Gpli.info
Bitoric Lens Design and FittingStephen P. Smith, B.S. Michigan College of Optometry at Ferris State University Abstract
Bitoric contact lenses are a type of gas permeable (GP) contact lens with two different curves. One curve is on the front surface and the other curve is on the back surface. It is best utilized when corneal cylinder is equal to or exceeds 2.50 diopters. The two curves allow the "saddle principle" to provide an alignment fitting relationship in both meridians. Case Report.
A 20-year-old Caucasian female presented to the clinic noting blurry vision from the dispensed soft toric trial lenses. Upon slit lamp examination, excessive rotation of the lenses was noted OU. We utilized the "left add right subtract" (LARS) principle with different soft toric lenses, but vision remained suboptimal with the patient noting a ghosting effect of the target. After discussing the possible options with the patient, we made the decision to order a trial pair of Art Optical® bitoric contact lenses. Despite some initial discomfort, the patient's vision had improved, remained stable, and no rotation was noted during follow-up appointments. Bitoric lenses are a great option for optical correction in patients with the appropriate amount of astigmatism. The lenses can drastically reduce the amount of rotation seen with soft torics to provide stable vision for the patient. It is important to educate a new GP patient on the transition period for adjusting to lens awareness, wearing and disinfecting schedule, and proper insertion and removal techniques. Key Words: astigmatism, bitoric, contact lens, gas permeable GP contact lenses make up 10% of the contact wearing population and bitoric lenses comprise an even smaller percentage of that population, but still they serve an important purpose for a particular patient base with high amounts of astigmatism.1,2 Toric lenses have two powers in the lens, so keeping the lens stable is imperative for clear vision. Some toric lenses accomplish this with prism ballasting inferiorly or truncation in the lens. Bitoric lenses use the "saddle principle" to maintain stability on the eye.1,3 A saddle fit will establish full alignment to the two principle meridians eliminating any corneal cylinder. GP contact lenses have many advantages over soft lenses. They preserve their shape on the cornea, offer better tear exchange, are more durable, are more resistant to deposit build up, and offer crisper vision.1-4 There are three types of toric GP contact lenses that include front torics, back torics, and bitorics. In most cases of high corneal astigmatism, a bitoric lens design should be used. The primary reason for new GP wearers to discontinue the use of their lenses is due to the initial discomfort experienced.2 Case Report
On August 29th 2012, a 20-year-old Caucasian female presented to the eye clinic with a chief complaint of blurry vision OU. This blurry vision had been present shortly after she began wearing the dispensed trial lenses three weeks prior. Her past ocular history was unremarkable. There was family history of glaucoma with her maternal grandmother, diabetes with her mother, cancer with her sister and maternal grandmother, and hypertension with her father, mother, and maternal grandmother. Hypoglycemia was noted in her review of systems. Her current medications included