Mecriticalcare.net

Recommendations for the diagnosis and management of corticosteroid
insufficiency in critically ill adult patients: Consensus statements from an
international task force by the American College of Critical Care Medicine
Paul E. Marik, MD, FCCM; Stephen M. Pastores, MD, FCCM; Djillali Annane, MD; G. Umberto Meduri, MD;Charles L. Sprung, MD, FCCM; Wiebke Arlt, MD; Didier Keh, MD; Josef Briegel, MD;Albertus Beishuizen, MD; Ioanna Dimopoulou, MD; Stylianos Tsagarakis, MD, PhD; Mervyn Singer, MD;George P. Chrousos, MD; Gary Zaloga, MD, FCCM; Faran Bokhari, MD, FACS; Michael Vogeser, MD
Objective: To develop consensus statements for the diagnosis and
hormone (250 g) administration or a random total cortisol of <10 g/dL. The
management of corticosteroid insufficiency in critically ill adult patients.
benefit of treatment with glucocorticoids at this time seems to be limited to patients
Participants: A multidisciplinary, multispecialty task force of experts in
with vasopressor-dependent septic shock and patients with early severe acute
critical care medicine was convened from the membership of the Society of
respiratory distress syndrome (PaO /F
of <200 and within 14 days of onset). The
Critical Care Medicine and the European Society of Intensive Care Medicine.
adrenocorticotrophic hormone stimulation test should not be used to identify those
In addition, international experts in endocrinology were invited to partici-
patients with septic shock or acute respiratory distress syndrome who should
receive glucocorticoids. Hydrocortisone in a dose of 200 mg/day in four divided
Design/Methods: The task force members reviewed published literature
doses or as a continuous infusion in a dose of 240 mg/day (10 mg/hr) for >7 days
and provided expert opinion from which the consensus was derived. The
is recommended for septic shock. Methylprednisolone in a dose of 1
consensus statements were developed using a modified Delphi methodology.
mg·kgⴚ1·dayⴚ1 for >14 days is recommended in patients with severe early acute
The strength of each recommendation was quantified using the Modified
respiratory distress syndrome. Glucocorticoids should be weaned and not stopped
GRADE system, which classifies recommendations as strong (grade 1) or weak
abruptly. Reinstitution of treatment should be considered with recurrence of signs
(grade 2) and the quality of evidence as high (grade A), moderate (grade B), or
of sepsis, hypotension, or worsening oxygenation. Dexamethasone is not recom-
low (grade C) based on factors that include the study design, the consistency
mended to treat critical illness–related corticosteroid insufficiency. The role of
of the results, and the directness of the evidence.
glucocorticoids in the management of patients with community-acquired pneumo-
Results: The task force coined the term critical illness–related corticosteroid
nia, liver failure, pancreatitis, those undergoing cardiac surgery, and other groups
insufficiency to describe the dysfunction of the hypothalamic-pituitary-adrenal axis
of critically ill patients requires further investigation.
that occurs during critical illness. Critical illness–related corticosteroid insufficiency
Conclusion: Evidence-linked consensus statements with regard to the
is caused by adrenal insufficiency together with tissue corticosteroid resistance and
diagnosis and management of corticosteroid deficiency in critically ill
is characterized by an exaggerated and protracted proinflammatory response.
patients have been developed by a multidisciplinary, multispecialty task
Critical illness–related corticosteroid insufficiency should be suspected in hypoten-
force. (Crit Care Med 2008; 36:1937–1949)
sive patients who have responded poorly to fluids and vasopressor agents, partic-
KEY WORDS: corticosteroid; glucocorticoid; insufficiency; deficiency; adult;
ularly in the setting of sepsis. At this time, the diagnosis of tissue corticosteroid
adrenal glands; diagnosis; management; consensus statement; guidelines; Del-
resistance remains problematic. Adrenal insufficiency in critically ill patients is best
phi methodology; evidence-based medicine; sepsis; cortisol; critical care; in-
made by a delta total serum cortisol of <9 g/dL after adrenocorticotrophic
tensive care units; intensive care; shock septic; surgery; stress dosing
*See also p. 1987.
Stronger Hospital of Cook County, Chicago, IL (FB); Hospital
cine, the European Critical Care Research Network, the
From the Division of Pulmonary and Critical Care Med-
of the University of Munich, Institute of Clinical Chemistry,
International Sepsis Forum, and the Gorham Foundation. Dr.
icine, Thomas Jefferson University, Philadelphia, PA (PEM);
Munich, Germany (MV).
Annane has received grant support from the French Ministry
Critical Care Medicine Fellowship Program, Memorial Sloan-
The American College of Critical Care Medicine (ACCM),
of Health for the prognostic value of a adrenocorticotrophic
Kettering Cancer Center, New York, NY (SMP); Critical Care
which honors individuals for their achievements and contri-
hormone test in septic shock; the French multicenter, ran-
Department, Universite de Versailes Saint-Quentin en Yve-
butions to multidisciplinary critical care medicine, is the
domized, controlled trial on hydrocortisone plus fludrocorti-
lines, Hospital Raymond Poincare, Garches, France (DA);
consultative body of the Society of Critical Care Medi-
sone in septic shock; the ongoing French multicenter 2 ⫻ 2
Division of Pulmonary and Critical Care Medicine, University
cine (SCCM) that possesses recognized expertise in
factorial study that compares strict glucose control vs. con-
of Tennessee HSC, Memphis, TN (GUM); Department of
the practice of critical care. The College has developed
ventional treatment for steroid-treated septic shock and hy-
Anesthesiology, Hadassah Hebrew University Medical Cen-
administrative guidelines and clinical practice parameters for
drocortisone alone vs. hydrocortisone and fludrocortisone;
ter, Jerusalem, Israel (CLS); Division of Medical Sciences,
the critical care practitioner. New guidelines and practice
and a French multicenter 2 ⫻ 2 factorial trial that compares
Institute of Biomedical Research, Endocrinology & Metabo-
parameters are continually developed, and current ones are
lism, The Medical School, University of Birmingham, Bir-
systematically reviewed and revised.
hydrocortisone plus fludrocortisone, activated protein C, the
mingham, UK (WA); Department of Anesthesiology and In-
Dr. Marik has received lecture fees from Eli Lilly and
combination of the two drugs, and placebos for the treatment
tensive Care Medicine, Campus Virchow-Clinic, Humboldt
Merck. Dr. Keh has received grant support from the German
of septic shock. Dr. Pastores has received grant support form
University, Berlin, Germany (DK); Department of Anesthesi-
Research Foundation and German Ministry of Education and
Eisai Medical Research (phase 3 trial of E5564 in severe
ology, University of Munich, Klinikum Grosshadern, Munich,
Research (HYPRESS: Hydrocortisone for Prevention of Septic
sepsis), and Artisan Pharma (phase 2 sepsis with dissemi-
Germany (JB); Department of Intensive Care, VU University
Shock). Dr. Sprung has been a member of a data monitoring
nated intravascular coagulation trial). The remaining authors
Medical Center, Amsterdam, Netherlands (AB); Department
and safety committee for Artisan Pharma, Novartis Corpora-
have not disclosed any conflicts of interest with respect to
of Critical Care Medicine, Athens University, Medical School,
tion, and Hutchinson Technology Incorporated. He has
this article.
Athens, Greece (ID); Department of Endocrinology, Athens'
served as a consultant for AstraZeneca, Eisai Corporation, Eli
For information regarding this article, E-mail:
Polyclinic, Athens, Greece (ST); Department of Medicine and
Lilly, and GlaxoSmithKline. He has received grant support
Wolfson Institute of Biomedical Research, University College
from the European Commission, Takeda, and Eisai Corpora-
Copyright 2008 by the Society of Critical Care
London, Jules Thorn Building, Middlesex Hospital, London,
tion. He has received lecture fees from Eli Lilly. Drs. Sprung,
Medicine and Lippincott Williams & Wilkins
UK (MS); First Department of Pediatrics, Athens University
Annane, Keh, Singer, and Briegel were investigators in the
Medical School, Athens, Greece (GPC); Baxter Healthcare,
CORTICUS study, which was supported by the European
Clintec Nutrition, Deerfield, IL (GZ); Department of Trauma,
Commission, the European Society of Intensive Care Medi-
Crit Care Med 2008 Vol. 36, No. 6

activate the hypothalamic-pitu-
majority is reached. This approach has
tory distress syndrome (ARDS) who re-
itary-adrenal (HPA) axis and
several distinct advantages. It allows the
ceived either moderate-dose corticoste-
stimulate the release of adreno-
inclusion of a large number of individuals
roid or placebo was performed. Four of
corticotrophic hormone (ACTH) from the
across diverse geographic locations and
the task force members (P. E. Marik, D.
pituitary, which in turn increases the re-
with a broad range of expertise. One of its
Annane, S. M. Pastores, G. U. Meduri)
lease of cortisol from the adrenal cortex
key advantages is that unlike a face-to-
reviewed the task force bibliography for
(1–3). This activation is an essential com-
face meeting of experts, it eliminates the
relevant studies. Septic shock was defined
ponent of the general adaptation to illness
possibility that a specific expert might
by the American College of Chest Physi-
and stress and contributes to the mainte-
dominate the consensus process. The
cians/Society of Critical Care Medicine
nance of cellular and organ homeostasis.
