Altemuler2.indd
Advances in Cognitive Psychology 2006 • volume 2 • no 2-3 • 207-220 Focal dystonia in musicians: Fromphenomenology to therapy
Hans-Christian Jabusch and Eckart Altenmüller
University of Music and Drama, Institute of Music Physiology and Musicians' Medicine, Hanover, Germany Received 11.01.2005 Accepted 11.10.2006 Keywords
musicians' cramp; focal dystonia, treatment, botulinum-toxin, trihexyphenidyl,
to focal task-specific dystonia with phenotypic
variations including musician's dystonia.
Background: Musician's dystonia is a task-spe-
Treatment: Treatment options for musician's
cific movement disorder which manifests itself
dystonia include pharmacological interventions
as a loss of voluntary motor control in extensively
such as administration of Trihexyphenidyl or
trained movements. In many cases, the disorder
Botulinum Toxin-A as well as retraining pro-
terminates the careers of affected musicians.
grams and ergonomic changes in the instrument.
Approximately 1% of all professional musicians
A long-term follow-up study was performed in
144 patients with musician's dystonia. The out-
Etiology and Pathophysiology: The pathophysi-
come was revealed on average 8.4 years after
ology of the disorder is still unclear. Findings
onset of symptoms. Outcome was assessed by
include (a) reduced inhibition in different levels
patients' subjective rating of cumulative treat-
of the central nervous system, (b) maladaptive
ment response and response to individual thera-
plasticity, e.g. in the somatosensory cortex and
pies. Seventy-seven patients (54%) reported an
in the basal ganglia, and (c) alterations in senso-
alleviation of symptoms: 33% of the patients
rimotor processing. Epidemiological data demon-
with Trihexyphenidyl, 49% with Botulinum Tox-
strated a higher risk for those musicians who
in, 50% with pedagogical retraining, 56% with
play instruments requiring maximal fine-motor
unmonitored technical exercises, and 63% with
skills. For instruments where workload differs
ergonomic changes. In embouchure dystonia,
across hands, focal dystonia appears more often
only 15% of patients reported improvement.
in the more intensely used hand. In psychologi-
The results demonstrate that the situation of musi-
cal studies, musicians with dystonia had more
cians with focal hand dystonia may be significantly
perfectionist tendencies than healthy musicians.
improved. Positive results after retraining and un-
These findings strengthen the assumption that
monitored technical exercises underline the benefit
behavioral factors may be involved in the etiolo-
of an active involvement of patients in the treat-
gy of musician's dystonia. Hereditary factors may
ment process. Only exceptionally, however, can
play a greater role than previously assumed. Pre-
musicians with focal dystonia return to normal mo-
liminary findings suggest a genetic contribution
tor control using the currently available therapies.
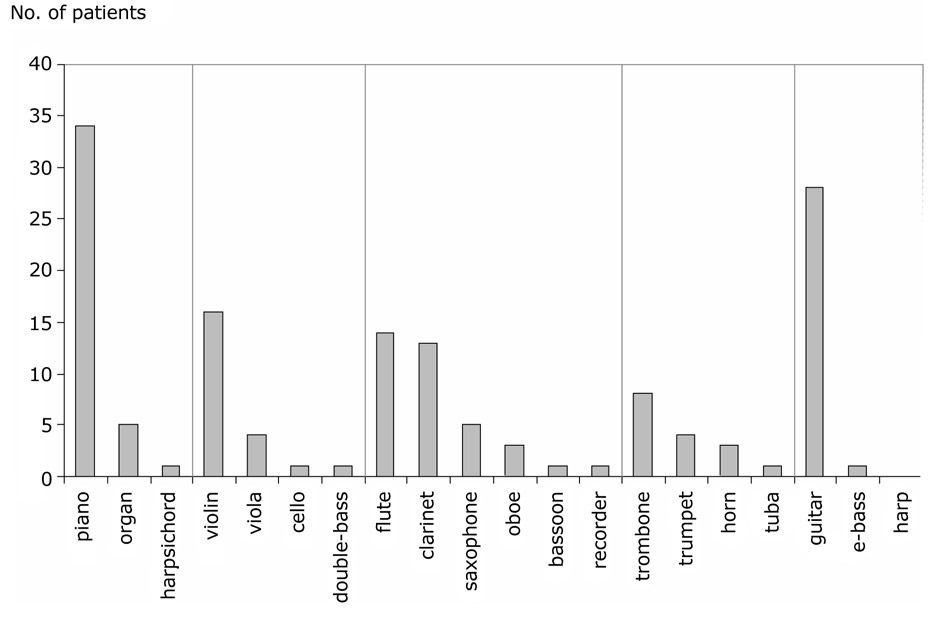
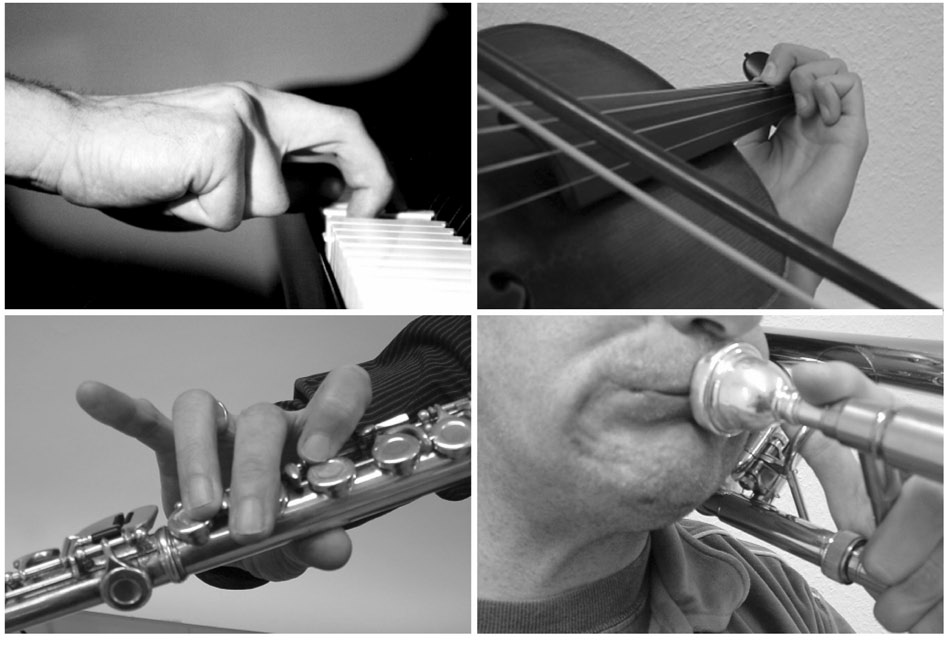