Tri-Sprintec® and Celexa®, and she had no known drug allergies. The lenses in which blur was noted were Vistakon Oasys Toric®, and the contact lens prescription was -5.50 -2.25X020 OD and -5.50 -2.25X170 OS. The base curve radius was 8.6 mm, and the diameter was 14.5 mm. At that appointment on August 9th, 2012 she reported 20/20 vision OU with the lenses, Slit lamp examination revealed a central fit, 1 mm of movement, ten degree temporal rotation of the lens OD, and no rotation OS. The over-refracion was plano. All other health exam elements were unremarkable. In reviewing her initial exam, we also noted her spectacle prescription to be -5.75 -2.75X008 OD and -5.75 -3.00X175 OS. This spectacle prescription gave her visual acuities of 20/25+1 OD and 20/20-2 OS. Upon taking initial visual acuities on August 29th, 2012 with the Vistakon Oasys Toric® lenses in she reported acuities of 20/100 OD, 20/80-2 OS, and 20/60+1 OU with a ghosting effect. Rotation or instability of the lens was suspected, and slit lamp evaluation confirmed that notion with 25 degrees of rotation temporally OD and 15-20 degrees of rotation temporally OS. The lenses were removed and slit lamp examination showed clear corneas and adnexa, no vascularization, no staining, no scarring, and the anterior chamber was clear. We applied the "LARS principle", and selected a CIBA Air Optix® torics lens of the same sphere and cylinder powers to attempt to improve the patient's vision. After allowing time to settle, she still reported suboptimal vision and slit lamp
examination showed unstable axis location. We then educated the patient on her refractive
correction options. We discussed the use of custom soft toric (ex. Art Optical Intelliwave®), GP
(standard or sclera), or trying various brands of soft toric contact lenses. The decision was made
to try standard diameter GP lenses. We then discussed the benefits of bitoric GP lenses such as
crisper, more stable vision and that they would be more economical long-term due to the ease of
maintenance and longer wearing life. We also made her aware that there would be a period
necessary to adapt to the increased lens awareness. Topography was then done and showed
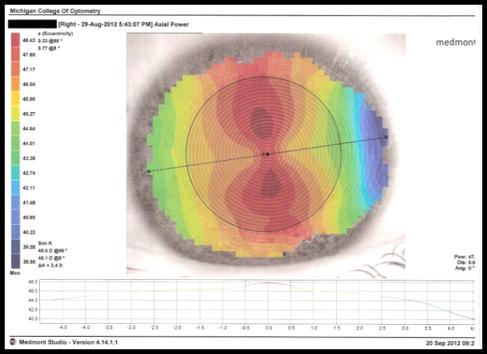
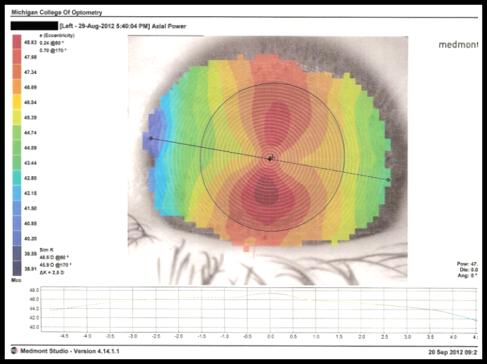
keratomy readings to be 46.1/48.5 @098 OD and 45.9/ 48.5 @080 OS.
Figure 1. Right Eye axial map
Figure 2. Left Eye axial map
depicting limbus-to-limbus With-
depicting limbus-to-limbus With-
the-Rule astigmatism.
the-Rule astigmatism.
The axial topographical map revealed with-the-rule astigmatism and it was calculated
that nearly all of the patient's refractive cylinder was corneal, so we opted for a spherical power
effect fit. This finding along with the amount of cylinder present made her a great candidate for
bitoric GP lenses. We empirically fit these lenses using the Mandell-Moore Bitoric Lens Guide
rather than using a diagnostic set. Using this method, we ordered an Art Optical bitoric of -5.25/-
7.25 BC: 7.37/7.03 OD and -5.25/ -7.50 BC:7.4/7.03 OS. The diameter was 9.5 and the optic
zone was 8.1 OU with Boston EO material. The patient was instructed to return to the clinic to
have the lenses dispensed and evaluated in two weeks.
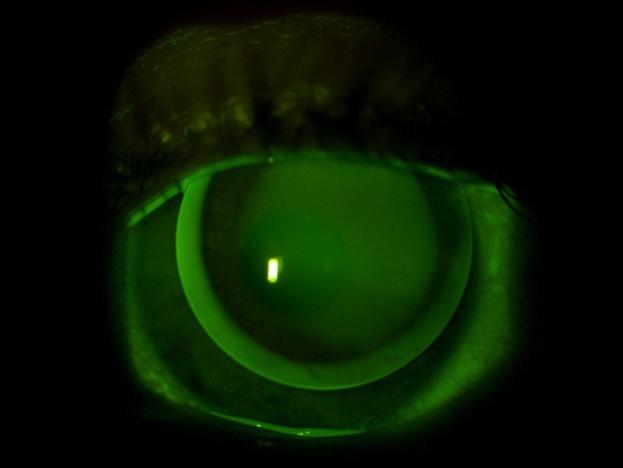
Figure 3. Left Eye slit map photograph using fluorescein to assess the lens-to-cornea
fitting pattern.
