
15.0 Ethical Conduct and Approval of Studies
15.1 Informed Consent
16.0 Protocol compliance
17.0 Handling and storage of Investigational Products
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
17.1 Product Accountability
18.0 Assessment Compliance
18.1 Screen and Baseline failures
Monitoring
Assurance
21.0 Study and Site Closure
22.0 Data Management
23.0 Statistical Analysis
24.0 Records Retention
25.0 Provision of study results and information to
26.0 Information disclosure and inventions
Ownership
26.2 Confidentiality
Publication
10 Results
(a) Descriptive
(b) Efficacy
(c) Safety
Discussion and Summary
12 Conclusions
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
LIST OF TABLES (Constipation-IBS)
TABLE NO. CONTENT
18 Demographic
20 Smoking
Duration of Constipation (in months)
No. Of Bowels in a Week for OP and DL on day 0 for
Classifying Patients before study commenced
Severity of Constipation
24 Randomization
Comparison of Weight (kg) (Day 0-Day 42)
No. Of Bowels in a Week (Day 0, 21 and 42)
Oxygen Content of Blood (Day 0, 21 and 42)
Straining During >25% of Bowel Movement [ (a) Day
0,(b)Day21,(c) Day 42) ]
Lumpy Stools [ (a) Day 0, (b) Day21 and (c) Day42 ]
30 Sensation
incomplete
evacuation for >25% of Bowel
Movement[(a)Day 0 (b)Day 21 and (c) Day 42)]
Sensation of Anorectal Blockage for >25% of Bowel
Movement.[(a)Day 0, (b) Day 21 and (c) Day 42)]
Manual Manoeuvres to facilitate >25% of Bowel
Movements[(a)Day 0 (b) Day 21 and (c) Day 42)]
Abdominal Pain relieved with Defecation [(a)Day 0 (b)
Day 21 and (c) Day 42)]
Abdominal Pain onset associated with a change in
frequency of stools[(a)Day 0 (b) Day 21 and (c) Day 42)]
Abdominal Pain onset associated with a change in form of
stools[(a)Day 0 (b) Day 21 and (c) Day 42)]
Passing Mucus during Bowel Movement
[(a)Day 0 (b) Day 21 and (c) Day 42)]
Abdominal fullness(a)Day 0 (b) Day 21 and (c) Day 42)]
Overall Efficacy-(A) Assessment By Investigators
(B) Assessment By Patients
Comparison of Efficacy of Oxy-Powder® with Dulcolax
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
DETAILED CLINICAL REPORT ON OXYPOWDER CONSTIPATION– IBS:
1.0 DETAILS OF THE FOLLOWING TOPICS HAVE ALREADY BEEN DESCRIBED
ABOVE UNDER "Clinical Report On Oxy-Powder®–Constipation":
Abstract–(Pages 2,3), Synopsis–(Pages 8–14), Glossary– (Pages 90–95), Regulatory Approvals–(Page
96), Investigators Declaration–(Page 97), QA statement– (Page 98),Signature of study Director / study
coordinator–(Page 99), Signature of study Co–coordinator, Monitor, QA Director–(Page 100),
Signature of Statistical Investigator–(Page 101),Contributors to the Study–(Page 102), Introduction–
(Pages103–113), Subject Information and Consent–( Pages114–115)
Since they are common to both clinical trials (constipation and constipation–IBS), these are not
being repeated here.
4.0 Rationale:
The present study was conducted to evaluate effectiveness of Oxypowder in treating IBS with
constipation precipitating loss of weight & improving oxygen delivery in patients of IBS with
4.1 Objective of the study
Primary objective of the present study was to evaluate effectiveness& safety of oxy-powder in
treating IBS with constipation
5.0 METHODOLOGY
5.1 Conduct (including Ethical conduct) of study (Page 114)
5.1.1. Study Design and Duration.
The study was done as Multicentric open randomized comparing safety and effectiveness of
Oxypowder developed by Global Healing Centre Inc. USA with Dulcolax tablets containing 5 mg
Bisacodyl manufactured by Cadila Health Care Ltd. Duration of the study was 6 weeks from the date
of administration of study products.
5.1.2 Subject Information and Consent
5.2 Procedure for Conduct of Study
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
The study was conducted in the out– patient setting in Bhatia Hospital. 20 patients of either sex were
selected for the study. The subjects were included after obtaining their informed consent. Necessary
Regulatory permission from Drug controller General of India was obtained and the study was cleared
by Independent Ethics Committee of Mayfair and Institutional Review Board of Bhatia Hospital
Medical Research Society, Mumbai. The study was conducted in accordance with Current Good
Clinical Practice (GCP) Guidelines.
5.3 Patient Selection
5.4 Subject inclusion
The subjects were included only if the following criteria were met with:
1) Age18 to 60 yrs.
2) Food habits. Both Vegetarians and Non–Vegetarians were included; however, non-vegetarians
3) Acceptable form of birth control was followed in female patients
4) The patients were selected when they satisfied Rome II criteria for IBS (Irritable bowel syndrome)
with constipation. The criteria were as follows:-
(The Rome II diagnostic criterion of irritable Bowel Syndrome always presumes the absence of a
structural or biochemical explanation for the symptoms and is made only by a physician.)
5.4.1 Rome II criteria for IBS
The Rome II diagnostic criteria of Irritable Bowel Syndrome always presumes the absence of a
structural or biochemical explanation for the symptoms and is made only by a physician.