Correspondence concerning this article should be ad-dressed to University of Music and Drama, Institute of Mu- Focal dystonia in musicians, also known as musician's sic Physiology and Musicians' Medicine Hohenzollernstrasse 47, 30161 Hannover, Germany, phone: +49 511 3100552, cramp, is a task-specific movement disorder which fax: +49 511 3100557, e-mail: [email protected], presents itself as a painless muscular incoordina- Hans-Christian Jabusch and Eckart Altenmüller tion or loss of voluntary motor control of extensively talists, 29 patients (20%) were playing plucked instru- trained movements while a musician is playing the ments, 37 patients (26%) were woodwind players and 16 patients (11%) were brass players. The distribution of individual instruments is displayed in Figure 1. In or- ). For those who are affected, focal dystonia is der to compare the distribution of instruments among highly disabling and in many cases terminates mu- dystonic musicians with that in a normal population of sical careers. According to estimates, one percent instrumentalists, the respective numbers of members of all musicians are affected (). In in the German Orchestra Union were used according this article, the phenomenology and epidemiology of to the March-2004 statistics of the German Orchestra musician's dystonia shall be addressed on the basis Union (representing over 90% of German orchestra of data from 144 affected musicians diagnosed and musicians). In our patient group, 20 high string play- followed-up at the Institute of Music Physiology and ers (violin, viola) and 2 low string players (violoncello, Musicians' Medicine of the Hannover University of double-bass) were affected. This ratio was compared Music and Drama. These data will be compared to with the distribution of 3810 high and 1464 low string data from other reports, and discussed with regard to players in the German Orchestra Union. Taking into risk factors for the development of musician's dysto- consideration that one low and 10 high string players nia. Treatment strategies and results will be outlined from our patient group were members of the German based on a retrospective inquiry and self-evaluation Orchestra Union, the comparison of 3800 high and of affected musicians treated with currently available 1463 low string players from the Orchestra Union with the distribution in our patient group revealed an over- All 144 patients were professional musicians diag- representation of high string players among patients nosed with focal dystonia at our outpatient clinic with musician's dystonia (χ2 = 3.83, df = 1, p = .05). between 1994 and 2001. The diagnostic procedure 124 patients were suffering from focal upper limb during their first visit included a complete neurological dystonias (86%), which presented themselves mostly examination as well as visual inspection while patients as hand dystonias in the typical manner with involun- were playing their instruments. None of the patients tary cramping of one or more fingers while patients were suffering from secondary dystonias or other neu- were playing; one trombone player displayed dystonic rological disorders. Data were statistically analyzed movement patterns in his left upper arm. Embouchure using χ2-tests and Fisher's exact tests to identify dis- dystonia was present in 20 patients (14%). Typical proportionate frequencies in the clinical manifestation patterns of dystonic posture are displayed in Figure 2. of subgroups of patients. The level of significance was Details of the localization of focal dystonia in different set at p = .05.