Delphi method helps to minimize the ef-
Consensus Conference and ARDS by the
Adrenalectomized animals succumb rap-
fects of group interactions and maximizes
American–European Consensus Confer-
idly to hemorrhagic and septic shock, and
the ability to elicit expert knowledge.
ence (16, 17). Vasopressor dependency
steroid replacement is protective against
The task force members individually
was defined as the requirement for a va-
these challenges (4, 5).
and collectively undertook a systematic
sopressor agent after 7 days of treatment
Once considered a rare diagnosis in
search of published literature pertaining
with a glucocorticoid (GC). The reviewers
the intensive care unit, "adrenal failure"
to the diagnosis and treatment of adrenal
independently abstracted data from all el-
is being reported with increasing fre-
failure in critically ill adult patients using
igible studies. Data were abstracted on
quency in critically ill patients with septic
Medline, CINAHL, EMBASE, and the Co-
study design, study size, corticosteroid
shock, severe community-acquired pneu-
chrane library. In addition, the reference
dosage, vasopressor dependency, and 28-
monia, trauma, head injury, burns, liver
lists of relevant articles were reviewed for
day mortality. Study and data inclusion
failure, HIV infection, pancreatitis, after
additional published works. Key words
was by consensus. We used the random
cardiac surgery, after the use of etomi-
used in these searches included "pitu-
effects models using Review Manager 4.2
date, and in brain-dead organ donors (6 –
itary–adrenal system, adrenal insuffi-
(Cochrane Collaboration, Oxford, UK) for
11). Adrenal failure may be associated
ciency, adrenal glands, pituitary–adrenal
all analyses and considered p ⬍ .05 (two-
with structural damage to the adrenal
function tests, hydrocortisone, glucocor-
sided) as significant. Summary effects es-
gland, pituitary gland, or hypothalamus;
ticoids (GC), adrenal cortex hormones,
timates are presented as odds ratio with
however, many critically ill patients de-
glucocorticoid receptor (GR), critical
95% confidence intervals. We assessed
velop reversible failure of the HPA axis.
care, intensive care units, intensive care,
heterogeneity between studies using the
Although it is generally agreed that
ARDS, shock septic, sepsis, and sepsis
Cochran Q statistic with p ⬍ .10 indicat-
adrenal failure may be common in sub-
syndrome." A comprehensive bibliogra-
ing significant heterogeneity and the I2
groups of critically ill patients, the diag-
phy was developed, with the references
with suggested thresholds for low (25–
nosis and management of this disorder
stored and cataloged using an electronic
49%), moderate (50 –74%), and high
remains controversial, with poor agree-
reference manager (Reference Manager
(⬎75%) values (18 –21).
ment among the experts. The objective of
v11.1, Thompson ResearchSoft, Carlsbad,
this task force was therefore to develop
consensus statements by experts in the
We used electronic mail to conduct
field based on the best available scientific
the Delphi process. A list of questions for
Exposure to hostile conditions results
evidence (12).
review was determined. Once a majority
in a series of coordinated responses—
agreement was reached on each question,
often referred to as stress responses—
the strength of each recommendation
organized to enhance survival; these in-
was quantified using the Modified Grades
clude a series of complex central and
Experts were selected from the mem-
of Recommendation Assessment, Devel-
peripheral adaptations. This stress re-
bership lists of the Society of Critical
opment, and Evaluation (GRADE) system
sponse is mediated mainly by the HPA
Care Medicine (SCCM) and the European
developed by the American College of
axis and the sympathoadrenal system,
Society of Intensive Care Medicine (ES-
Chest Physicians (Appendix 1) (15). In all,
which includes the sympathetic nervous
ICM). Specific individuals were selected
there were seven rounds until a majority
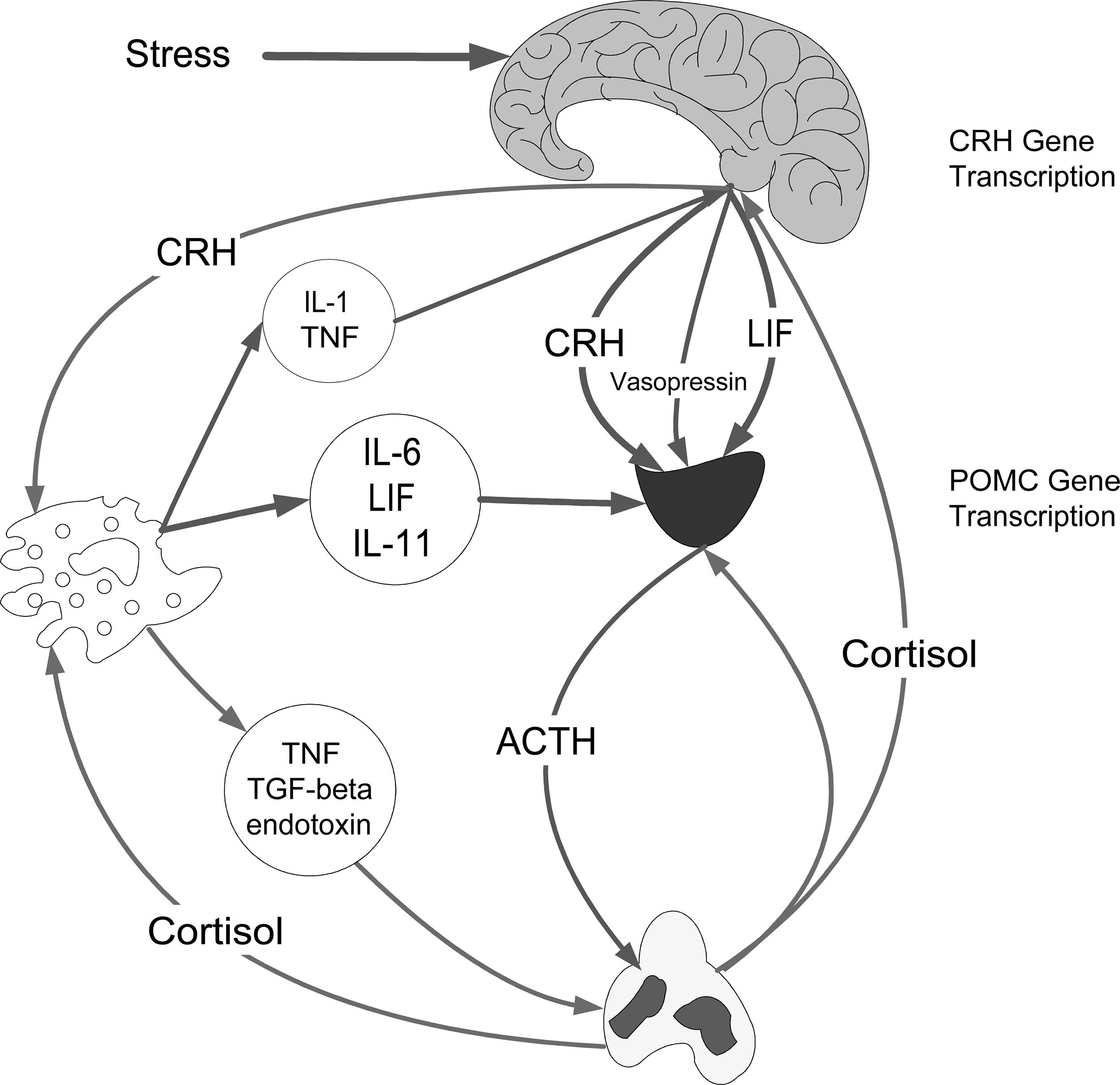
system and the adrenal medulla (Fig. 1)
to represent geographic diversity and a
agreement was achieved on all the ques-
(22–24). The HPA axis and the sympa-
broad range of expertise on the basis of
tions. In addition, the group met in Paris,
thoadrenal system are functionally re-
their published research. In addition, en-
France, in September 2005 and again at
lated. Activation of the sympathoadrenal
docrinologists with expertise in this area
the Society of Critical Care Medicine 35th
system results in the secretion of epi-
were invited to join the task force.
Critical Care Congress in San Francisco,
nephrine and norepinephrine from the
The consensus statement was devel-
CA, in January 2006 to review the
adrenal medulla and also leads to an in-
oped using a modified Delphi methodol-
progress of the Delphi process. The initial
creased production of inflammatory cyto-
ogy (12). The Delphi method, originally
draft of the manuscript was written by
kines, such as interleukin-6. Activation of
developed by the RAND Corporation, is a
the Chair (P. E. Marik). The draft manu-
the HPA axis results in increased secre-
structured process that uses a series of
script was reviewed and iteratively edited
tion from the paraventricular nucleus of
questionnaires, each referred to as a
by all members of the task force.
the hypothalamus of corticotropin-
round, to both gather and provide infor-
A meta-analysis of randomized con-
releasing hormone, a 41-amino acid pep-
mation (13, 14). With each round, the
trolled trials that compared the 28-day
tide, and arginine vasopressin. Cortico-
answers are modified based on the re-
mortality and vasopressor dependency of
tropin-releasing hormone plays a pivotal
sponses of the previous round. The
patients with septic shock and the 28-day
integrative role in the response to stress.
Crit Care Med 2008 Vol. 36, No. 6

receptor mediating selective cholesteroluptake (32–34). These receptors are ex-pressed at high levels in the parenchymalcells of the liver and the steroidogeniccells of the adrenal glands, ovary, andtestis (35).
Cortisol exerts its effects after uptake
from the circulation by binding to intra-cellular glucocorticoid receptors (GRs)(3). These receptors belong to a steroid-hormone-receptor superfamily of tran-scription factors, which are made up of aC-terminal ligand binding domain, a cen-tral DNA binding domain interactingwith specific DNA sequences on targetgenes, and an N-terminal hypervariableregion. The binding of cortisol to GR inthe cytoplasm results in the activation ofthe steroid receptor complex via a processinvolving the dissociation of heat shockproteins (heat shock proteins 90 and 70)and FK-506 binding proteins (36 –38). In-tracellularly, the cortisol-GR complexmoves to the nucleus, where it binds as ahomodimer to DNA sequences called glu-cocorticoid-responsive elements locatedin the promoter regions of target genes,
Figure 1. Activation of the hypothalamic-pituitary-adrenal axis by a stressor and the interaction with
which then activate or repress transcrip-
the inflammatory response. ACTH, adrenocorticotrophic hormone; CRH, corticotropin-releasing hor-
tion of the associated genes. In addition,
mone; IL-6, interleukin-6; IL-11, interleukin-11; LIF, leukemia inhibitory factor; POMC, pro-
the cortisol-GR complex may affect cellu-
opiomelanocortin; TGF-beta, transforming growth factor-; TNF, tumor necrosis factor.
lar function indirectly by binding to andmodulating the transcriptional activity ofother nuclear transcription factors, such
Corticotropin-releasing hormone stimu-
ing in a significant increase in the
as nuclear factor B (NF-B) and activa-
lates the production of ACTH by the an-
percentage of free cortisol (27, 28). The
tor protein-1. Overall, GCs affect the
terior pituitary, causing the zona fascicu-
circulating half-life of cortisol varies from
transcription of thousands of genes in
lata of the adrenal cortex to produce
70 to 120 mins. The adrenal gland does
every cell of the body. It has been esti-
more GCs (cortisol in humans, cortico-
not store cortisol; increased secretion
mated that GCs affect 20% of the genome
sterone in rats). Arginine vasopressin is a
arises due to increased synthesis under
of mononuclear blood cells (39).