Irritable Bowel Syndrome can be diagnosed based on at least 12 weeks (which need not be
consecutive) in the preceding 12 months, of abdominal discomfort or pain that has two out of three of
these features:
1. Relieved with defecation; and/or
2. Onset associated with a change in frequency of stool; and/or
3. Onset associated with a change in form (appearance) of stool.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
5.4.2 Symptoms that Cumulatively Support the Diagnosis of IBS
1. Abnormal stool frequency (may be defined as greater than 3 bowel movements per day and less
than 3 bowel movements per week);
2. Abnormal stool form (lumpy/hard or loose/watery stool);
3. Abnormal stool passage (straining, urgency, or feeling of incomplete evacuation);
4. Passing of mucus in the faeces.
5. Bloating with abdominal distension.
5.5 Supportive Symptoms of IBS
1. Fewer than three bowel movements a week
2. More than three bowel movements in a day
3. Passing hard or lumpy stools
4. Loose (mushy) or watery stools
5. Straining during a bowel movement
6. Urgency (having to rush to have a bowel movement)
7. Feeling of incomplete bowel movement
8. Passing mucus (white material) during bowel movement
9. Abdominal fullness, bloating, or swelling
5.6 Red Flag symptoms which are NOT typical of IBS
Pain that often awakens/interferes with sleep
Diarrhoea that often awakens/interferes with sleep
Blood in your stool (visible or occult)
Abnormal physical examination
5.7 Diagnosis of IBS
The diagnosis of irritable Bowel Syndrome was based on at least 12 weeks (which need not be
consecutive) in the preceding 12 months of abdominal discomfort or pain that had two out of three of
the following features:
3.Relieved with defecation; and/or
4.Onset associated with a change in frequency of stool; and/or
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
5.Onset associated with a change in form (appearance) of stool.
Since the patients selected were those suffering from IBS with constipation, following symptoms that
supported the diagnosis of IBS with constipation were considered:
1. Abnormal stool frequency – Defined as less than 3 bowel movements per week
2 Abnormal stool form – lumpy/hard stools
3 Abnormal stool passages –
straining During > 25% of Bowel movements
sensation of incomplete evacuation for > 25% of Bowel Movements
sensation of anorectal blockage for > 25% of Bowel movements
manual Manoeuvres to facilitate > 25% of Bowel movements
6.Passage of Mucus during bowel movement.
7.Abdominal fullness or bloating
The patients who had following Red Flag symptoms which are not typical of IBS were excluded
from the study –
Pain that often awakens/interferes with sleep
Blood in your stool (visible or occult)
Abnormal physical examination
5.8 Subject exclusion
Following patients were excluded from the study:
1. Evidence of Malignancy on colonoscopy / having diagnosed organic GI disorder
2. Pregnant and lactating women
3. Evidence of lactose intolerance to explain bowel symptoms
4. History of cardiac arrhythmia's or heart disease
5. History of Glaucoma
6. History of urine retention
7. History of schizophrenia
8. History of substances of abuse/dependency
9. Intellectually unable or unwilling to complete daily GI ratings.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
6.0 Study procedure and Treatment
After selection, the patients were subjected to detailed medical History and clinical examination
Patients then were subjected to following pre–study evaluation :-
Record of weight
Oxygen content of Blood. This was done by using pulse oxcimeter.
Stool examination
Barium meal to rule out any Bowel organic lesion leading to constipation
Colonoscopy to rule out any colonic organic lesion and any faecal impaction.
After ruling out any organic lesion, the patients were included in the study.
7.0 Treatment and Timings
Test Product (A) – Oxy-Powder® capsules marketed by Global Healing Centre, Inc. USA containing
715.5 mg Active in each capsule
Comparative Product (B) – Dulcolax tablets marketed by Cadila Healthcare Ltd, India containing 5
mg Bisacodyl in each tablet.
7.1 DOSAGE & ADMINISTRATION
The patients were divided in two (2) groups as per the Randomization schedule. Group1 was
administered Product A while Group 2 was administered Product B
7.1.1 Test Product (A)
For first time, patients started with a seven-day initial cleansing procedure. After the initial cleanse, a
maintenance dose was continued for keeping intestinal tract clean and deliver oxygen into the system.
Patients were advised to take Oxy-Powder with plenty of potable water during the day and eat healthy
(a) For Cleansing
Patients were directed by the investigators to take four (4) capsules in the evening on an empty
stomach with 240 mL water. If 3-5 bowel movements were not achieved the following day, the
dosage was increased by adding two (2) capsules every night until 3-5 bowel movements were
achieved the following day. The day on which the dosage was finalized was considered as "day one
(1)" of the seven (7) day cleansing cycle. This dosage was continued for seven (7) consecutive days.
After the seven (7) day cleansing cycle, the maintenance dose was started.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
(b) Maintenance Dose:
Patients were given capsules supplies for seven (7) days with instructions that they had be taken as
they did during cleansing cycle. For following 5 weeks, the same dosage was to be repeated by the
patients every other day. They were assured that the capsules were not habit forming or harmful to the
body and could be taken indefinitely.
(c) Comparative Product (B)
Patients in this Group were directed by the investigators to take two tablets of Dulcolax (comparative
formulation) as per the Randomization scheme with plenty of water every day, for first 7 days, in the
evening on empty stomach. Thereafter, the subjects were instructed to take the same dose of Dulcolax
tablets on alternate days on empty stomach in the evening for 6 weeks.
Administration on day ‘0', ‘3 weeks' and ‘6 weeks' was done on empty stomach (to enable measuring
Oxygen levels) in the morning. Subjects were asked to report to the hospital on empty stomach in the
morning for administration of Investigational products and Oxygen level in the blood was measured
15 minutes and 30 minutes after administration of tablets/ capsules.
On the remaining days, the subjects were asked to take same dose of the Investigational product at
their residence in the evening on empty stomach followed by Dinner two hours post-administration of
Administration on day 0, 3 weeks and 6 weeks were done on empty stomach in the morning. Subjects
were asked to report to the hospital in a fasting state in the morning for administration of
investigational products and Oxygen level in the blood were measured 15 minutes and 30 minutes
after administration of tablets/capsules.
On the remaining days, the subjects were instructed to take investigational product at home at the
same dose levels in the evening on empty stomach. They were told to take Dinner at least two hours
post-administration of Drug.
Along with Oxypowder, drinking of large quantity of potable water was recommended. This was not
only healthy for the body but was necessary to aid the body in eliminating toxins from the bowel at a
faster rate. Oxy-Powder works with stomach acid; if the level of HCl is below normal, it may hinder
the effectiveness of the Oxy-Powder, and hence, it was suggested to take an organic lemon wedge
squeezed into glassful of potable water with Oxypowder in the evening.