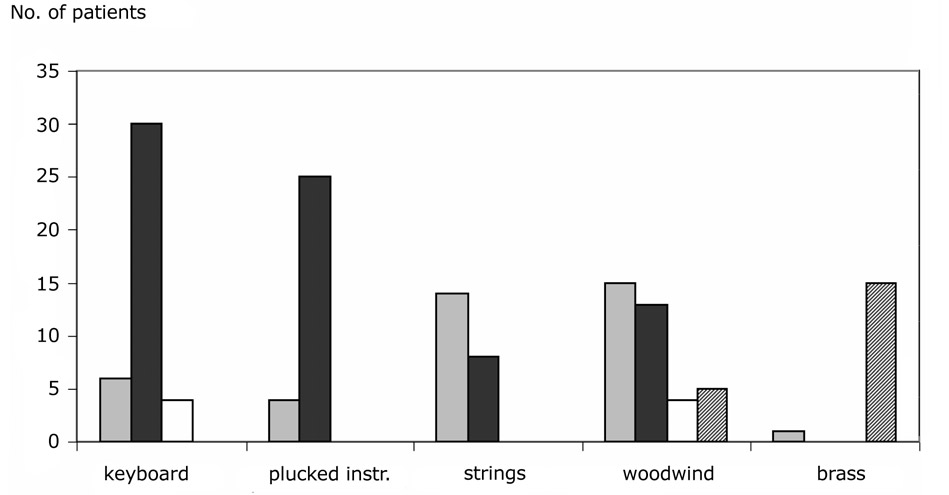
instrument families are given in Figure 3. χ2-tests in 115 patients with unilateral hand dystonia revealed a DEMOGRAPHICS, EPIDEMIOLOGY
different laterality of focal hand dystonia (χ2 = 23.5, df = 3, p < .0001): keyboard musicians and those with plucked instruments were primarily affected The patient group consisted of 116 male (81%) and in the right hand and string players in the left hand 28 female musicians (19%). The mean age at onset of (Bonferroni-corrected follow-up χ2-tests; keyboard vs. symptoms was 33 years (range 17-63 years), the mean string players: χ2 = 13.3, df = 1, p < 0, 01; keyboard duration of dystonic symptoms at the time of the first musicians vs. musicians with plucked instruments: visit was 5.1 years (range 0.1-28 years). At the time of χ2 = 13.6, df = 1, p < 0, 01). No such lateralization the onset of symptoms, 74 patients (51%) had profes- was seen in woodwind players. Bilateral hand dystonia sional positions as soloists and 24 (17%) were tutti was seen only in keyboard instrumentalists (n = 4) players in orchestras, 25 patients (17%) had teaching and in woodwind players (n = 4). Handedness was positions and 21 (15%) were students. Concerning the categorized as right-handed / left-handed / ambidex- genre, 137 patients (95%) were classical musicians, trous according to preferences in the use of hands in 2 patients (1%) were jazz musicians, and 5 patients the activities handwriting, eating with spoon, and cut- (4%) were pop musicians. Nine patients (6%) had a ting with scissors. Among the patients with unilateral history of either writer's cramp or musician's dystonia hand dystonia, there were 108 right-handed patients in their family. The distribution of instrument groups and 5 left-handed patients, 2 patients were ambidex- was as follows: 22 patients (15%) were bowed string trous. Seventy-five right-handed patients had right players, 40 patients (28%) were keyboard instrumen- hand dystonia, and 33 right-handed patients had left
Focal dystonia in musicians: From phenomenology to therapy
Figure 1.
The distribution of instruments in 144 patients with musician's dystonia. Instrument families are separated by vertical lines.
Figure 2.
Typical patterns of dystonic posture in a pianist, a violinist, a flutist and a trombone player.
Hans-Christian Jabusch and Eckart Altenmüller
Figure 3.
Localization of musician's dystonia as distributed in different instrument families.