weak ACTH secretagogue and vasoactive
the control of ACTH (29). Cholesterol is
GCs play a major role in regulating
peptide that acts synergistically with cor-
the principal precursor for steroid bio-
the activity of NF-B, which plays a cru-
ticotropin-releasing hormone to increase
synthesis in steroidogenic tissue. In a se-
cial and generalized role in inducing cy-
secretion of ACTH. The increase in corti-
ries of sequential enzymatic steps, cho-
tokine gene transcription (40 – 42).
sol production results in multiple effects
lesterol is converted to pregnenolone and
NF-B is normally maintained in an in-
(metabolic, cardiovascular, and immune)
then to the end products of adrenal bio-
active form by sequestration in the cyto-
aimed at maintaining or restoring ho-
synthesis, namely, aldosterone, dehydro-
plasm through interaction with inhibi-
meostasis during stress.
epiandrostenedione, and cortisol (29).
tory proteins (IBs). On stimulation by
The first and rate-limiting step in adrenal
Cortisol Physiology, Synthesis,
steroidogenesis is the formation of preg-
DNA, physical and chemical stresses, and
and Glucocorticoid Receptors
nenolone from cholesterol. At rest and
inflammatory cytokines, the latent NF-
during stress, about 80% of circulating
B/IB complex is activated by phosphor-
Cortisol is the major endogenous GC
cortisol is derived from plasma choles-
ylation and proteolytic degradation of
secreted by the adrenal cortex. More than
terol, the remaining 20% being synthe-
IB, with exposure of the NF-B nuclear
90% of circulating cortisol is bound to
sized in situ from acetate and other pre-
localization sequence. The liberated
corticosteroid-binding globulin, with
cursors (30). Experimental studies
NF-B then translocates to the nucleus
⬍10% in the free, biologically active suggest that high-density lipoprotein is and binds to promoter regions of targetform (25, 26). Corticosteroid-binding
the preferred cholesterol source of steroi-
genes to initiate the transcription of mul-
globulin is the predominant binding pro-
dogenic substrate in the adrenal gland
tiple cytokines (including tumor necrosis
tein, with albumin binding a lesser
(31). Recently, mouse SR-B1 (scavenger
factor-␣, interleukin-1, and interleukin-
amount. During acute illness, particu-
receptor, class B, type 1) and its human
6), cell adhesion molecules (e.g., intercel-
larly sepsis, corticosteroid-binding glob-
homolog (Cla-1) have been identified as
lular adhesion molecule-1, E-selectin),
ulin levels fall by as much as 50%, result-
the high-affinity high-density lipoprotein
and other mediators of inflammation.
Crit Care Med 2008 Vol. 36, No. 6

GCs inhibit the activity of NF-B by in-
widely (0 –77%), depending on the popu-
severe asthma, systematic lupus ery-
creasing the transcription of IBs and by
lation of patients studied and the diag-
thematosus, ulcerative colitis, and rheu-
directly binding to and inhibiting NF-B
nostic criteria. However, the overall prev-
matoid arthritis (62– 65). It is therefore
alence of adrenal insufficiency in
likely that acute inflammation, similar to
Cortisol has several important physio-
critically ill medical patients approxi-
chronic inflammation, may be associated
logic actions on metabolism, cardiovas-
mates 10 –20%, with a rate as high as
with tissue corticosteroid resistance (61).
cular function, and the immune system
60% in patients with septic shock. In a
In experimental models, endotoxin and
(6, 43). The metabolic effects of cortisol
study recently published by Annane et al.
proinflammatory cytokines have been
include an increase in blood glucose con-
(53), the prevalence of adrenal insuffi-
shown to cause decreased GR nuclear
centrations through the activation of key
ciency (as determined by metyrapone
translocation (66 – 68). In an ex vivo
enzymes involved in hepatic gluconeo-
testing) in patients with severe sepsis and
model, Meduri et al. (69) demonstrated
genesis and inhibition of glucose uptake
septic shock was reported to be 60%. The
reduced nuclear translocation of the GR
in peripheral tissues such as the skeletal
major effect of adrenal insufficiency in
complex in patients with fatal ARDS, de-
muscles. In addition, in adipose tissue,
the critically ill patient is manifested
spite adequate cytoplasmic (and serum)
lipolysis is activated, resulting in the re-
through alterations in the systemic in-
levels of cortisol. It is likely that multiple
lease of free fatty acids into the circula-
flammatory response and cardiovascular
mechanisms cause systemic inflamma-
tion. Cortisol also has a permissive effect
tion-associated GC resistance, including
on other hormones, increasing glucose
The mechanisms leading to dysfunc-
decreased GR number, increased expres-
levels, including catecholamines and glu-
tion of the HPA axis during critical illness
sion of the beta isoform of the GR (unable
cagon. Sustained cortisol hypersecretion
are complex and poorly understood and
to bind ligand), altered ratio of chaperone
stimulates glucose production at the ex-
likely include decreased production of
proteins (FK binding proteins and heat
pense of protein and lipid catabolism and
corticotropin-releasing hormone, ACTH,
shock protein 90), reduced affinity of the
insulin resistance.
and cortisol and the dysfunction of their
GR for ligand, altered nuclear receptor
Cortisol increases blood pressure
receptors. A subset of patients may have
coactivators, reduced DNA binding, de-
through several mechanisms involving
structural damage to the adrenal gland
creased histone acetylation, increased ac-
the kidney and vasculature. In vascular
from either hemorrhage or infarction,
tivity of the P-glycoprotein membrane
smooth muscle, cortisol increases sensi-
and this may result in long-term adrenal
transport pump, and increased conver-
tivity to vasopressor agents such as cat-
dysfunction. Adrenal hemorrhage has
sion of cortisol to cortisone (61, 68, 70 –
echolamines and angiotensin II (44, 45).
been described with blunt abdominal
72). Furthermore, polymorphisms of the
These effects are mediated partly by the
trauma, after major surgery, in dissemi-
GR and other pivotal genes may influence
increased transcription and expression of
nated intravascular coagulation associ-
the downstream effects of the GC–GR in-
the receptors for these hormones (44,
ated with sepsis, and in patients with
teraction (73, 74). Additional research in
45). Although the effect of GCs on nitric
burns, heparin-induced thrombocytope-
this area, particularly as it applies to crit-
oxide is complex, it seems to increase
nia, the antiphospholipid syndrome, HIV
ically ill patients, is urgently required.
endothelial nitric oxide synthetase,
infection, disseminated fungal infections,
Current evidence suggests that medi-
thereby maintaining microvascular per-
and tuberculosis (3, 54 –59). In addition,
ators released in patients with critical ill-
fusion (46 – 49). Cortisol has potent anti-
patients who have been treated long term
ness, and sepsis in particular, may either
inflammatory actions, including the re-
with adrenally suppressive doses of exog-
stimulate or impair the synthesis and ac-
duction in the number and function of
enous GCs are likely to develop secondary
tion of cortisol via actions on the HPA
various immune cells, such as T and B
adrenal insufficiency (3, 6). However, it
axis and the GR signaling system. The net
lymphocytes, monocytes, neutrophils,
seems that most critically ill patients who
effect of these opposing actions on the
and eosinophils, at sites of inflammation.
develop adrenal insufficiency develop re-
HPA axis and GR may be time dependent
Cortisol decreases the production of cy-
versible dysfunction of the HPA axis (6,
and, in addition, depend on the severity of
tokines, chemokines, and eicosanoids and
60). Decreased production of cortisol or
illness and the extent and pattern of me-
enhances the production of macrophage
ACTH is particularly common in patients
diator production. Although the focus on
migration inhibitory factor (22, 50).
with severe sepsis and septic shock (60).
most research has been in the area of
Annane et al. (53) demonstrated an in-
sepsis and ARDS, it is likely that similar
Dysfunction of the HPA Axis
creased risk of adrenal insufficiency in
mechanisms operate in other disorders
During Acute Illness
patients with positive blood cultures and
characterized by significant systemic in-
those with Gram-negative infections.
flammation, including pancreatitis,
The acute stress response during crit-
Clinical and experimental data indi-
burns, post-cardiopulmonary bypass, and
ical illness is characterized by activation
cate that the failure to improve in sepsis
liver failure (75–79).
of the HPA and sympathoadrenal system
and ARDS is frequently associated with
axis, with increased secretion of cortisol,
failure of activated GRs to down-regulate
RECOMMENDATIONS OF THE
an increase in the percentage of free cor-
the transcription of inflammatory cyto-
TASK FORCE
tisol, and increased translocation of the
kines, despite elevated levels of circulat-
GR complex into the nucleus. Impor-
ing cortisol, a condition defined as sys-
Critical Illness–Related Corticosteroid
tantly, there is increasing evidence that
temic inflammation-associated GC
in many critically ill patients, this path-
resistance (61). Tissue corticosteroid re-
way may be impaired (27, 51, 52). The
sistance is a well-known manifestation of
Recommendation 1: Dysfunction of the
reported prevalence of adrenal insuffi-
chronic inflammatory diseases, such as
HPA axis in critical illness is best de-
ciency in critically ill patients varies
chronic obstructive pulmonary disease,
scribed by the term critical illness–
Crit Care Med 2008 Vol. 36, No. 6

related corticosteroid insufficiency
Strength of Recommendation: 2B
adrenal gland to increase production of
cortisol in response to ACTH; it does not
Recommendation 2: The terms abso-
The diagnosis of adrenal insufficiency
assess the integrity of the HPA axis, the
lute or relative adrenal insufficiency
in critically ill patients has been based on
response of the HPA axis to other stresses
are best avoided in the context of crit-
the measurement of a random total se-
(i.e., hypotension, hypoglycemia), or the
ical illness.