During the study, prescription medicines were not contraindicated as long as Oxypowder was taken 6
hours before or 6 hours after the medicine. Consumption of Laxatives, anti-diarhoeals and anti-
spasmodics were prohibited during the study.
After starting the study medication, patients, were initially called every day in the morning to check
their daily weight for 7 days.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
After doing the oxygen content on Day 0, all the patients were asked to visit on 3rd wk and 6th wk.
They were called in morning on empty stomach. Group administered "Oxy-Powder®' were
administered capsules and their oxygen levels were determined at '15 min. and '30 min. Post
administration of the dose. In Dulcolax group of patients, since they were comparative group, their
Oxygen levels were measured without administering Dulcolax, '15 min. and ' 30 min. after their
arrival. On 3rd week and 6th week patients were subjected to detailed symptoms to evaluate the effect
of the study drug. Stool analysis was repeated at the end of 6 weeks.
7.2 Study Assessment (Page 118)
7.3 End Points (Page 121)
8.0 Demography
Demographic data including Height, Weight, Age and Sex was collected for all the subjects in
different groups at the time of their inclusion in the study simultaneous to recording of their Medical
History including their Food Habits, Smoking History, Details and Quantity of consumption of
alcoholic drinks and other beverages in a day or frequency thereof and consumption of Tobacco in
other forms or any Drug of Abuse.
As regards the symptom of constipation–IBS, duration of its existence, its severity, No. of Bowels /
Week and type of stools were also recorded.
GRADING OF RESPONSE
The evaluated parameters were compared with those obtained with Dulcolax administered to the
patients belonging to the constipation group.
9.0 Efficacy
a) Overall therapeutic response was graded individually by the investigator with each patient as
‘Excellent', ‘Good', ‘Fair' & ‘Poor'.
b) Therapeutic efficacy was correlated and graded as ‘Complete Cure', ‘Improvement' and
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
10.0 Safety
Severity of each Adverse Event was rated as ‘Mild' (no limitation of usual activity), ‘Moderate'
(some limitation of usual activity), and ‘Severe' (inability to carry out usual activities).
11.0 Withdrawal from Study
There was no withdrawal of patients in either of the treatment in constipation–IBS category. All 20
patients enrolled continued with the study.
12.0 Statistics and data handling
12.1 Statistical Analysis– Derived and Transformed Data
Out of 20 patients enrolled, all 20 patients completed the study & were included in the final analysis.
Their demographic features were compared at baseline using appropriate tests (Student's' test and
Chi-square or Fisher's exact test). Efficacy parameters in two treatment groups were compared by
using Fisher's exact test.
12.2 Data Analysis
12.2.1 Hypotheses
Oxy-Powder® is both, safe and effective in patients with constipation-IBS
12.2.2 Sample Size Consideration
The study design had been examined and approved by a qualified statistician with respect to sample
12.2.3 Primary Comparisons of Interest
Oxy-Powder® is compared for effectiveness in relieving constipation–IBS vis-à-vis Dulcolax tablets
in the same group.
12.2.4 Other Comparisons of Interest
Comparison of safety of Oxy-Powder® has been done vis-à-vis safety achieved post-administering of
Dulcolax tablets.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
12.2.5 Interim Analysis
Data from patients was collected regularly but analyzed at the end of the study for safety and
effectiveness of the Oxy-Powder®.
12.2.6 Analysis Population
After any drop outs, it was assumed to have a minimum of 15 patients (out of 20) in constipation–IBS
group completing the study. Number of patients who actually completed 6 weeks of study was 20.
The population analysis for safety and effectiveness of Oxy-Powder® and Dulcolax has been done for
these 20 patients at the end of the study.
12.2.7 Withdrawal
No patient withdrew from the study until completion of study; all 20 patients have been included in
12.2.8 Missing Data
There has been no Missing data of any patient.
13.0 OTHER ISSUES
Results of Barium Meal test conducted at the commencement of study, pre–administration of
the dose indicated that none of the patients exhibited any signs of organic lesions. In 7 patients
completing the study, no organic lesions were seen in Barium meal test even 6 weeks post– dose
administration at the completion of the study.
In the same 7 patients completing the study (of Oxy-Powder® as well as Dulcolax) , pre–dose
colonoscopy as well as 6 weeks post dose administration colonoscopy studies showed similar findings
in patients under study in having multiple spasmodic contractions in sigmoid and descending colon
but with slight reduction in impacted faecal material shown in post– administration
colonoscopy. This is perhaps one of the factors responsible for efficacy of Oxy-Powder® in the
treatment of constipation with and without IBS. Six weeks period of study was perhaps short to see
greater reduction in impacted faecal material
The investigator recommended that since conduct of these two tests after 6 weeks of completion of
the study did not show any significant differences that could lead to any conclusions, they should be
dropped at the conclusion of the study. However, the patients should continue to be subjected to these
two tests at the commencement of study.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
These recommendations were forwarded to the sponsor by e-mail who gave his consent to follow the
recommendations of the investigator and permitted waiving of conduct of these two tests at the end of
6 weeks period of the study in each of the rest of the patients.
14.0 Ethics
The design of the protocol conformed to the Declaration of Helsinki adopted by the 18th World
Medical Assembly (WMA), Helsinki, Finland (1964) and all amendments. All the patients were
informed of the nature and the purpose of the study and their consent to participate was obtained.
They were also informed of their freedom to withdraw from the study at anytime and at any stage of
the trial. The study was conducted only after the protocol was approved by IEC of MCERC and IRB
of Bhatia General Hospital.Since Oxy-Powder® was marketed in the USA and other countries for
almost a decade with no reported ADR's, and the present study was designed and conducted for
global markets (other than India), the study director prudently and by way of abundant precaution
informed Indian Regulatory Authority, Drugs Controller General of India at CDSCO, New Delhi, of
intention of MCERC to conduct the clinical trial Phase III on Oxy-Powder® in Indian patients.
