Jokstad.no


Applying color theory
in clinical practice to
Science Manager, FDI World Dental Federation
Professor, University of Oslo, Norway
Learning objectives
Be familiar with the physical mechanisms of
tooth coloring and its measurement
Recognize possible etiology for discolorationRealize the potentials and limitations of
esthetic restorative materials
Be acquainted with different shade guides
and their characteristics
Know of commercially available digital
systems for shade matching
Know procedures for optimizing correct
shade matching & communication
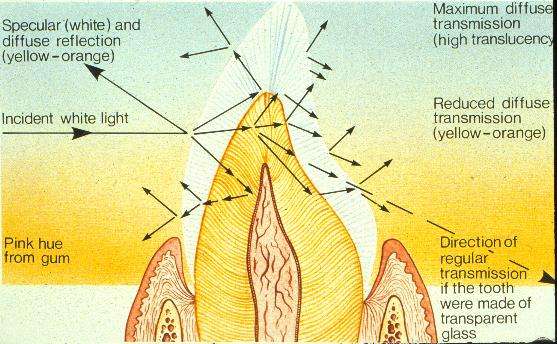
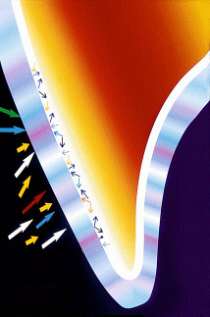
Light- tooth interaction

Colors for teeth and dental materials are reported in the literature as:
• Munsell values (Hue, Chroma, Value)
• Tristimulus values X, Y, Z
• CIE chromaticity values Y(%), x, y
• CIE L*a*b
CIE L*a*b color system
L=100, White
L=0, Black
E*= Change of L*a*b values
Proportional contributors to tooth color
• The proportional contribution of
enamel, dentin, pulp, gingiva and mucosa to the spectral reflection from the tooth in isolation remain uncertain
Proportional contributors to tooth color
• The proportional contribution of enamel,
dentin, pulp, gingiva and mucosa to the spectral reflection from the tooth in
isolation remain uncertain
• In general, dentin
E*= 8(1 – 15)
contributes the most as it is more chromatic than enamel
Proportional contributors to tooth color
• The proportional contribution of enamel,
dentin, pulp, gingiva and mucosa to the spectral reflection from the tooth in
isolation remain uncertain
• In general, dentin contributes the most as
it is more chromatic than enamel
• Enamel is very translucent
and more grey-blue than
Learning objectives
1. Be familiar with the physical mechanisms of
tooth coloring and its measurement
2. Recognize possible etiology for
discoloration and best treatment
• Extrinsic• Intrinsic
Extrinsic discolored teeth – etiology
N1-type colored material (chromogen) binds to the tooth surface. The color of the chromogen is similar to that of dental stains caused by tea, coffee, wine, chromogenic bacteria, and metals.
Extrinsic discolored teeth – etiology
N1-type colored material (chromogen) binds to the tooth surface. The color of the chromogen is similar to that of dental stains caused by tea,coffee, wine, chromogenic
bacteria, and metals.
N2-type colored material changes color after binding to the tooth. The stains actually are N1-type food stains that darken with time.
Extrinsic discolored teeth – etiology
N1-type colored material (chromogen) binds to the tooth surface. The color of the chromogen is similar to that of dental stains caused by tea, coffee, wine, chromogenic bacteria, and metals. N2-type colored material changes color after binding to the tooth. The stains actually are N1-type food stains that darken with time.
N3-type colorless material or prechromogen binds to the tooth and undergoes a chemical reaction to cause a stain. N3-type stains are caused by carbohydrate-rich foods (eg, apples, potatoes), stannous fluoride, and chlorhexidine.