rum cortisol ("stress" cortisol level) or
adequacy of stress cortisol levels. In ad-
the change in the serum cortisol in re-
dition, the ACTH stimulation test may be
Dysfunction of the HPA axis in critical
sponse to 250 g of synthetic ACTH
poorly reproducible, especially in patients
illness is best described by the term crit-
(ACTH stimulation test), the so-called
with septic shock (97, 98). Despite these
ical illness–related corticosteroid insuffi-
delta cortisol (6, 84). Both of these tests
limitations, Annane et al. (53) have re-
ciency (CIRCI). CIRCI is defined as inad-
have significant limitations in the criti-
ported that a delta cortisol of ⬍9 g/dL
equate cellular corticosteroid activity for
cally ill (85). Assays for serum cortisol
and a random total cortisol of ⬍10 g/dL
the severity of the patient's illness. CIRCI
measure the total hormone concentra-
were the best predictors of adrenal insuf-
manifests with insufficient GC-GR–
tion (serum-free cortisol plus the pro-
ficiency (as determined by metyrapone
mediated down-regulation of proinflam-
tein-bound fraction). The consensus is
testing) in patients with severe sepsis/
matory transcription factors, leading to
that the free cortisol, rather than the
septic shock. Furthermore, although the
persistent elevation of proinflammatory
protein-bound fraction, is responsible for
1-g ACTH stimulation test may be more
mediators over time. CIRCI occurs as a
the physiologic function of the hormone
physiologic and have a greater sensitivity
result of a decrease in adrenal steroid
at the cellular level (6, 50, 86). In most
than the 250-g test, due to limited data,
production (adrenal insufficiency) or tis-
critically ill patients, corticosteroid-
the 1-g test dose is currently not rec-
sue resistance to GCs (with or without
binding globulin levels are decreased and
ommended (99). It should also be appre-
adrenal insufficiency). Adrenal insuffi-
the percentage of free cortisol is in-
ciated that at present, we are unable to
ciency may arise due to dysfunction at
creased (27, 51, 52, 86, 87). Furthermore,
measure tissue GC resistance or deter-
any point in the HPA axis. The terms
with acute stimulation of the adrenal
mine the circulating cortisol level that is
absolute or relative adrenal insufficiency
gland, the relative increase of free bioac-
required to overcome tissue resistance.
are best avoided in the context of critical
tive cortisol concentrations is substan-
In those patients (severe sepsis, septic
illness (80). CIRCI is a dynamic process
tially more pronounced than the increase
shock, and ARDS) most likely to benefit
(i.e., patients may not have CIRCI at ad-
of total cortisol concentrations (27, 51,
from treatment with moderate-dose GCs,
mission to the hospital/intensive care
52, 86 – 88). Consequently, in critically ill
it is not clear that treatment should be
unit but may develop CIRCI during the
patients, the total serum cortisol level
based on the results of adrenal function
course of their illness) (81– 83). CIRCI is
may not accurately reflect the free corti-
testing. To date, six randomized, placebo-
usually a reversible condition caused by
sol level. This dissociation between the
controlled studies have evaluated hydro-
proinflammatory mediators; however, it
total and free cortisol level is most
cortisone treatment (200 –300 mg/day) in
may also arise due to structural damage
marked in patients with a serum albumin
patients with septic shock (95, 100 –103)
of the adrenal gland. CIRCI may affect the
of ⬍2.5 mg/dL (85, 87, 89).
(Figs. 2 and 3). In these studies, more
balance between proinflammatory and
Although measurement of the free
rapid shock reversal was noted in patients
anti-inflammatory pathways and thereby
cortisol level may arguably be prefera-
treated with hydrocortisone, and this
influence immune, metabolic, vascular,
ble, this test is currently not widely
benefit was noted in both ACTH respond-
and organ dysfunction.
available. It is likely, however, that with
ers (delta cortisol of ⬎9 mg/dL) and non-
Diagnosis of Adrenal Insufficiency
improvement in laboratory techniques
responders (delta cortisol of ⬍9 mg/dL)
and clinical demand, this test will be-
(Fig. 2). Furthermore, recent randomized
Recommendation 3: At this time, adre-
come commercially available (90). The
controlled studies in patients with early
nal insufficiency in critical illness is
interpretation of the total serum cortisol
ARDS (treatment within 14 days) and se-
best diagnosed by a delta cortisol (after
concentration is further complicated by
vere community-acquired pneumonia
250 g cosyntropin) of ⬍9 g/dL or a
the fact that the specificity, sensitivity,
demonstrated improved outcome with
random total cortisol of ⬍10 g/dL.
and performance of the commercially
GCs (when compared with placebo), in-
Strength of Recommendation: 2B
available assays are not uniform (91). It is
dependent of adrenal function testing
likely that the variation in assay charac-
(see section below) (7, 104, 105). These
Recommendation 4: The use of free
teristics might be even more significant
data suggest that in patients with septic
cortisol measurements cannot be rec-
in critically ill patients, especially those
shock and early ARDS, the decision to
ommended for routine use at this time.
with septic shock (91, 92). Cross-reactiv-
treat with moderate-dose corticosteroids
Although the free cortisol assay has
ity of the cortisol immunoassay with pre-
should be based on clinical criteria and
advantages over the total serum corti-
cursors or metabolites of cortisol that
not on the results of adrenal function
sol, this test is not readily available.
accumulate in sepsis may account for this
testing. The inability to diagnose cortico-
Furthermore, the normal range of the
steroid tissue resistance may partly ex-
free cortisol in critically ill patients is
Although a delta cortisol of ⬍9 g/dL
plain these observations.
currently unclear.
has proven to be an important prognostic
Strength of Recommendation: 2B
Who to Treat with Glucocorticoids?
marker (9, 53, 93, 94), and a marker of
Recommendation 5: The ACTH stimu-
response to treatment with corticoste-
Recommendation 6: Hydrocortisone
lation test should not be used to iden-
roids (95, 96), the ACTH stimulation test
should be considered in the manage-
tify those patients with septic shock or
has a number of limitations. The delta
ment strategy of patients with septic
ARDS who should receive GCs.
cortisol is a measure of the ability of the
shock, particularly those patients who
Crit Care Med 2008 Vol. 36, No. 6
Figure 2. Meta-analysis of treatment with moderate-dose hydrocortisone on shock reversal at day 7 in patients with septic shock grouped by response to
adrenocorticotrophic hormone. RR, relative risk; 95% CI, 95% confidence interval.
Figure 3. Meta-analysis of treatment with moderate-dose hydrocortisone on 28-day survival in patients with septic shock. RR, relative risk; 95% CI, 95%
confidence interval.
have responded poorly to fluid resusci-
in study size, inclusion criteria, and cor-
fludrocortisone (50 g daily) or matching
tation and vasopressor agents.
ticosteroid dosing limits the interpreta-
placebo for 7 days. All patients underwent
Strength of Recommendations: 2B
tion of this meta-analysis. Nevertheless,
an ACTH stimulation test. There was a
the French multicenter study and the re-
30% decrease in 28-day mortality in the
The benefit of moderate-dose hydro-
cently completed European multicenter
cortisone (200 –300 mg/day) in patients
study (CORTICUS) were better powered
(hazard ratio, 0.67; 95% confidence inter-
with septic shock has been evaluated in
to detect a survival difference and deserve
val, 0.47– 0.95; p ⫽ .02) (95). This benefit
six randomized controlled trials (95,
further analysis. Annane et al. (95) ran-
was confined to the group of nonre-
100 –103, 106). A meta-analysis of these
domized 300 patients with refractory sep-
sponders (delta cortisol of ⬍9 g/dL).
six studies (including the recently com-
tic shock (systolic blood pressure of ⬍90
The CORTICUS study was a double-
pleted CORTICUS study) demonstrates
mm Hg for ⬎1 hr, despite fluid resusci-
blind, randomized, placebo-controlled
greater shock reversal (at day 7) with
tation and the use of vasopressor agents)
study performed in 52 centers through-
hydrocortisone but no benefit in terms of
to treatment with hydrocortisone (50 mg
out Europe (106). A total of 500 patients
mortality (Figs. 2 and 3). The variability
intravenously every 6 hrs) and oral
(499 available to analyze) were enrolled
Crit Care Med 2008 Vol. 36, No. 6


between March 2002 and November
lay in instituting treatment. It is also
resolution of shock was noted in both
2005. Inclusion criteria included septic
possible that improvements in the sup-
responders and nonresponders. Thus, at
shock (systolic blood pressure of ⬍90
portive care of critically ill patients with
this time, it seems that the decision to
mm Hg, despite adequate fluid resuscita-
septic shock over the last decade have
treat patients with septic shock should
tion or need for vasopressors) and evi-
increased the survival of patients with
not be based on the results of a random
dence of organ dysfunction attributable
CIRCI who would otherwise have died.
total cortisol level or the response to
to sepsis. Patients were randomized to
The demographics and clinical character-
ACTH. In addition, it should be noted
hydrocortisone (50 mg intravenously ev-
istics of the patients enrolled in the two
that the administration of hydrocortisone
ery 6 hrs for 5 days, then 50 mg intrave-
studies were quite different, with 40.1%
during septic shock has been demon-
nously every 12 hrs for 3 days, followed
of patients in the French study being
strated to reduce the prevalence of post-
by 50 mg intravenously daily for 3 days)
surgical patients as compared with 64.5%
traumatic stress disorder and improve
or matching placebo. Patients did not re-
in the CORTICUS study. Source control
the emotional well-being of survivors of
ceive fludrocortisone. Although the base-
may be more important in determining
septic shock (110).
line characteristics of the patients were
the outcome of sepsis in surgical patients
similar, only 35% of the cohort were
than that of adjunctive interventions.
Recommendation 7: Moderate-dose GC
medical patients, with the abdomen be-
Furthermore, it is possible that selection
should be considered in the manage-
ing the commonest source of infection
bias affected the demographics and out-
ment strategy of patients with early
(48%). There was no difference in the
come of the CORTICUS study. Although
severe ARDS (PaO /F
28-day all-cause mortality between those
it has been suggested that clinical equi-
before day 14 in patients with unre-
patients who received hydrocortisone as
poise existed during enrollment into the
solving ARDS. The role of GC treat-
compared with placebo. Furthermore,
CORTICUS study (107), many intensivists
ment in acute lung injury and less se-
there was no difference in mortality be-
continue to use corticosteroids in the
vere ARDS (PaO /F
of ⬎200) is less
tween the groups when stratified as re-
management of patients with septic
sponders (delta cortisol of ⬎9 g/dL) or
shock (108, 109).