15.0 Ethical conduct of the study and Ethics Approval
This study was conducted in accordance with "Good Clinical Practice" (GCP) guidelines and all other
applicable regulatory requirements, including WMA's Declaration of Helsinki –VI on Ethical
Principles for Medical Research Involving Human Subjects, as adopted by the 52nd WMA General
Assembly, Edinburgh, October 2000.
The investigator was assigned the responsibility for ensuring that this protocol, the site's informed
consent form, and any other information that will be presented to potential subjects (e.g.
advertisements or information that supports or supplements the informed consent) were reviewed and
approved by the appropriate IEC/IRB. The investigator agreed to allow the IEC / IRB direct access to
all relevant documents. MCERC provided the investigator, IEC and IRB with relevant
document(s)/data that were needed for IEC/IRB review and approval of the protocol for conducting
the study. After receiving copies of the IEC/IRB approval, the investigational product(s), blank copies
of the approved informed consent forms, CRF's and any other information that the IEC/IRB had
approved for presentation to potential subjects. were sent to the trial centre sites, No further
amendments were made in the above formats by IEC/IRB
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
15.1 Informed Consent
Informed consent was obtained from each participant before the subject was permitted to participate
in the study. The contents and process of obtaining informed consent was in accordance with all
applicable regulatory requirements.
16.0 Protocol Compliance
There were two deviations in the protocol.
1) Age of the patients for enrollment was raised to 65 years to include geriatric patients in whom
constipation is more prevalent. There was shortage of patients suffering from constipation in the age
group specified in the protocol.
Permission from the sponsor was obtained to include patients suffering from constipation up to the
age of 65 years.
2) During course of the study, both the investigators independently made following observation:
a) Pre– and post–colonoscopy showed multiple spasmodic contractions in sigmoid and descending
colon with large amount of fecal impaction in entire colon.
b) In Barium meal test, no organic lesions were seen before and after Barium meal administration.
These observations were made in case of type1and type 2 patients.
Both the investigators recommended that in view of these observations, post-colonoscopy and post–
administration of Barium meal should not be done since they do not significantly contribute to the
results of the study. Instead, they were causing discomfort discouraging the patients from continuing
with the treatment. They recommended that both the tests must be done at the time of enrolling the
These recommendations were forwarded to the sponsor who, while agreeing with the suggestions of
the investigators, permitted to waive conduct of post–colonoscopy as well as post administration of
17.0 Handling and Storage of Investigational Product
Investigational products were dispensed and administered according to procedures described herein.
Only subjects enrolled in the study received investigational product, in accordance with all applicable
regulatory requirements. Only authorized site staff supplied and administered investigational
products. All investigational products were stored in a secured area with access limited to the
investigator and authorized site staff and under physical conditions that are consistent with
investigational product's specific requirements.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
17.1 Product Accountability
The investigator is responsible for investigational product accountability, reconciliation, and record
maintenance. In accordance with all applicable regulatory requirements, the investigator and the
designated site staff maintained investigational product accountability records throughout the course
of the study. The authorized person(s) documented the amount of investigational product received
from MCERC, the amount supplied and administered to the subjects.
18.0 Assessment of Compliance
A diary card was given to the patients during the entire course of the clinical trial which will record
the number of capsules/ tablets taken and number of stools passed. Diary card was issued at day 0,
week 3 and week 6 after collecting the previously completed diary filled every day from the
concerned patient. Patient was required to contact his physician in the event of any difficulties /
queries the patient had.
18.1 Screen and Baseline Failures
Not applicable since the study is non-invasive
19.0 Study Monitoring
In accordance with applicable regulations, GCP guidelines and MCERC procedures, MCERC
monitors contacted the site prior to the subject enrollment to review the protocol and data collection
procedures with site staff. In addition, the monitor periodically contacted the site, including
conducting on-site visits. The extent, nature and frequency of on-site visits were based on such
considerations as the study objective and/or endpoints, the purpose of the study, study design
complexity, and enrollment rate.
During these contacts, the monitor
Checked the progress of the study.
Reviewed study data collected.
Conducted source document verification.
Identified any issues and address their resolution.
This was done in order to verify that the:
Data was authentic, accurate, and complete.
Safety and rights of subjects were being protected.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Study was conducted in accordance with the currently approved protocol (and any amendments),
GCP guidelines, and all applicable regulatory requirements.
The investigators agreed to allow the monitor direct access to all relevant documents and to allocate
his/her time and the time of his/her staff to the monitor to discuss findings and any relevant issues.
At study closure, monitors conducted all activities described in Section, "Study and Site Closure."
The monitor also reviewed subject-completed health outcomes questionnaire(s) for extraneous written
comments that could indicate possible AEs. Information collected in the CRF and in the subject-
completed health outcomes questionnaire(s) are independent components of this study. Except for
header section information (e.g., subject number, treatment number, and visit date) and other
information as defined in the standard clarification agreement (SCA), neither the monitor nor the
investigator attempted to reconcile responses to individual questions/items recorded on the subject-
completed health outcomes questionnaire(s) or health outcomes portions of diary cards with other data
recorded in the CRF's. Subject-completed health outcome questionnaires generally serve as the source
document; therefore, unless otherwise specified elsewhere, no other source document is available for
data validation.
20.0 Quality Assurance
To ensure compliance with GCP guidelines and all applicable regulatory requirements, MCERC
regularly conducted Quality Assurance audit. It was open to Regulatory agencies to conduct
regulatory inspection of this study at any time during or after completion of the study. The
investigator and institution agreed to allow the auditor/inspector direct access to all relevant
documents and to allocate his/her time and the time of his/her staff to the auditor/inspector to discuss
findings and any relevant issues.
21.0 Study and Site Closure
Upon completion of the study, the monitor conducted the following activities in conjunction with the
investigator or site staff, as appropriate:
Return of all study data to MCERC Data queries.
Accountability, reconciliation, and arrangements for unused investigational product(s).
Review of site study records for completeness.