Discolored teeth – best treatments
Active agent
AirScaling / Brushing with
(whitening) toothpaste +Patient counseling
Heriditary defects
Restorative treatment
Tetracycline staining
Custom bleaching trays worn by
10 % carbamide peroxide
patient daily for six to 12 weeks
Single or multiple discolored
External bleaching—in-office one
30 - 38 % H- peroxide, alone
or with heat or light
Multiple teeth and entire
Custom bleaching trays worn by
10 % carbamide peroxide
arches, most effective for
patient daily for two to six weeks
yellow or brown discoloration
Isolated brown or white
Microabrasion followed by neutral
Abrasives + HCl up to 36 %
discolorations of shallow
White discoloration on
Microabrasion followed by custom
Abrasives and acid; 10 %
carbamide peroxide
Endodontically treated teeth
Internal bleaching—in-office or
Na perborate or 35 % H
Intrinsic discolored teeth – etiology
1. Hereditary defects
Dentinogenesis imperfecta.
•
Teeth relatively normal at eruption
Discolor increases with time
More and more translucent, pink yellow, brownish or grey-brown
Enamel may chip off with subsequent heavy dentin discoloration
Intrinsic discolored teeth - etiology
1. Hereditary defects
Dentinogenesis imperfecta. Normal at eruption.
Translucent, yellow, pink, brownish or grey-brown. The enamel may chip off with subsequent heavy discoloration of dentin
Amelogenesis imperfecta. 2 categories:1. Hypoplastic:Teeth smooth and glossyColor is orange, reddish or brown2. Hypomineralised:Color can vary between bone white,
yellow, red and black
The enamel may chip off later
Intrinsic discolored teeth - etiology
2. Toxic effects during tooth development
Fluorosis: Surface may range between small
opaque white spots to extensive yellow-brown bands and/or areas
Intrinsic discolored teeth - etiology
2. Toxic effects during tooth development
Fluorosis: The surface may range between small opaque white spots to
extensive yellow-brown areas
Tetracycline:Chemical complex to ameloenamel proteinsColor can vary between light to dark yellowCharacteristic fluorescence in UV lightCervically usually darker due to thin enamel
Intrinsic discolored teeth - etiology
Amelogenesis imperfecta
2.Toxic effects during tooth development: Fluorosis -
following a trauma, due to internal bleedingin the pulp, with retention of porphyrines andiron in the dentin.The discoloration may bereversible or remain, even if the pulparemains vital
4.Pulp necrosis: Results usually in a tooth
discoloration, but not always
Intrinsic discolored teeth - etiology
1. Hereditary: Dentinogenesis & Amelogenesis imperfecta
2. During tooth development: Fluorosis - Tetracycline
3. Trauma: Internal bleeding in the pulp, with retention of
porphyrines and iron in the dentine
4. Pulp necrosis: Usually tooth discoloration, but not always 5. Other reasons:Degradation products from metallic restorativesSeldom bleeders' diseasesSurface erosions Unknown reasons, possibly related to some
childhood illness. E.g. hepatitis over a p
Discolored teeth – best treatments
Active agent
AirScaling / Brushing with
(whitening) toothpaste +Patient counseling
Heriditary defects
Restorative treatment
Tetracycline staining
Custom bleaching trays worn by
10 % carbamide peroxide
patient daily for six to 12 weeks
Single or multiple discolored
External bleaching—in-office one
30 - 38 % H- peroxide, alone
or with heat or light
Multiple teeth and entire
Custom bleaching trays worn by
10 % carbamide peroxide
arches, most effective for
patient daily for two to six weeks
yellow or brown discoloration
Isolated brown or white
Microabrasion followed by neutral
Abrasives + HCl up to 36 %
discolorations of shallow
White discoloration on
Microabrasion followed by custom
Abrasives and acid; 10 %
carbamide peroxide
Endodontically treated teeth
Internal bleaching—in-office or
Na perborate or 35 % H
Learning objectives
1. Be familiar with the
physical mechanisms of tooth coloring and its measurement
2. Recognize possible
etiology for discoloration and best treatment
3. Realize the potentials
and limitations of esthetic restorative
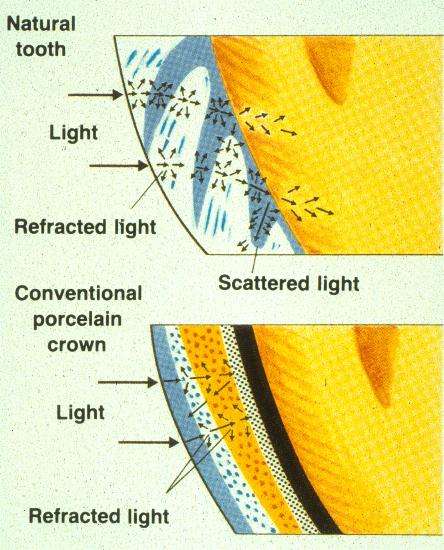
Presently, there are no
spectrophotometric quality control of materials with minimum criteria of performance
Among the direct materials,
composite resins possess the best optical-physical properties regarding
Technique in 1980
New products in 2004
Dental Materials- composites, clinical observations
• Most materials become more
opaque and lighter after a while intraorally, due to water uptake
– This varies markedly among
different materials
Dental Materials- composites, clinical observations
Most materials become more opaque and lighter after a while intraorally, due to water uptake
• Chemically polymerised composites
discolor more into yellow than thelight
polymerisation chemicals in the resin
Dental Materials- composites, clinical observations
Most materials become more opaque and lighter after a while intraorally, due to water uptake
more into yellow than the light polymerised dueto the polymerisation chemicals in the resin
• Chemically polymerised composites
with microfillers discolor more compared to those with macrofillers.