Strength of Recommendations: 2B
nonresponders (delta cortisol of ⬍9 g/
Given the different outcomes of the
dL) to the ACTH stimulation test. How-
French and CORTICUS studies, what
Five randomized studies (n ⫽ 518)
ever, the patients who received hydrocor-
should the clinician do? Considering the
have evaluated the role of GC treatment
tisone had more rapid resolution of shock
central role of cortisol in modulating the
in patients with acute lung injury due to
(p ⫽ .001 for responders and p ⫽ .06 for
stress response and recognizing the po-
community-acquired pneumonia (7) and
nonresponders). There were, however,
tential suppressive effects of sepsis on the
in patients with ARDS of varied origins
more episodes of new infection (not sta-
HPA axis and on GR activity, the use of
(104, 105, 111, 112). Varying doses (200 –
tistically significant) and septic shock (re-
moderate-dose hydrocortisone seems ra-
750 mg of hydrocortisone equivalents per
bound inflammation) in the hydrocorti-
tional in patients with septic shock poorly
day), dosing strategies (infusion/bolus),
sone group. The prevalence of other
responsive to fluid and vasopressor resus-
and duration of therapy (7–32 days) were
adverse events, including critical illness
citation. This is supported by recent data
used in these studies. Due to the marked
polyneuropathy, was similar between
that demonstrate that up to 60% of pa-
differences in study design and patient
tients with severe sepsis and septic shock
characteristics, the cumulative summary
A number of factors may account for
have adrenal insufficiency (53). The best
of these studies should be interpreted
the different results of the French multi-
available clinical evidence suggests that
with some caution. Nevertheless, these
center study and the CORTICUS study.
moderate-dose hydrocortisone results in
trials consistently reported that treat-
The patients enrolled in the French study
significantly more rapid resolution of
ment was associated with significant im-
were sicker than those enrolled in the
shock (Fig. 2). The effects of moderate-
provement in PaO /F
(7, 104, 105, 111,
CORTICUS study (28-day mortality in the
dose hydrocortisone on mortality seem
112), a significant reduction in markers
placebo arm of 61% vs. 31.5%). Further-
less clear (Fig. 3). Nevertheless, based on
of systemic inflammation (7, 104, 105,
more, the time window of enrollment was
current data, hydrocortisone should be
111, 112), duration of mechanical venti-
8 hrs in the French study as compared
considered in the management strategy
lation (7, 104, 105, 111, 112), and inten-
with 72 hrs in the CORTICUS study. It is
of patients with septic shock, particularly
sive care unit length of stay (all with p
likely that only patients at a high risk of
those patients who have responded poorly
values of ⬍.05) (7, 104, 105, 111). Sub-
death will benefit from corticosteroids,
to fluid resuscitation and vasopressor
group analysis (Fig. 4) based on studies
and this benefit may diminish with a de-
agents. As noted in Figure 2, more rapid
that investigated only treatment (methyl-
Figure 4. Effects of prolonged methylprednisolone treatment on mechanical ventilation–free days at day 28. Reproduced with permission from Meduri et
al (114). WMD, weighted mean difference; 95% CI, 95% confidence interval.
Crit Care Med 2008 Vol. 36, No. 6
prednisolone) durations of ⬎1 wk (n ⫽
a distinct reduction in the relative risk of
day). The optimal initial dosing regi-
295) (104, 105, 111) showed a distinct
death (82/214 [38%] vs. 98/186 [52.5%];
men in patients with early severe ARDS
increase in the number of mechanical
relative risk, 0.78; 95% confidence inter-
is 1 mg·kg⫺1·day⫺1 methylpred-
ventilation–free days (weighted mean dif-
val, 0.64 – 0.96; p ⫽ .02) (114). When an-
nisolone as a continuous infusion.
ference, 5.59 days; 95% confidence inter-
alyzing the three trials investigating cor-
Strength of Recommendation: 1B
val, 3.49 –7.68; p ⬍ .001).
ticosteroids for durations of ⬎1 wk
GC treatment in acute lung injury–
initiated before day 14 of ARDS (n ⫽
Recommendation 9: The optimal dura-
ARDS was not associated with increased
245), mortality was equally decreased
tion of GC treatment in patients with
rates of gastrointestinal bleeding or nos-
(35/144 [24%] vs. 40/101 [40%]; relative
septic shock and early ARDS is unclear.
ocomial infections, and two of the studies
risk, 0.62; 95% confidence interval, 0.43–
However, based on published studies
reported a reduction in the rate of noso-
0.90; p ⫽ .01) (Fig. 5) (114).
and pathophysiological data, patients
comial infections, likely attributable to
The results of one randomized trial
with septic shock should be treated for
the shorter duration of mechanical ven-
(111) indicate that 1 mg·kg⫺1·day⫺1
ⱖ7 days before tapering, assuming
tilation (104, 105). In the two random-
methylprednisolone, given as an infusion
that there is no recurrence of signs of
ized trials (104, 111) that incorporated
and tapered over the course of 4 wks, is
sepsis or shock. Patients with early
infection surveillance, nosocomial infec-
associated with a favorable risk– benefit
ARDS should be treated for ⱖ14 days
tions were frequently (56%) identified in
profile when secondary preventive mea-
before tapering.
the absence of fever. The combination of
sures are implemented. These measures
Strength of Recommendation: 2B
GCs and neuromuscular blocking agents
include 1) intensive infection surveil-
significantly increases the risk for pro-
lance, 2) avoidance of paralytic agents,
Recommendation 10: GC treatment
longed neuromuscular weakness (113).
and 3) avoidance of rebound inflamma-
should be tapered slowly and not
In the ARDS Network trial, although both
tion with premature discontinuation of
stopped abruptly.
groups had similar exposure to paralytic
treatment that may lead to physiologic
Strength of Recommendation: 2B
agents (49% vs. 42%; p ⫽ .3), those ran-
deterioration and reintubation. It should
domized to methylprednisolone had a
be noted that the premature and rapid
Recommendation 11: Treatment with
higher rate of serious events associated
taper of corticosteroids in the ARDS Net-
fludrocortisone (50 g orally once
with myopathy or neuropathy (105). The
work trial resulted in a deterioration of
daily) is considered optional.
other four trials did not report an in-
and a higher reintubation
Strength of Recommendation: 2B
creased rate of neuromuscular complica-
rate in the treatment group (105, 114).
tions (7, 104, 111, 112).
Preliminary data suggest that GCs
Recommendation 12: Dexamethasone
A reduction in mortality was noted in
may be of benefit in patients with severe
is not recommended for the treatment
four studies (7, 104, 111, 112). The ARDS
community-acquired pneumonia, liver
of septic shock or ARDS.
Network trial reported increased 60-day
failure, pancreatitis, patients undergoing
Strength of Recommendation: 1B
mortality in the subgroup randomized to
cardiopulmonary bypass, and during
methylprednisolone after 14 days of
weaning from mechanical ventilation (7,
Ideally, the dose of GC should be suf-
ARDS (105). This small subgroup (n ⫽
10, 11, 75, 96, 115). The potential bene-
ficient to down-regulate the proinflam-
48), however, had large imbalances in
fits of treatment with hydrocortisone in
matory response without causing im-
baseline characteristics, and the mortal-
these patient subgroups and other criti-
mune-paresis and interfering with wound
ity difference lost significance (p ⫽ .57)
cally ill patients deserve further investi-
healing. Similarly, the duration of GC
when adjusting for these imbalances
therapy should be guided by the duration
(114). The two small clinical trials (n ⫽
of CIRCI and the associated duration of
How to Treat
68) (7, 111) showed marked reduction in
systemic inflammation. The optimal dose
the relative risk of death with GC therapy
Recommendation 8: In patients with
and duration of treatment with hydrocor-
(2/39 [5%] vs. 11/31 [35%]; relative risk,
septic shock, intravenous hydrocorti-
tisone/methylprednisolone remains to be
0.15; 95% confidence interval, 0.04 –
sone should be given in a dose of 200
determined in well-controlled and well-
0.59; p ⫽ .007). The three subsequently
mg/day in four divided doses or as a
powered studies. However, the results of
published larger clinical trials (104, 105,
bolus of 100 mg followed by a contin-
published studies do allow us to make a
112), when combined (n ⫽ 400), achieved
uous infusion at 10 mg/hr (240 mg/
number of recommendations. A number
Figure 5. Effects of prolonged glucocorticoid treatment initiated before day 14 of acute lung injury-acute respiratory distress syndrome on survival.
Reproduced with permission from Meduri et al (114). RR, relative risk; 95% CI, 95% confidence interval.
Crit Care Med 2008 Vol. 36, No. 6
of randomized controlled studies have in-
nisolone for ⱖ14 days, followed by a slow
with septic shock and ARDS. At this time,
vestigated the utility of a high-dose,
taper while monitoring indices of oxygen-
treatment with moderate-dose corticoste-
short-course treatment with corticoste-
roids is recommended in patients with
roids in patients with ARDS and sepsis.
Meduri et al. (124) demonstrated that
septic shock who have responded poorly
Doses of methylprednisolone as high as
persistent elevation of inflammatory cy-
to volume resuscitation and vasopressor
20 –30 mg/kg body weight (10,000 to
tokines predicted a poor outcome in pa-
agents. The consistent positive results re-
40,000 mg of hydrocortisone) during the
tients with ARDS. Recently, two longitu-
ported in patients with early severe ARDS
course of 24 hrs were investigated (116 –
dinal studies in patients with severe
of ⬍200) and unresolving
118). These studies were unable to dem-
community-acquired pneumonia found
ARDS treated with GCs before day 14
onstrate an improved outcome, and there
high levels of circulating inflammatory
suggest that treatment with moderate-
was a higher risk of complications in the
cytokines 3 wks after clinical resolution
dose GCs should be considered in these
patients who received high-dose cortico-
of sepsis (125, 126). The larger study,
patients. Tests of adrenal function are not
steroids (116 –118). The literature there-
involving 1,886 patients, showed hospital
routinely required in these patients. The
fore does not support the use of high-
mortality to be associated with higher
role of GCs in the management of pa-
dose corticosteroids in critically ill
circulating inflammatory cytokine levels
tients with community-acquired pneu-
patients (except to prevent/treat rejection
and persistent elevation over time (125).
monia, liver failure, pancreatitis, those
in transplant patients).