Return of treatment codes to MCERC
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
22.0 Data Management
Subject data was collected by the investigators or designees using the Case Report Form (CRF)
framed by MCERC in consultation with the sponsor and the investigators. Subject data necessary for
analysis and reporting was entered into a validated database Clinical data management was performed
in accordance with the ‘applicable MCERC standards' and data cleaning procedures. Original CRF's
are retained by MCERC.
23.0 Statistical analysis
The data generated on the subjects was classified in different forms to obtain meaningful results on
statistical analysis. Three different types of tables supplied to the statistician included:
T1–subject wise medical history including history of a) surgery undergone,
b) illness, c) medication, duration of constipation and IBS if applicable and its severity
T2–Baseline data including subject number and code, subject's age, sex, weight, food habits, smoking
T3– subject wise clinical investigations (Oxygen content of the blood, stool examination at 0 and 42
weeks, Efficacy evaluation
by the investigators and side effects experienced, if any
The results were statistically analyzed using SAS statistical software.
24.0 Records Retention
Following closure of the study, the investigators maintained all site study records in a safe and
secure location. The records were maintained to allow easy and timely retrieval, when needed (e.g.
audit or inspection), and, whenever feasible, to allow any subsequent review of data in conjunction
with assessment of the facility, supporting systems, and staff. Where permitted by local
laws/regulations or institutional policy, some or all of these records were maintained in a format other
than hard copy in an electronic form. The investigator also assured that all reproductions were legible,
were a true and accurate copy of the original and met accessibility and retrieval standards, including
re-generating a hard copy, when required. Furthermore, the investigator also ensured that there was an
acceptable backup of these reproductions and that an acceptable quality control process existed for
making these reproductions.
MCERC informed the investigators of the time period for retaining these records to comply with all
applicable regulatory requirements. The minimum retention time would meet the strictest standards
applicable to that site for the study, as dictated by any institutional requirements or local laws or
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
regulations, or MCERC standards/procedures which shall not exceed 1year from the date of
submission of the report
25.0 Provision of Study Results and Information to Investigators
After the completion of the clinical study report, Study Director of MCERC provided copy of the
same to the investigators along with the details of the study treatment assignment to enable them to
review the data to determine the outcome of the study for the benefit of their subjects.
. The investigator and the study staff were directed to hold the information confidentially
26.0 Information disclosure and inventions
26.1 Ownership
All information provided by MCERC and all data and information generated by the site as parts of the
study (other than a subject's medical records) are the sole property of MCERC
All rights, title, and interests in any inventions, know-how or other intellectual or industrial property
rights which are conceived or reduced to practice by site staff during the course of or as a result of the
study are the sole property of MCERC, and are hereby assigned to MCERC.
26.2 Confidentiality
All information provided by MCERC and all data and information generated by the site as part of the
study (other than a subject's medical records) have been kept confidential by the investigators and
other site staff. This information and data will not be used by the investigators or other site personnel
for any purpose other than conducting the study. These restrictions do not apply to:
(1) Information which becomes publicly available through no fault of the investigator or site staff;
(2) Information which it is necessary to disclose in confidence to an IEC or IRB solely for the
evaluation of the study;
(3) Information which it is necessary to disclose in order to provide appropriate medical care to a
study subject; or
(4) Study results which may be published as described in the next paragraph.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
26.3 Publication
For Multicentric studies, the first publication or disclosure of study results shall be a complete, joint
Multicentric publication or disclosure coordinated by MCERC Thereafter, any secondary publications
will cite reference the original publication(s).
Prior to submitting for publication, presentation, use for instructional purposes, or otherwise
disclosing the study results generated by the site (collectively, a "Publication"), the investigators shall
provide MCERC with a copy of the proposed Publication and allow MCERC a period of at least thirty
(30) days. The proposed Publications shall not include either MCERC's confidential information
other than the study results or personal data of any subject, such as name or initials.
At MCERC's request, the submission or other disclosure of a proposed Publication will be delayed
for a sufficient time to allow MCERC to seek patent or similar protection of any inventions, know-
how or other intellectual or industrial property rights disclosed in the proposed Publication.
If a written contract for the conduct of the study, which includes publication provisions inconsistent
with this statement is executed, that contract's publication provisions shall apply rather than this
It is mandatory to inform and register with the Association of publishers of Medical General, the
Clinical trial details, before commencement of the study.
[Ref: The International Committee of Medical Journal Editors (ICMJE) Policy dtd. May 23, 2004].
20.0 RESULTS
(a) DESCRIPTIVE
(i) Demography:
The baseline demographic characteristics of patients were similar in two treatment groups of the study
(P> .05). Summary of patient's characteristics including sex, age & weight is presented in Table 18
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table18–Demographic Characteristics
Drug & No. of
Mean Age ( yrs )
Mean Wt. ( kg. )
Patients
Male Female Max Min.
(ii) Patients living style
The food habits of the patients are given in Table 19. Both Non-Vegetarian and Vegetarian patients
were included in the study.
Table -19 – Food Habits.
Drug
Non veg (%)
Veg. (%)
SMOKING:
In both groups, some patients were smokers – Table 20.
Table20– Smoking History
Drug Yes
No
MEDICAL HISTORY:
According to Rome II criteria for IBS, all patients selected was suffering from IBS along with
constipation for 12 weeks (3 months) or more. They were grouped as follows – Tables 21-23.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table 21– Duration of constipation in months (As per Groups)
Groups A
B
3 months – 12 months
12 months – 24 months
Table 22 – Number of bowels in a week (As per Groups)
Groups A
B
Table 23–Severity of Constipation.
Severity A
B
(P >.05).
All above groups were statistically compared by using appropriate tests & there was no statistically
significant difference between the two groups indicating they were comparable at the base line values
All the patients were checked for their daily weight for 7 days (0 + 6 days) & then on 3rd week & 6th
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
(IV) Study Medication
The randomization of the patients was done as 2:1 i.e. 2 patients were given Oxypowder & 1 patient
was given Dulcolax. Out of 20 patients, 13 patients received Oxypowder (A) & 7 patients received
Dulcolax (B). Their disposition for the study is presented in Table 24.