Composites are tested in laboratory for discoloration potential. E.g.
1. Color Stability, in
2. Color Stability,
3. Stain Resistance,
in 37/80°C Coffee
4. Stain Resistance,
An absolute requirement is adequate preparation depth!
The thickness of a restoration / veneer is critical to obtain a correct reflection spectrum and thus acceptable shade
Not removing enough tooth substance will either result in poor esthetics or to overcontouring with risk for subsequent gingival recession. This is especially critical cervically.
Learning objectives
1. Be familiar with the physical mechanisms of
tooth coloring and its measurement
2. Recognize possible etiology for discoloration
and best treatment
3. Realize the potentials and limitations of
esthetic restorative materials
4. Be acquainted with different
shade guides and their characteristics
Composite / Hybrid
VITA/ Biodent / Own
Composite / Hybrid
Composite / GIC / Hybrid / Ceram /
Biodent/ VITA/ Own
Composite / Hybrid / GIC
Biodent / VITA
Hybrid / GIC / Ceram
Composite / Hybrid / Prefab teeth
Composite / Ceram
VITA / Vintage Halo
Ceram / Prefabricated teeth
VITA VITA3D
Composite / Ceram
• Large deviations between
supposedly similar tooth shades from the same producer is not uncommon
Large deviations between supposedly similar tooth shades from the same producer is not uncommon
• Custom-made color shades using the
actual restorative material is claimed to be better than using a standard color shade
Large deviations between supposedly similar tooth shades from the same producer is not uncommon
Custom-made color shades using the actual restorative material is claimed to be better than using a standard color shade
• Some tooth shades changes
following immersion in disinfectants. Keep away from chlorine-containing solutions!
The 5 most common shade guides in use internationally
Bioform -> Biotone ->Trubyte Bioblend -> Portrait IPN
Brown- Brown
1990; Vivadent -> Kerascop
Changed in the mid-seventies
A3.5 & D4 added in 1980
B1 & D1 sometimes excluded
―VITA-Shade‖ guides from different
producers may often differ markedly from the original
Reddish- 43
‖old‖ VITA shades
Learning objectives
Be familiar with the physical mechanisms of tooth coloring and its measurement
Recognize possible etiology for discoloration and best treatment
Realize the potentials and limitations of esthetic restorative materials
Be acquainted with different shade guides and their characteristics
5. Know of commercially available
digital systems for shade matching
Digital Shade Matching Systems
A hand held optic
device with dual light source connected through fiber optics to a spectrophotometer
Digital Shade Systems
• Dental Color Analyser
(clearlight.com/ aei)
• Metalor-ikam system
• ShadeVision /ShadeRite
• Spectroshade
• ShadeEye NCC
Digital Shade Systems -Benefits
• Improved communication between
• Can integrate with
– Intra-oral camera– Digital Camera– Image enhancing software– Mouth Simulator– Printer
Learning objectives
Be familiar with the physical mechanisms of tooth coloring and its measurement
Recognize possible etiology for discoloration and best treatment
Realize the potentials and limitations of esthetic restorative materials
Be acquainted with different shade guides and their characteristics
Know of commercially available digital systems for shade matching
6. Know procedures for optimizing
correct shade matching & communication
Fixed Prosthetic Dentistry- shade selection
Before you start…1. Have the patient remove lipstick or bright makeup
2. If patient is wearing bright clothing, drape him or
her with a neutral colored cover, i.e. light blue or light gray
3. Keep a surface with a neutral color nearby
4. Clean the teeth if doubt of extrinsic discoloration
5. Don't recline your patient – keep at eye level
6. Do not wear glasses that changes with light
Fixed Prosthetic Dentistry- shade selection
… right environment1. Do not use direct lights. Lighting
should be in the most natural light possible. Incoming light may be altered if the window in your operatory has a lot of greenery around it
Fixed Prosthetic Dentistry- shade selection
… right environment1.