Furthermore, higher circulating inter-
undergoing cardiac surgery, and other
Myopathy and an increased risk of su-
leukin-6 levels at intensive care unit dis-
groups of critically ill patients requires
perinfections are more common in pa-
charge were associated with increased
tients receiving ⬎300 mg of hydrocorti-
risk of death over 3 months (127). These
sone equivalents per day (117, 118).
data support the concept of immune dys-
Furthermore, while suppressing an exag-
regulation in severe sepsis and ARDS (in-
gerated proinflammatory response, a
sufficient corticosteroid activity–CIRCI)
1. Jurney TH, Cockrell JL Jr, Lindberg JS, et
dose of 200 –300 mg of hydrocortisone
and suggest that the duration of treat-
al: Spectrum of serum cortisol response to
per day does not seem to have immuno-
ment with GCs should be guided by the
ACTH in ICU patients: Correlation with de-
suppressive effects (119, 120). Based on
duration of elevation of inflammatory cy-
gree of illness and mortality. Chest 1987;
these data and the treatment protocol
tokines (124). Further studies should ex-
2. Reincke M, Allolio B, Wurth G, et al: The
used in the French and CORTICUS stud-
plore this concept.
hypothalamic-pituitary-adrenal axis in crit-
ies, we recommend that patients with
In the French study, patients in the
ical illness: Response to dexamethasone and
septic shock be treated with 50 mg of
treatment group received hydrocortisone
corticotropin-releasing hormone. J Clin
hydrocortisone intravenously every 6 hrs
together with fludrocortisone (50 g
Endocrinol Metab 1993; 77:151–156
or a bolus of 100 mg, followed by a con-
orally once daily), whereas in the CORTI-
3. Arlt W, Allolio B: Adrenal insufficiency.
tinuous intravenous infusion at 10 mg/hr
CUS study patients received hydrocorti-
Lancet 2003; 361:1881–1893
(340 mg the first day; 240 mg/day on
sone alone. It is unclear if the addition of
4. Hinshaw LB, Beller BK, Chang AC, et al:
subsequent days). The use of a continu-
fludrocortisone played a role in the favor-
Corticosteroid/antibiotic treatment of adre-
ous infusion of hydrocortisone has been
able outcome of the French study. The
nalectomized dogs challenged with lethal E.
reported to result in better glycemic con-
benefit of the addition of fludrocortisone
coli. Circ Shock 1985; 16:265–277
5. Darlington DN, Chew G, Ha T, et al: Corti-
trol, with less variability of blood glucose
in patients with septic shock is currently
costerone, but not glucose, treatment en-
concentration and a reduction in the staff
being investigated in two randomized
ables fasted adrenalectomized rats to sur-
workload of managing hyperglycemia
controlled trials comparing hydrocorti-
vive moderate hemorrhage. Endocrinology
(85, 121–123). Treatment should con-
sone alone vs. hydrocortisone together
1990; 127:766 –772
tinue for ⱖ7 days before tapering, assum-
with fludrocortisone (www.ClinicalTrial.
6. Marik PE, Zaloga GP: Adrenal Insufficiency
ing that there is no recurrence of signs of
gov NCT 00368381 and NCT00320099).
in the critically ill: A new look at an old
sepsis or shock. Hydrocortisone should
Treatment with fludrocortisone is consid-
problem. Chest 2002; 122:1784 –1796
be tapered slowly and not stopped
ered optional at this time.
7. Confalonieri M, Urbino R, Potena A, et al:
abruptly. The hydrocortisone dose should
Although treatment with dexametha-
Hydrocortisone infusion for severe commu-
be reduced every 2–3 days in small steps,
sone has been suggested in patients with
nity-acquired pneumonia: A preliminaryrandomized study. Am J Respir Crit Care
unless there is clinical deterioration,
septic shock until an ACTH stimulation
Med 2005; 171:242–248
which would then require an increase in
test is performed, this approach can no
8. Dimopoulou I, Tsagarakis S: Hypothalamic-
hydrocortisone dose. Abruptly stopping
longer be endorsed. This recommenda-
pituitary dysfunction in critically ill pa-
hydrocortisone will likely result in a re-
tion is based on the fact that dexametha-
tients with traumatic and nontraumatic
bound of proinflammatory mediators,
sone leads to immediate and prolonged
brain injury. Intensive Care Med 2005; 31:
with recurrence of the features of shock
suppression of the HPA axis (limiting the
(and tissue injury) (105, 119). In addi-
value of ACTH testing).
9. Tsai MH, Peng YS, Chen YC, et al: Adrenal
tion, it should be appreciated that GC
insufficiency in patients with cirrhosis, se-
treatment itself results in down-regula-
vere sepsis and septic shock. Hepatology
tion of GR levels in most cells, potentiat-
2006; 43:673– 681
10. Eklund A, Leppaniemi A, Kemppainen E, et
ing the rebound phenomenon with the
CIRCI is a complex and frequent dis-
al: Vasodilatory shock in severe acute pan-
abrupt cessation of GC treatment (70).
order of which our understanding contin-
creatitis without sepsis: Is there any place
Currently, the optimal dose and duration
ues to evolve. Although CIRCI may affect
for hydrocortisone treatment? Acta Anaes-
of therapy in patients with early severe
a spectrum of critically ill patients, most
thesiol Scand 2005; 49:379 –384
ARDS is 1 mg·kg⫺1·day⫺1 methylpred-
of the research has focused on patients
11. Fernandez J, Escorsell A, Zabalza M, et al:
Crit Care Med 2008 Vol. 36, No. 6
Adrenal insufficiency in patients with cir-
27. Ho JT, Al-Musalhi H, Chapman MJ, et al:
hibition of NF-kappa B activity through in-
rhosis and septic shock: Effect of treatment
Septic shock and sepsis: A comparison of
duction of I kappa B synthesis. Science
with hydrocortisone on survival. Hepatol-
total and free plasma cortisol levels. J Clin
1995; 270:286 –290
ogy 2006; 44:1288 –1295
Endocrinol Metab 2006; 91:105–114
41. Barnes PJ, Adcock I: Anti-inflammatory ac-
12. Definitions of ACCP evidence-based guide-
28. Dimopoulou I, Alevizopoulou P, Dafni U, et
tions of steroids: Molecular mechanisms.
lines, consensus statements, and other re-
al: Pituitary-adrenal response to human
Trends Pharmacol Sci 1993; 14:436 – 441
views and projects. American College of
corticotropin-releasing hormone in criti-
42. Barnes PJ, Karin M: Nuclear factor-kB-A
Chest Physicians, 2007. Available at: http://
cally ill patients. Intensive Care Med 2007;
pivotal transcription factor in chronic in-
flammatory diseases. N Engl J Med 1997;
definitions.php. Accessed February 2, 2008
29. Arlt W, Stewart PM: Adrenal corticosteroid
13. Fink A, Kosecoff J, Chassin M, et al: Con-
biosynthesis, metabolism, and action. En-
43. Oelkers W: Adrenal insufficiency. N Engl
sensus methods: Characteristics and guide-
docrinol Metab Clin North Am 2005; 34:
J Med 1996; 335:1206 –1212
lines for use. Am J Public Health 1984;
44. Collins S, Caron MG, Lefkowitz RJ: Beta-
30. Borkowski AJ, Levin S, Delcroix C, et al:
adrenergic receptors in hamster smooth
14. Williams PL, Webb C, Williams PL, et al:
Blood cholesterol and hydrocortisone pro-
muscle cells are transcriptionally regulated
The Delphi technique: A methodological
duction in man: Quantitative aspects of the
by glucocorticoids. J Biol Chem 1988; 263:
discussion. J Adv Nurs 1994; 19:180 –186
utilization of circulating cholesterol by the
15. Guyatt G, Gutterman D, Baumann MH, et
adrenals at rest and under adrenocortico-
45. Sakaue M, Hoffman BB: Glucocorticoids in-
al: Grading strength of recommendations
tropin stimulation. J Clin Invest 1967; 46:
duce transcription and expression of the
and quality of evidence in clinical guide-
alpha 1B adrenergic receptor gene in DTT1
lines: Report from an American College of
31. Yaguchi H, Tsutsumi K, Shimono K, et al:
MF-2 smooth muscle cells. J Clin Invest
Chest Physicians Task Force. Chest 2006;
Involvement of high density lipoprotein as
1991; 88:385–389
substrate cholesterol for steroidogenesis by
46. Limbourg FP, Huang Z, Plumier JC, et al:
16. Bone RC, Balk RA, Cerra FB, et al: Defini-
bovine adrenal fasciculo-reticularis cells.
Rapid nontranscriptional activation of en-
tions for sepsis and organ failure and guide-
Life Sci 1998; 62:1387–1395
dothelial nitric oxide synthase mediates in-
lines for the use of innovative therapies in
32. Acton S, Rigotti A, Landschultz KT, et al:
creased cerebral blood flow and stroke pro-
sepsis: The ACCP/SCCM Consensus Confer-
Identification of scavenger receptor SR-BI
tection by corticosteroids. J Clin Invest
ence Committee. American College of Chest
as a high density lipoprotein receptor. Sci-
2002; 110:1729 –1738
Physicians/Society of Critical Care Medi-
ence 1996; 271:518 –520
47. Hafezi-Moghadam A, Simoncini T, Yang Z,
cine. Chest 1992; 101:1644 –1655
33. Calco D, Gomez-Coronado D, Lasuncion
et al: Acute cardiovascular protective effects
17. Bernard GR, Artigas A, Brigham KL: The
MA, et al: CLA-I is an 85-kD plasma mem-
of corticosteroids are mediated by non-
American-European Consensus Conference
brane glycoprotein that acts as a high affin-
transcriptional activation of endothelial ni-
on ARDS: Definitions, mechanisms, rele-
ity receptor for both native (HDL, LDL, and
tric oxide synthase. Nat Med 2002;
vant outcomes, and clinical trial coordina-
VLDL) and modified (OxLDL and AcLDL)
tion. Am J Respir Crit Care Med 1994; 149:
lipoproteins. Arterioscler Thromb Vasc Biol
48. Bobadilla NA, Tapia E, Jimenez F, et al:
1997; 17:2341–2349
Dexamethasone increases eNOS gene ex-
18. Cochran W: The combination of estimates
34. de la Llera-Moya M, Connelly MA, Drazul D,
pression and prevents renal vasoconstric-
from different experiments. Biometrics
et al: Scavenger receptor class B type 1
tion induced by cyclosporin. Am J Physiol
1954; 10:101–129
affects cholesterol homeostasis by magnify-
1999; 277:F464 –F471
19. Berlin JA, Laird NM, Sacks HS, et al: A
ing cholesterol flux between cells and HDL.