Table 24 – Randomization
(V) Non–Study Medication:
None of the patients received any medication other than the Test or the Reference formulation.
(VI) Patient Withdrawal
No patient withdrew from the study until completion of study; all 20 patients have been included in the
All the patients were checked for their daily weight for 7 days (0 + 6 days) & then on 3rd week & 6th
Table 25 shows comparison of their weights From Day 0 to day 42.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table 25 – Comparison of weight (kg) (Day 0 – Day 42)
Drug
No
Mean ( S.D.)
Table 26 – Number of Bowels in a week (grouped)
Day 0
Day 21
Day 42
As seen from Table 26 all patients in both groups, had increase in the frequency of stool after 42 days
Oxypowder releases nascent oxygen for its action and the objective of the study was to seen whether
Oxypowder increases oxygen saturation of blood. As seen from Table 27, there was marginal increase
in oxygen delivery after taking Oxypowder for 6 weeks (42 days) as compared to Day 0
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table 27– Oxygen content of blood (Day 0, Day 21, and Day 42)
Drug No
Mean (∀S.D)
Oxygen Content of Blood Day 0
Oxygen Content of Blood Day 21 after 15 Min.
Oxygen Content of Blood Day 21 after 30 Min.
Oxygen Content of Blood Day 42 after 15 Min.
Oxygen Content of Blood Day 42 after 30 Min.
Oxygen Content of Blood Day 0
Oxygen Content of Blood Day 21 after 15 Min.
Oxygen Content of Blood Day 21 after 30 Min.
Oxygen Content of Blood Day42 after 15 Min.
Oxygen Content of Blood Day42 after 30 Min.
Since all the patients of IBS had constipation, various symptoms of constipation were compared on 3
week and 6 week to their baseline values (day 0)
Tables 28, 29, 30, 31, 32 show that their is significant reduction in all the symptoms in both groups
Table 28–(a) Straining During >25% of Bowel Movement (Day 0)
Drug
No. of patients (%)
(b)Straining During > 25% of Bowel Movement (Day 21).
Drug
No. of patients (%)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Drug
No. of patients (%)
(c) Straining During > 25% of Bowel Movement (Day 42).
Drug
No. of patients
Table29 (a)– Lumpy Stools (Day 0).
Drug
No. of patients
Lumpy Stools (b) (Day 21).
Drug
No. of patients
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Lumpy Stools (c) (Day 42).
Drug
No. of patients
Table30–(a) Sensation of incomplete evacuation for >25% of Bowel movement (Day 0).
Drug
No. of patients
(b)Sensation of incomplete evacuation for >25% of Bowel movement (Day21).
Drug
No. of patients ( % )
(c) Sensation of incomplete evacuation for >25% of Bowel movement (Day 42).
Drug
No. of patients ( % )
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Drug
No. of patients ( % )
Table 31–(a) Sensation of Anorectal Blockage for >25% of Bowel Movement (Day 0).
Drug
No. of patients ( % )
(b)Sensation of Anorectal Blockage for >25% of Bowel Movement (Day 21).
Drug
No. of patients ( % )
(c)Sensation of Anorectal Blockage for >25% of Bowel Movement (Day 42).
Drug
No. of patients ( % )
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table 32–(a) Manual Manoeuvres to facilitate >25% of Bowel Movements (Day 0).
Drug
No. of patients
(b) Manual Manoeuvres to facilitate >25% of Bowel Movements (Day 21).
Drug
No. of patients
(c) Manual Manoeuvres to facilitate >25% of Bowel Movements (Day 42).
Drug
No. of patients
As seen from Table 28 in group A all 13 patients had straining on Day 0 as compared to this on Day
42 only 1 (7.7%) patient had these symptoms.
Similarly in Table 29, in group A 12 patients ( 92.3% ) passed hard, and lumpy stools on Day 0 where
as on day 42 none of the patients had this symptoms Table 30, 31 & 32 also show significant
reduction in symptoms in both groups ( P < .05 )
Effect of Oxypowder was evaluated on typical symptoms of IBS with constipation. i.e.
1.Abdominal discomfort or pain
Relieved with defecation – Table (33)
Onset associated with a change in frequency of stool – (Table 34)
Onset associated with change in form of stool – (Table 35)
2.Passing mucus during bowel movement – ( Table 36 )
3.Abdominal Fullness ( Table 37 )
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table 33–(a) ABDOMINAL PAIN RELIEVED WITH DEFECATION (DAY 0)
Drug
No. of patients ( % )
(b)ABDOMINAL PAIN RELIEVED WITH DEFECATION (DAY 21)
Drug
No. of patients ( % )
(c)ABDOMINAL PAIN RELIEVED WITH DEFECATION (DAY 42)
Drug
No. of patients ( % )
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table 34–(a) ABDOMINAL PAIN ONSET ASSOCIATED WITH A CHANGE IN
FREQUENCY OF STOOLS (DAY 0)
Drug
No. of patients ( % )
(b) ABDOMINAL PAIN ONSET ASSOCIATED WITH A CHANGE IN FREQUENCY OF
STOOLS (DAY 21)
Drug
No. of patients ( % )
(c) ABDOMINAL PAIN ONSET ASSOCIATED WITH A CHANGE IN FREQUENCY OF
STOOLS (DAY 42)
Drug
No. of patients ( % )
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table35–(a) ABDOMINAL PAIN ONSET ASSOCIATED WITH A CHANGE IN FORM OF
STOOLS (DAY 0)
Drug
No. of patients ( % )
(b) ABDOMINAL PAIN ONSET ASSOCIATED WITH A CHANGE IN FORM OF STOOLS
Drug
No. of patients ( % )
(c) ABDOMINAL PAIN ONSET ASSOCIATED WITH A CHANGE IN FORM OF STOOLS
Drug
No. of patients ( % )
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table36– (a) PASSING MUCUS DURING BOWEL MOVEMENT (DAY 0)
Drug
No. of patients ( % )
(b) PASSING MUCUS DURING BOWEL MOVEMENT (DAY 21)
Drug
No. of patients ( % )
(c)PASSING MUCUS DURING BOWEL MOVEMENT (DAY 42)
Drug
No. of patients ( % )
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Table37–(a) ABDOMINAL FULLNESS (DAY 0)
Drug
No. of patients ( % )
(b) ABDOMINAL FULLNESS (DAY 21)
Drug
No. of patients ( % )
(c) ABDOMINAL FULLNESS (DAY 42)
Drug
No. of patients ( % )
As seen from Table 33, 34 and 35 there was significant reduction in Abdominal pain after the
treatment in both groups.