The patient returned to the eye clinic September 20th, 2012 to have the ordered bitoric
lenses fit and assessed. The lenses were rinsed, inserted, and allowed to settle. Initial visual
acuities with the lenses were 20/20-2 OD and 20/20-1 OS. The slit lamp exam findings showed
center alignment, movement to be about 1 mm, fluorescein pattern was aligned, good edge lift,
and excellent surface quality. The over-refraction was plano OU. The patient was educated that
the lenses were to be worn daily and disinfected with Clear Care® solution. The GP bitoric
lenses were dispensed, and she was instructed to return to the clinic in 1-2 weeks for a contact
The patient returned October 4th, 2012 after wearing the GP bitoric lenses for two weeks.
The patient noted lens awareness, but that the awareness had gradually decreased while wearing
the lenses 8 hours a day over the two weeks. She also noted a marked improvement in her vision
with the GP bitorics in comparison to her previous soft toric lenses. Her initial visual acuities
were 20/20 OD and 20/15-1 OS at distance, and at near her visual acuities were 20/25-2 OD and
20/15-1 OS. During the slit lamp evaluation, the lenses were noted to be sitting slightly superior
to center. Good movement, edge lift, surface quality, and an aligned fluorescein pattern were also
observed. Further biomicroscopy was done and revealed normal lids, lashes, and cornea. The
patient was made aware the comfort of GP lenses should continue to improve over the coming
weeks and that if the comfort doesn't improve or she notes a decrease in vision to return to the
clinic to assessed for mini scleral or scleral lenses.
Discussion
The objective in fitting a bitoric lens is to achieve a close alignment of the contact lens on
the eye and create an appearance in the fluorescein pattern as if the fit were a spherical lens on a
mildly astigmatic eye. Making the lenses slightly flatter in the vertical meridian will promote
more vertical lens movement and increase tear flow beneath the lens. This will likely provide an
upper lid attached fit, which will be a more comfortable fit. The diameter used for these contact
lenses was determined to ensure complete pupil coverage in both bright and dim conditions.
Most lens designs range from 9.2 to 9.8mm in diameter.1,5 In designing and ordering the patient's
lenses, we used the Mandell-Moore Bitoric Lens guide to input her refraction and keratometry
values. We then determined the base curve by fitting 0.25 diopters flatter than her flat "K"
measurement and 0.50 diopters flatter than her steep "K" measurement, which we obtained via
the Medmont® topographer.1-4
For this patient, we discussed many treatment options. The use of GP toric lenses was
deemed best for initial use in this case. The three GP torics considered were front torics, back
torics, and bitorics. Front torics are useful for patients with spherical corneas and astigmatism.