49. Murata T, Hori M, Sakamoto K, et al: Dexa-
comparison of statistical methods for com-
J Lipid Res 2001; 42:1969 –1978
methasone blocks hypoxia-induced endo-
bining event rates from clinical trials. Stat
35. Liu J, Heikkila P, Meng QH, et al: Expres-
thelial dysfunction in organ-cultured pul-
Med 1989; 8:141–151
sion of low and high density lipoprotein
20. Higgins JP, Thompson SG: Quantifying het-
receptor genes in human adrenals. Eur J
monary arteries. Am J Respir Crit Care Med
erogeneity in a meta-analysis. Stat Med
Endocrinol 2000; 142:677– 682
2004; 170:647– 655
2002; 21:1539 –1558
36. Rhen T, Cidlowski JA: Antiinflammatory ac-
50. Cooper MD, Stewart PM: Corticosteroid in-
21. Higgins JP, Thompson SG, Deeks JJ, et al:
tion of glucocorticoids–new mechanisms
sufficiency in acutely ill patients. N Engl
Measuring inconsistency in meta-analyses.
for old drugs. N Engl J Med 2005; 353:
J Med 2003; 348:727–734
BMJ 2003; 327:557–560
51. Widmer IE, Puder JJ, Konig C, et al: Corti-
22. Chrousos GP: The hypothalamic-pituitary-
37. Sinars CR, Cheung-Flynn J, Rimerman RA,
sol response in relation to the severity of
adrenal axis and immune-mediated inflam-
et al: Structure of the large FK506-binding
stress and illness. J Clin Endocrinol Metab
mation. N Engl J Med 1995; 332:1351–1362
protein FKBP51, an Hsp90-binding protein
2005; 90:4579 – 4586
23. Carrasco GA, Van de Kar LD, Carrasco GA,
and a component of steroid receptor com-
52. Vogeser M, Groetzner J, Kupper C, et al:
et al: Neuroendocrine pharmacology of
plexes. Proc Nat Acad Sci U S A 2003; 100:
Free serum cortisol during the postopera-
stress. Eur J Pharmacol 2003; 463:235–272
tive acute phase response determined by
24. Miller DB, O'Callaghan JP, Miller DB, et al:
38. Vermeer H, Hendriks-Stegeman BI, van der
equilibrium dialysis liquid chromatogra-
Neuroendocrine aspects of the response to
BB, et al: Glucocorticoid-induced increase
phy-tandem mass spectrometry. Clin Chem
stress. Metab Clin Exp 2002; 51:5–10
in lymphocytic FKBP51 messenger ribonu-
Lab Med 2003; 41:146 –151
25. Dunn JF, Nisula BC, Rodbard D: Transport
cleic acid expression: A potential marker for
53. Annane D, Maxime V, Ibrahim F, et al: Di-
of steroid hormones: Binding of 21 endog-
glucocorticoid sensitivity, potency, and bio-
agnosis of adrenal insufficiency in severe
enous steroids to both testosterone-binding
availability. J Clin Endocrinol Metab 2003;
sepsis and septic shock. Am J Respir Crit
globulin and corticosteroid-binding globu-
Care Med 2006; 174:1319 –1326
lin in human plasma. J Clin Endocrinol
39. Galon J, Franchimont D, Hiroi N, et al:
54. Vella A, Nippoldt TB, Morris JC III: Adrenal
Metab 1981; 53:58 – 68
Gene profiling reveals unknown enhancing
hemorrhage: A 25-year experience at the
26. Mueller UW, Potter JM: Binding of cortisol
and suppressive actions of glucocorticoids
Mayo Clinic. Mayo Clin Proc 2001; 76:
to human albumin and serum: The effect of
on immune cells. FASEB J 2002; 16:61–71
protein concentration. Biochem Pharmacol
40. Auphan N, Didonato JA, Rosette C, et al:
55. Kovacs KA, Lam YM, Pater JL: Bilateral
1981; 30:727–733
Immunosuppression by glucocorticoids: In-
massive adrenal hemorrhage: Assessment of
Crit Care Med 2008 Vol. 36, No. 6
putative risk factors by the case-control
to glucocorticoids. Neuroimmunomodula-
of current assessment methods. J Clin En-
method. Medicine 2001; 80:45–53
tion 2005; 12:321–338
docrinol Metab 2006; 91:3725–3745
56. Deeb SA, Rosenberg RB, Wilkerson RJ, et al:
70. Schaaf MJ, Cidlowski JA: Molecular mecha-
86. le Roux CW, Chapman GA, Kong WM, et al:
Adrenal hemorrhage in a pediatric burn pa-
nisms of glucocorticoid action and resis-
Free cortisol index is better than serum
tient. Burns 2001; 27:658 – 661
tance. J Steroid Biochem Mol Biol 2002;
total cortisol in determining hypothalamic-
57. Weyrich P, Balletshofer B, Hoeft S, et al:
pituitary-adrenal status in patients under-
Acute adrenocortical insufficiency due to
71. Creed TJ, Probert CS: Review article: Ste-
going surgery. J Clin Endocrinol Metab
heparin-induced thrombocytopenia with
roid resistance in inflammatory bowel dis-
2003; 88:2045–2048
subsequent bilateral haemorrhagic infarc-
ease. Mechanisms and therapeutic strate-
87. Hamrahian AH, Oseni TS, Arafah BM: Mea-
tion of the adrenal glands. Vasa 2001; 30:
gies. Aliment Pharmacol Ther 2007; 25:
surement of serum free cortisol in critically
ill patients. N Engl J Med 2004; 350:
58. Espinosa G, Santos E, Cervera R, et al: Ad-
72. Lewis-Tuffin LJ, Cidlowski JA: The physiol-
renal involvement in the antiphospholipid
ogy of human glucocorticoid receptor beta
88. Vogeser M, Briegel J, Zachoval R: Dialyzable
syndrome: Clinical and immunologic char-
(hGRbeta) and glucocorticoid resistance.
free cortisol after stimulation with Syn-
acteristics of 86 patients. Medicine 2003;
Ann N Y Acad Sci 2006; 1069:1–9
acthen. Clin Biochem 2002; 35:539 –543
73. Xu D, Buehner A, Xu J, et al: A polymorphic
89. Salgado DR, Verdeal JC, Rocco JR: Adrenal
59. Arnason JA, Graziano FM: Adrenal insuffi-
glucocorticoid receptor in a mouse popula-
function testing in patients with septic
ciency in the antiphospholipid antibody
tion may explain inherited altered stress
shock. Crit Care 2006; 10:R149
syndrome. Semin Arthritis Rheum 1995;
response and increased anxiety-type behav-
90. Vogeser M, Mohnle P, Briegel J: Free serum
iors. FASEB J 2006; 20:2414 –2416
cortisol: Quantification applying equilib-
60. Briegel J, Scheelling G, Haller M, et al: A
74. De Iudicibus S, Stocco G, Martelossi S, et al:
rium dialysis or ultrafiltration and an auto-
comparison of the adrenocortical response
Association of BclI polymorphism of the
mated immunoassay system. Clin Chem
during septic shock and after complete re-
glucocorticoid receptor gene locus with re-
Lab Med 2007; 45:521–525
covery. Intensive Care Med 1996; 22:
sponse to glucocorticoids in inflammatory
91. Vogeser M, Briegel J, Jacob K: Determina-
bowel disease. Gut 2007; 56:1319 –1320
tion of serum cortisol by isotope-dilution
61. Meduri GU, Yates CR: Systemic inflamma-
75. Marik PE, Gayowski T, Starzl TE, et al: The
liquid-chromatography electrospray ioniza-
tion-associated glucocorticoid resistance
hepatoadrenal syndrome: A common yet
tion tandem mass spectrometry with online
and outcome of ARDS. Ann N Y Acad Sci
unrecognized clinical condition. Crit Care
extraction. Clin Chem Lab Med 2001; 39:
2004; 1024:24 –53
Med 2005; 33:1254 –1259
62. Ito K, Ito M, Elliott WM, et al: Decreased
76. Murphy JF, Purdue GF, Hunt JL: Acute ad-
92. Cohen J, Ward G, Prins J, et al: Variability of
histone deacetylase activity in chronic ob-
renal insufficiency in the patient with
cortisol assays can confound the diagnosis
structive pulmonary disease. N Engl J Med
burns. J Burn Care Rehabil 1993; 14:
of adrenal insufficiency in the critically ill
2005; 352:1967–1976
population. Intensive Care Med 2006; 32:
63. Hew M, Bhavsar P, Torrego A, et al: Relative
77. Winter W, Kamolz L, Donner A, et al: Hy-
corticosteroid insensitivity of peripheral
drocortisone improved haemodynamics and
93. Rothwell PM, Udwadia ZF, Lawler PG: Cor-
blood mononuclear cells in severe asthma.
fluid requirement in surviving but not non-
tisol response to corticotropin and survival
Am J Respir Crit Care Med 2006; 174:
surviving of severely burned patients. Burns
in septic shock. Lancet 1991; 337:582–583
2003; 29:717–720
94. Bollaert PE, Fieux F, Charpentier C, et al:
64. Chikanza IC, Kozaci DL: Corticosteroid re-
78. De Waele JJ, Hoste EA, Baert D, et al: Rel-
Baseline cortisol levels, cortisol response to
sistance in rheumatoid arthritis: Molecular
ative adrenal insufficiency in patients with
corticotropin, and prognosis in late septic
and cellular perspectives. Rheumatology
severe acute pancreatitis. Intensive Care
shock. Shock 2003; 19:13–15
2004; 43:1337–1345
Med 2007; 33:1754 –1760
95. Annane D, Sebille V, Charpentier C, et al:
65. Chikanza IC, Kozaci D, Chernajovsky Y: The
79. Gloor B, Uhl W, Tcholakov O, et al: Hydro-
Effect of treatment with low doses of hydro-
molecular and cellular basis of corticoste-
cortisone treatment of early SIRS in acute
cortisone and fludrocortisone on mortality
roid resistance. J Endocrinol 2003; 179:
experimental pancreatitis. Dig Dis Sci 2001;
in patients with septic shock. JAMA 2002;
66. Pariante CM, Pearce BD, Pisell TL, et al: The
80. Meyer NJ, Hall JB: Relative adrenal insuffi-
96. Huang CJ, Lin HC: Association between ad-
proinflammatory cytokine, interleukin-
ciency in the ICU: Can we at least make the
renal insufficiency and ventilator weaning.