As seen from Table 37, in group A 11 patients ( 84.6% ) had abdominal fullness on Day 0, where as
on Day 42, only 1 ( 7.7% ) patient had this symptom indicating significant reduction ( P < .05 )
All above the parameters indicate that Oxypowder significantly reduced the symptoms of IBS with
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
Routine Stool Examination was done before and after the drug treatment, which was normal in all 20
Efficacy was independently judged by the Investigator & patient and it was rated as excellent, Good,
Fair and Poor. It was statistically analysed using Fisher's Exact Test
Table 38– EFFICACY TABLES
(A) ASSESSMENT BY INVESTIGATOR
Efficacy Grade
DRUG
A B
(P < 0.05)
(B) ASSESSMENT BY PATIENTS
Efficacy Grade
DRUG
A B
(P < 0.05)
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
In group A out of 13 completed patients investigator assessment was excellent for 6 ( 46.2% ) Good
for 5(38.5% ) Fair for 2 ( 15.4% ), where as in group B out of 7 patients it was Good for 3 ( 42.9% ),
Fair for 2 ( 28.6% ) and poor for 2 (28.6% ).
Efficacy of Oxypowder in treating IBS with constipation was significantly (P<.05) more than
Dulcolax and hence this indicates Oxypowder was more efficacious in treating IBS with constipation
Table 39–Overall Efficacy
EFFICACY
Overall efficacy was also judged as complete cure, Improvement and Failure. Table 39 shows that in
group A, out of 13 patients 4 patients ( 30.8% ) had complete cure, 9 patients ( 69.2% ) had
improvement and there was no failure where as in group B out of 7 patients, none of the patients had
complete cure, 5 patients ( 71.4% ) had improvement and 2 patients ( 28.6% ) had failure
Above Table indicates efficacy of Oxypowder is significantly more (P < .05) than Dulcolax in treating
patients of IBS with constipation.
Regarding Adverse events, none of the patients had any adverse events during the study period.
DISCUSSION AND SUMMARY
SUMMARY:
The present study titled
"Multicentric Randomized, Open, Comparative study to evaluate the safety and efficacy of Oxy-
Powder® in patients of chronic constipation and IBS" was conducted to evaluate effectiveness of
Oxypowder in treating constipation and IBS with constipation precipitating loss of weight &
improving oxygen delivery in patients of constipation and IBS with constipation The study was
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
sponsored by Dr. Edward Group III, CEO, Global Healing Center, Inc. & contracted to Mayfair
Clinical, Education & Research Centre (MCERC), a Clinical Research Organisation (CRO) for
conduct of the study.
For evaluating effectiveness of Oxy-Powder® in patients of constipation, the study was conducted in
Bhatia General Hospital located in Mumbai. However, for evaluating effectiveness of Oxy-Powder®
in patients of IBS with constipation, the study was conducted in Bhatia General Hospital. The Study
Protocol was carefully designed and got approved from the sponsor by MCERC. The respective
investigators were Dr. Chetan Bhatt and Dr. Sharad Shah.
The study commenced after MCERC obtained approvals from IEC of MCERC, IRB of Bhatia
Hospital and other Regulatory authorities. The study proposed to enrol 60 patients according to
inclusion and exclusion criteria given in the protocol but ultimately culminated with 40 patients (one
patient out of these had ADR and withdrew from the study from 3rd day). The randomization of the
patients was done as 2:1 i.e. 2 patients were given Oxypowder & 1 patient was given Dulcolax, the
comparative product. Thus, there were 13 patients in Oxy-Powder® group and 7 patients in Dulcolax
group. All the patients were counselled before enrolment and their "Informed Consent" was taken.
Their Medical History was recorded by the investigators They were subjected to clinical examination
and pre-study evaluation including recording of weight, oxygen content of blood using pulse
oxcimeter, stool examination, Barium meal (to rule out any Bowel organic lesion leading to
constipation) and colonoscopy (to rule out any colonic organic lesion and any faecal impaction).
Duration of the trial was 42 days i.e. 6 weeks out of which the first week administration of the
treatment products was for bowel cleansing followed by 5 weeks of maintenance. The patients were
instructed to take four capsules of Oxy-Powder® (Test formulation) or two tablets of Dulcolax
(Comparative formulation), as per the Randomization scheme, with plenty of water every day for first
7 days, in the evening on empty stomach. Thereafter, subjects were instructed to take the same dose of
either test of reference formulation on alternate days, on empty stomach, in the evening, for period of
Administration on day '0', '3 weeks' and ' 6 weeks' were done on empty stomach in the morning.
Subjects were asked to report to the hospital with empty stomach in the morning for administration of
investigational products and Oxygen level in the blood were measured 15 minutes and 30 minutes
after administration of tablets/capsules.
On the remaining days, the subjects were instructed to take investigational product at home at the
same dose levels in the evening on empty stomach. They were told to take Dinner at least two hours
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
post-administration of Drug. Patients were emphatically told to report to the investigators any
ADR's that they experience during or after the study.
DISCUSSION OF THE RESULTS:
The Demographic Characteristics recorded in Table-1 indicate that among 27 patients enrolled in
Oxy-Powder® (OP) group, there were 19 male patients (70.4%) and 8 female patients (29.6%) while
in 13 patients in Dulcolax group (DL), there were 8 male patients (61.5%) and 5 female patients
(38.5%).They conformed to the age and the weight as given in the protocol. 13(48.1%) in OP group
were non-vegetarians and 14 (51.9%) were vegetarians as compared to 7(53.8%) non-vegetarians and
6(46.2%) vegetarians in DL group. Majority of patients in both the groups were non-smokers.