Do not use direct lights. Lighting should be in the most natural light possible. Incoming light may be altered if the window in your operatory has a lot of greenery around it
2. Compare your shade selection under
varying conditions such as with lip retraction versus lip down and when the patient moves their head in different directions or lighting angles
Fixed Prosthetic Dentistry- shade selection
… right environment1.
Do not use direct lights. Lighting should be in the most natural light possible. Incoming light may be altered by greenery around the window
Compare your shade selection under varying conditions such as with lip retraction versus lip down and when the patient moves their head in different directions or lighting angles
3. Have also your patient press their
tongue against the lingual surface, when doing an anterior tooth restoration
Fluorescent Natural daylight Incandescent
The same teeth look different under different light
Fixed Prosthetic Dentistry -shade selection
. right time1. Select the shade at the beginning of the session
before the tooth becomes dehydrated and your eyes fatigued
2. An impression and the use of rubber dam will
cause lighter teeth. Retraction cord may influence the tooth color both ways. Anaesthetics too?
3. The canines are good for selecting shade as they
have the highest chroma of the dominant color of the teeth
4. Once the tooth is fully prepared, use your guide to
select the shade of the dentin in the tooth's body
1. The first impression is usually the most
accurate in shade selection
2. It is important avoid fatiguing the eyes.
Do not stare for >3-10 secs. Gazing at a neutral color, e.g. blue or grey for approx. 30 seconds will help to cleanse and refocus the eyes
Fixed Prosthetic Dentistry - shade selection
. the process …1.
Place the shade tab parallel to the facial surface of the teeth, not in front or behind
Arrange each tab on the guide so that the incisal edge is facing out or away from the tab holder. Since incisal shading has the greatest influence on value, it is helpful to position the incisal area of the tabs closest to the teeth you are shading. This will also help avoiding color choice being influenced by the hue area of the tab
Always select the value reading first. It may help to squint
Now that the value reading has been taken, use your hue guide to select the color reading
Fixed Prosthetic Dentistry -shade selection
… finalising 1. Make your final shade selection after
comparing your selections with those of a staff member and/or ask the patient's opinion on your choice
2. Make a mental note of morphological details
3. If unable to match, choose a lower chroma
4. Take photo with shade tab if possible
Communicate this to laboratory
Get as detailed as possible with characterization
Every piece of information helps:
– Surface texture– Glaze– Translucency– Wear– Proximal view with
incisal/thickness of enamel
– Any unique color
characterizations of the dentine
Source: http://www.jokstad.no/chinacol.pdf
math.helsinki.fi
Second order logic and set theory Both second order logic and set theory can be used as a foundation for mathematics, that is, as a formal language in which propositions ofmathematics can be expressed and proved. We take it upon ourselvesin this paper to compare the two approaches, second order logic on onehand and set theory on the other hand, evaluating their merits andweaknesses. We argue that we should think of first order set theoryas a very high order logic.
gablofen.com
TRATAMIENTO DE LA ESPASTICIDAD GRAVEGablofen® para ITB TherapySM (Intrathecal Baclofen Therapy—Terapia Intratecal con Baclofen) aprobada por la FDA INFORMACIÓN IMPORTANTE SOBRE RIESGOS ADVERTENCIA: NO DEJE DE TOMAR GABLOFEN DE REPENTE Si deja de administrarse baclofen repentinamente