1alpha, reduces glucocorticoid receptor
diagnosis? Am J Respir Crit Care Med 2006;
Am J Respir Crit Care Med 2006; 173:
translocation and function. Endocrinology
1999; 140:4359 – 4366
81. Marik PE: The adrenal exhaustion syn-
97. Loisa P, Uusaro A, Ruokonen E: A single
67. Liu LY, Sun B, Tian Y, et al: Changes of
drome in patients with liver disease. Inten-
adrenocorticotropic hormone stimulation
pulmonary glucocorticoid receptor and
sive Care Med 2006; 32:275–280
test does not reveal adrenal insufficiency in
phospholipase A2 in sheep with acute lung
82. Van der Voort PHJ, Koopman M: Follow up
septic shock. Anesth Analg 2005; 101:
injury after high dose endotoxin infusion.
corticotropin stimulating tests during ICU
Am Rev Respir Dis 1993; 148:878 – 881
stay. Intensive Care Med 2004; 30(Suppl
98. Bouachour G, Roy PM, Guiraud MP, et al:
68. Kino T, Ichijo T, Chrousos GP: FLASH in-
The repetitive short corticotropin stimula-
teracts with p160 coactivator subtypes and
83. Beishuizen A, Vermes I, Hylkema BS, et al:
tion test in patients with septic shock. Ann
differentially suppresses transcriptional ac-
Relative eosinophilia and functional adrenal
Intern Med 1995; 123:962–963
tivity of steroid hormone receptors. J Ste-
insufficiency in critically ill patients. Letter.
99. Marik PE, Zaloga GP: Adrenal insufficiency
roid Biochem Mol Biol 2004; 92:357–363
Lancet 1999; 353:1675–1676
during septic shock. Crit Care Med 2003;
69. Meduri GU, Muthiah MP, Carratu P, et al:
84. Annane D, Sebille V, Troche G, et al: A
Nuclear factor-kappaB- and glucocorticoid
3-level prognostic classification in septic
100. Chawla K, Kupfer Y, Tessler S: Hydrocorti-
receptor alpha–mediated mechanisms in
shock based on cortisol levels and cortisol
sone reverses refractory septic shock. Crit
the regulation of systemic and pulmonary
response to corticotropin. JAMA 2000; 283:
Care Med 1999; 27(Suppl):A33
inflammation during sepsis and acute respi-
101. Oppert M, Schindler R, Husuang C, et al:
ratory distress syndrome: Evidence for in-
85. Arafah BM: Hypothalamic-pituitary adrenal
Low-dose hydrocortisone improves shock
flammation-induced target tissue resistance
function during critical illness: Limitations
reversal and reduces cytokine levels in early
Crit Care Med 2008 Vol. 36, No. 6
hyperdynamic septic shock. Crit Care Med
111. Meduri GU, Headley S, Golden E, et al:
Stress doses of hydrocortisone in septic
2005; 33:2457–2464
Effect of prolonged methylprednisolone
shock: Beneficial effects on opsonization-
102. Bollaert PE, Charpentier C, Levy B, et al:
therapy in unresolving acute respiratory
dependent neutrophil functions. Intensive
Reversal of late septic shock with supra-
distress syndrome: A randomized controlled
Care Med 2008; 34:344 –349
physiologic doses of hydrocortisone. Crit
trial. JAMA 1998; 280:159 –165
121. Loisa P, Parviainen I, Tenhunen J, et al:
Care Med 1998; 26:645– 650
112. Annane D, Sebille V, Bellissant E: Effect of
Effect of mode of hydrocortisone adminis-
103. Briegel J, Forst H, Haller M, et al: Stress
low doses of corticosteroids in septic shock
tration on glycemic control in patients with
doses of hydrocortisone reverse hyperdy-
patients with or without early acute respi-
septic shock: A prospective randomized
namic septic shock: A prospective, random-
ratory distress syndrome. Crit Care Med
trial. Crit Care 2007; 11:R21
ized, double-blind, single-center study. Crit
122. Weber-Carstens S, Deja M, Bercker S, et al:
Care Med 1999; 27:723–732
113. Leatherman JW, Fluegle WL, David WS, et
Impact of bolus application of low-dose hy-
104. Meduri GU, Golden E, Freire AX, et al:
al: Muscle weakness in mechanically venti-
drocortisone on glycemic control in septic
Methylprednisolone infusion in patients
lated patients with severe asthma. Am J
shock patients. Intensive Care Med 2007;
with early severe ARDS: Results of a ran-
Respir Crit Care Med 1996; 153:1686 –1690
domized trial. Chest 2007; 131:954 –963
114. Meduri GU, Marik PE, Chrousos GP, et al:
123. Egi M, Bellomo R, Stachowski E, et al: Vari-
105. The Acute Respiratory Distress Syndrome
Steroid treatment in ARDS: A critical ap-
ability of blood glucose concentration and
Network: Efficacy and safety of corticoste-
praisal of the ARDS network trial and the
short-term mortality in critically ill pa-
roids for persistent acute respiratory dis-
recent literature. Intensive Care Med 2008;
tients. Anesthesiology 2006; 105:244 –252
tress syndrome. N Engl J Med 2006; 354:
124. Meduri GU, Headley S, Kohler G, et al:
115. Halonen J, Halonen P, Jarvinen O, et al:
Persistent elevation of inflammatory cyto-
106. Sprung CL, Annane D, Keh D, et al: Hydro-
Corticosteroids for the prevention of atrial
kines predicts a poor outcome in ARDS:
cortisone therapy for patients with septic
fibrillation after cardiac surgery: A random-
Plasma IL-1 beta and IL-6 levels are consis-
shock. N Engl J Med 2008; 358:111–124
ized controlled trial. JAMA 2007; 14:
tent and efficient predictors of outcome
107. Annane D, Briegel J, Keh D, et al: Clinical
over time. Chest 1995; 107:1062–1073
equipoise remains for issues of adrenocor-
116. Keh D, Sprung CL: Use of corticosteroid
125. Kellum JA, Kong L, Fink MP, et al: Under-
ticotropic hormone administration, cortisol
therapy in patients with sepsis and septic
testing, and therapeutic use of hydrocorti-
shock: An evidence-based review. Crit Care
standing the inflammatory cytokine re-
sone. Crit Care Med 2003; 31:2250 –2251
Med 2004; 32:S527–S533
sponse in pneumonia and sepsis: Results of
108. Annane D, Vignon P, Renault A, et al: Nor-
117. Annane D, Bellissant E, Bollaert PE, et al:
the Genetic and Inflammatory Markers of
epinephrine plus dobutamine versus epi-
Corticosteroids for severe sepsis and septic
Sepsis (GenIMS) Study. Arch Intern Med
nephrine alone for management of septic
shock: A systematic review and meta-
2007; 167:1655–1663
shock: A randomised trial. Lancet 2007;
analysis. BMJ 2004; 329:480 – 489
126. Lekkou A, Karakantza M, Mouzaki A, et al:
118. Minneci PC, Deans KJ, Banks SM, et al:
109. Russell JA, Walley KR, Singer J, et al: Vaso-
Meta-analysis: The effect of steroids on sur-
HLA-DR expression as predictors of out-
pressin versus norepinephrine infusion in
vival and shock during sepsis depends on
come for patients with community-ac-
patients with septic shock. N Engl J Med
the dose. Ann Intern Med 2004; 141:47–56
quired severe infections. Clin Diagn Lab
2008; 358:877– 887
119. Keh D, Boehnke T, Weber-Cartens S, et al:
Immunol 2004; 11:161–167
110. Schelling G, Stoll C, Kapfhammer HP, et al:
Immunologic and hemodynamic effects of
127. Yende S, Knong L, Weussfeld J: Inflamma-
The effect of stress doses of hydrocortisone
"low-dose" hydrocortisone in septic shock:
tory markers prior to hospital discharge
during septic shock on posttraumatic stress
A double-blind, randomized, placebo-
predict subsequent mortality after commu-
disorder and health-related quality of life in
controlled, crossover study. Am J Respir
nity acquired pneumonia: Proceedings of
survivors. Crit Care Med 1999; 27:
Crit Care Med 2003; 167:512–520
the American Thoracic Society. Am J Respir
120. Kaufmann I, Briegel J, Schliephake F, et al:
Crit Care Med 2006; 3:A836
Crit Care Med 2008 Vol. 36, No. 6
Appendix 1. Modified Grades of Recommendation Assessment, Development, and Evaluation (GRADE) system for Grading the strength of the evidence (15)
Grade of recommendation/
Benefits vs. Risk and burdens
Methodological quality of
supporting evidence
1A: Strong recommendation,
Benefits clearly outweigh risk
RCTs without important limitations
Strong recommendation can
high quality evidence
and burdens or vise versa
or overwhelming evidence from
apply to most patients in most
observational studies
1B: Strong recommendation,
Benefits clearly outweigh risk
RCTs with important limitations or
Strong recommendation can
moderate quality evidence
and burdens or vise versa
exceptionally strong evidence
apply to most patients in most
from observational studies
1C: Strong recommendation,
Benefits clearly outweigh risk
Observational studies or case series
Strong recommendation but may
low quality or very low-
and burdens or vise versa
change when higher quality
evidence becomes available
2A: Weak recommendation,
Benefits closely balanced with
RCTs without important limitations
Weak recommendation, best
high quality evidence
or overwhelming evidence from
action may differ depending on
observational studies
circumstances or patients orsocietal values
2B: Weak recommendation,
Benefits closely balanced with
RCTs with important limitations or
Weak recommendation, best
moderate quality evidence
exceptionally strong evidence
action may differ depending on
from observational studies
circumstances or patients orsocietal values
2C: Weak recommendation,
Uncertainty in the estimates of
Observational studies or case series
Very weak recommendations;
low quality or very low
benefits, risks, and burdens;
other alternatives may be
benefits risk and burden
equally reasonable
may be closely balanced
Reproduced with permission from Chest. RCT, randomized controlled trial.
Crit Care Med 2008 Vol. 36, No. 6
Source: http://www.mecriticalcare.net/downloads/guidelines/coricosteroidinsufficiencyadult.pdf
Pruefungsfragen_maerz_2015_heilpraktiker
Zentrum für Naturheilkunde und Homöopathie Ulrich Kinder e. K. , 87435 Kempten, Kronenstr. 49 88212 Ravensburg, Karlstraße 10, 89073 Ulm, Neue Straße 40 Unser nächster Prüfungsvorbereitungskurs beginnt im Juli 2015 Nähere Informationen über Tel. 0831- 21163 / http://www.znh.de Prüfungsfragen März 2015 – Heilpraktiker Gruppe A
cmemsc.org
The Commonwealth of Massachusetts Executive Office of Health and Human Services Department of Public Health Office of Emergency Medical Services 99 Chauncy Street, 11th Floor Boston, MA 02111 DEVAL L. PATRICK GOVERNOR TIMOTHY P. MURRAY FAX: 617-753-7320 LIEUTENANT GOVERNOR JUDYANN BIGBY, MD SECRETARY