MEDICAL HISTORY: Their medical history indicated that in OP group, among the patients
enrolled,13 (48.1%) patients suffered from constipation problem for a period ranging between 3
months to 12 months, 6 (22.2%) between 12 months to 24 months and 8 (29.6%) for more than 24
months. In DL group, 6 (46.2%) patients suffered from constipation problem for a period ranging
between 3 months to 12 months, 4 ( 30.8% ) between 12 months to 24 months and 3 ( 23.1% ) for
more than 24 months.
These and the above figures indicate that enrolment was in full conformance with the
requirements of the protocol.
As regards the severity of constipation based on number of bowels in a week, in OP group, 9(33.3%)
patients suffered from Severe constipation, 17(63.0%) from Moderate constipation and 1(3.7%)
from Mild constipation,
In DL group, 5(38.5%) patients suffered from Severe constipation, 8(61.5%) from Moderate
constipation and none from Mild constipation,
IN OTHER WORDS, THE TWO GROUPS OF PATIENTS ENROLLED WERE EVENLY
BALANCED WITH RESPECT TO SEVERITY OF CONSTIPATION.
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
POST ADMINISTRATION CHANGES:
As seen from the results recorded in Table 8, there is no reduction in the weight of the patients in OP
group after 42 days of administration of Oxy-Powder® as compared to
Base line (0 day) indicating that administration of Oxypowder did not lead to reduction of weight in
the patients. Similarly, there was no reduction in the weight in Dulcolax group. In both the groups,
after starting the investigating drug; frequency of stools (No. of Bowels in a week) increased as is
shown by the results recorded in Table 9. Comparing the two groups, the percentage performance of
Oxy-Powder® was better than Dulcolax on the 21st and the 42nd Day.
As stated in the "Introduction", Oxypowder releases nascent oxygen for its action; the objective of
this study was to see whether Oxypowder increases oxygen saturation of blood. As seen from Table
10, there was marginal increase in oxygen delivery after taking Oxypowder for 6 weeks (42 days) as
compared to Day 0. It thus appears that the study period was little short and should have been
extended approximately to 180 days to get more conclusive results.
During the study, the patients in both the groups showed significant reduction in various symptoms as
shown in Tables 11, 12, 13, 14, 15 (Straining During >25% of Bowel Movement during 0-42 days,
Lumpy Stools during 0-42 days, Sensation of incomplete evacuation for >25% of Bowel movement
during 0-42 days, Sensation of Anorectal Blockage for >25% of Bowel Movement during 0-42 days
and Manual Manoeuvres to facilitate >25% of Bowel Movements during 0-42 days). As can be seen
from the results in Table 11 in Oxypowder group, 25 patients (92.6%) had straining on Day 0 as
compared to only 2 (7.7%) patients on Day 42. Similarly, in Table 12, in the same group, 26 patients
96.3%) passed hard and lumpy stools on Day 0 where as on day 42, it was reduced only to two
patients (7.7%). The above parameters indicate that there is significant reduction in the symptoms
(P<05) in both groups. However, In this case also, the results were better in case of Oxypowder as
compared to Dulcolax Routine stool examination done before and after the drug treatment showed no
abnormality in all 40 patients in this study
MAYFAIR CLINICAL EDUCATION & RESEARCH CENTRE,
Mohan Mill Compound, Ghodbunder Road, Thane-400 607.
Document No MCERC/REPTCLTR/OXY/1205/001 Study Identifier: Mfair/oxy/200506
EFFICACY JUDGED:
Efficacy was independently judged by the Investigators & the patients. It was graded as excellent,
Good, Fair and Poor. The results were statistically analysed using Fisher's Exact Test. In Oxypowder
group, out of 26 completed patients, investigator assessment was excellent for 13 (50%) Good for
12(46.2%) Fair for 1 (3.8%), where as in Dulcolax group, out of 13 patients, it was excellent for 1
(7.7%) Good for 6 (46.2%), Fair for 4 (30.8%) and poor for 2 (15.4%).
Overall efficacy was also judged as complete cure, Improvement and Failure. Table 17 shows that in
Oxypowder group , out of 26 patients, 11 patients ( 42.3% ) had complete cure, 15 patients ( 57.7% )
had improvement and there was no failure where as in Dulcolax group, out of 13 patients, 1 patient (
7.7% ) had complete cure, 10 patients ( 76.9% ) had improvement and 2 patients ( 15.9% )
experienced failure.
CONCLUSION:
Efficacy of Oxypowder in treating constipation was significantly (P<.05) higher than Dulcolax thus
indicating that Oxypowder was more efficacious in treating constipation than Dulcolax.
No adverse event was reported other than one patient in Op group withdrawing from the study
right in the beginning. Oxy-Powder® was well tolerated by all the patients under treatment of
this product.
––––– THE END OF REPORT ––––
Source: https://www.oxypowder.net/pdf/oxypowder-clinical-trials.pdf
Jv129910289p
JOURNAL OF VIROLOGY, Dec. 1999, p. 10289–10295 Copyright © 1999, American Society for Microbiology. All Rights Reserved. Effect of Lamivudine on Human T-Cell Leukemia Virus Type 1 (HTLV-1) DNA Copy Number, T-Cell Phenotype, and Anti-Tax Cytotoxic T-Cell Frequency in Patients with HTLV-1-Associated Myelopathy G. P. TAYLOR,1* S. E. HALL,2 S. NAVARRETE,2 C. A. MICHIE,3 R. DAVIS,1 A. D. WITKOVER,2 M. ROSSOR,4
natchez.ms.us
SPECIAL CALL MEETING January 4, 2016 A Special Call Meeting of the Mayor and Board of Aldermen of the City of Natchez, Mississippi, was held in the Council Chambers at 4:00 p.m. on Monday, January 4, 2016. Mayor Pro Tempore Arceneaux-Mathis presided at the meeting. Elected Officials City Officials & Present Absent Department Larry L. Brown Donnie Holloway, City ClerkMayor Hyde Carby, City Attorney