The spherical correction is on the back of the lens, while the astigmatic correction is on the
front.1,2 Back torics have spherical correction on the front of the lens with the astigmatic
correction on the back. The back toric lens can induce additional astigmatism in the flatter
meridian of the eye, so use of these lenses should be confined to patients who follow the "two-
thirds principle". The "two-thirds principle" is determined by dividing the refractive cylinder at
the cornea by 1.5 and then adding that value to your flat "K" measurement. This will give you an
appropriate steep "K" value.1 Back torics are best utilized in cases of against-the-rule
astigmatism.1,2 Finally, a bitoric lens has a toric anterior surface that compensates for any
residual astigmatism created by the toric posterior surface. There are two type of fits with the
bitoric lenses. There is a spherical power effect fit where the lens acts optically as a spherical
lens because the difference in base curves between the front and back surfaces cancel out any
toricity regardless of the rotation of the lens. There is also a cylinder power effect fit where the
front and back base curves do not completely equal the difference in the lens powers, so rotation
does have an effect on vision. This type of lens design must be prism ballasted to maintain the
proper axis although the saddle principle with these lenses decreases the chance the lens will
rotate.1,2,4,5 Custom soft toric lenses were also an option for this patient, but due the high cost and
possibility of rotation still occurring, this alternative was not used. Scleral and corneoscleral
lenses were discussed as an option for this patient if lens awareness was still noticeable in the
weeks after the follow-up exam. Due to their larger diameter, these lenses rest almost exclusively
on the conjunctiva which is much less sensitive than the cornea. These lenses are also less likely
to become decentered or dislocated.1,6
Bitoric lenses show limited success when the keratometric axis differs 15 degrees or
more from the spectacle cylinder axis.1-3 Spherical GP lenses would be a more practical option of
treatment in these circumstances. Corneal topography that exhibits a symmetric pattern and
astigmatism that is limbus-to-limbus is a good indicator for success in using a bitoric lens
Conclusions
Bitoric lenses are a very viable option for refractive correction in patients with the
suitable amount of astigmatism. The lenses can considerably decrease the amount of rotation
seen with soft torics to provide stable vision for the patient. It is important to inform a new GP
patient on the adjustment period for increased lens awareness, so their expectations of comfort
are appropriate.
References
1. Bennett, Edward, and Vinita Henry. Clinical Manual of Contact Lenses. 3rd ed.
Philadelphia: Lippincott, Williams & Wilkins, 2009. 336-344. Print.
2. Heiting , Gary. "Toric Contact Lenses for Astigmatism." (2011) All about vision, Web.
23 Nov 2012. <http://www.allaboutvision.com/contacts/torics.htm>.
3. Raul Martín Herranz, Guadalupe Rodríguez Zarzuelo and Victoria de Juan Herráez
(2012). Contact Lens Correction of Regular and Irregular Astigmatism, Astigmatism - Optics, Physiology and Management, Dr. Michael Goggin (Ed.), ISBN: 978-953-51-0230-4, InTech, Available from: <http://www.intechopen.com/books/astigmatism-optics-physiology-and-management/contact-lens-correction-ofregular-and-irregular-astigmatism>
4. Silbert, Joel. "Optometric Management." Optometric Management. (2007):
5. Anderson , Bruce. "GP Lens Institute." GP Lens Institute. (2012):
6. Visser , E, R Visser , H Van Lier, et al. "Eye & Contact Lens: Science & Clinical
Practice." Eye & Contact Lens: Science & Clinical Practice. 33.1 (2007): 13-20. <http://journals.lww.com/claojournal/Abstract/2007/01000/Modern_Scleral_Lenses_Part_I Clinical_Features.3.asp>.
Source: http://www.gpli.info/pdf/2013-q3-case-smith-stephen.pdf
A semi-synthetic organism with an expanded genetic alphabet
A semi-synthetic organism with an expandedgenetic alphabet Denis A. Malyshev1, Kirandeep Dhami1, Thomas Lavergne1, Tingjian Chen1, Nan Dai2, Jeremy M. Foster2, Ivan R. Corre & Floyd E. Romesberg1 Organisms are defined by the information encoded in their genomes, suggest that decomposition is mediated by phosphatases. As no degra- and since the origin of life this information has been encoded using a
awmsg.org
All Wales Guide: Pharmacotherapy for Smoking Cessation July 2014 This guidance has been prepared by Rosemary Allgeier, Principal Pharmacist in Public Health, Public Health Wales, with support from the All Wales Prescribing Advisory Group (AWPAG) and the All Wales Therapeutics and Toxicology Centre (AWTTC), and has subsequently been endorsed by the All Wales Medicines Strategy Group (AWMSG). Please direct any queries to AWTTC: All Wales Therapeutics and Toxicology Centre University Hospital Llandough Penlan Road Llandough Vale of Glamorgan CF64 2XX 029 2071 6900 This document should be cited as: All Wales Medicines Strategy Group. All Wales Guide: Pharmacotherapy for Smoking Cessation. July 2014.