Grey bars: left hand affected. Black bars: right hand affected. White bars: both hands affected. Hatched bars: embouchure
hand dystonia. This pattern was inverse in left-handed
Since female musicians are predominant in the mu-
patients: in four of these the left hand was affected
sicians' population in Germany, the latter ratio was
(three woodwind players, one guitarist), and in one
corrected to 6:1 Similarly,
pianist the right hand was affected. These propor-
this effect has to be taken into account for the non-
tions were significantly different (Fisher's exact test;
corrected male:female ratio of 4:1 of the present
p < .05).
sample of patients, which additionally underlines the
Ninety-five patients (66%) had dystonic symptoms
increased risk of male musicians to develop focal dys-
only while they were playing the instrument, whereas
tonia. A positive family history of dystonia as seen in
49 patients (34%) had additional difficulties in other
6% of our patient group, has already been described
activities such as writing on the computer keyboard or
as a risk factor for development of musician's dystonia
in everyday activities. Local pain preceded focal dysto-
in other reports
nia in 13 (9%) patients: 7 patients (5%) experienced
local pain only before onset of dystonic symptoms,
The mean age at onset of dystonic symptoms (33
while 6 (4%) patients had pain in the affected region
years) observed in the present study harmonizes with
before and after onset of dystonic symptoms. Twenty-
other studies demonstrating a peak in the fourth dec-
five (17%) patients reported local pain only after onset
of dystonic symptoms, whereas 106 (74%) patients
never experienced pain in the affected region.
Our results demonstrated an association between
the instrument group and the localization of focal dys-
Risk factors for the development of tonia. This is obvious for brass players who are pre-
dominantly suffering from embouchure dystonia. Also in musicians with unilateral hand dystonia an associa-
The demographic data demonstrated a preponderance
tion was observed between the instrument group and
of male musicians in the sample of the present study
the localization of focal dystonia. Keyboard musicians
with a male:female ratio of 4:1. In other reports, the
(piano, organ, harpsichord) and those with plucked
male:female ratio of patients with musician's dysto-
instruments (guitar, e-bass, no harp) were primarily
nia was between 2:1 () and 5:1 (
affected in the right hand. All these instruments are
the patient group of the latter
characterized by a higher workload in the right hand.
report partially overlapped with the present sample).
Additionally, guitar playing requires higher tempo-
Focal dystonia in musicians: From phenomenology to therapy
rospatial precision in the right hand compared to the
moment of the performance. This, as a consequence,
left hand. Bowed string players who have a higher
combines the situation of public performance in classi-
workload and complexity of movements in the left hand
cal music with a high level of social pressure: the gap
were predominantly affected in the left hand. These
between success and failure is minimal in this genre.
observations harmonize with other reports (
Taken together, epidemiological findings indicate
that the amount of workload of the respective body
Moreover, focal hand dys-
part, the complexity of movements and the degree of
tonia in both hands was only seen in those musicians
spatial and temporal sensorimotor precision as well as
with instruments requiring similar movement patterns
the level of social constraints associated with the musi-
in both hands (although with different workload), such
cal performance were related to musician's dystonia.
as woodwind and keyboard instruments. The reported data suggest that musicians with instruments requir-
ing high levels of spatial sensorimotor precision were more often affected by dystonia than were other musi-
The pathophysiology of focal dystonia is still unclear.
cians. Within the string family, musicians who were
Beside of alterations in the basal ganglia circuitry
playing high string instruments (violin, viola) were
more often affected compared to those with low string
dysfunctional plasticity in the sensory thalamus
instruments (violoncello, double-bass). Although the
; ), there is growing evi-
comparison of the distribution of string players in our
dence for the abnormal cortical processing of sensory
patients group with that of the German Orchestra
information as well as degraded representation of mo-
Union might be biased by unreported cases of musi-
tor function in patients with focal dystonia (
cian's dystonia in the union, results suggest that high
string players were overrepresented in our patients
group. High string instruments require a higher spa-
bition was found to be decreased in dystonic patients
tial sensorimotor precision in the left hand compared
to low string instruments due to the shorter length of
In animal studies, repetitive movements
their strings: The strings of a violin, for example, are
induced symptoms of focal hand dystonia and a dis-
approximately three times shorter than the strings of
tortion of the cortical somatosensory representation in
a double-bass (This results
monkeys (suggesting that practice-in-
in a threefold decreased distance between the spots of
duced alterations in cortical processing may play a role
the two tones of a given interval on the fingerboard of
in focal hand dystonia. Recently, behavioral treatment
the violin and in a higher spatial sensorimotor preci-
in patients with focal hand dystonia resulted in clini-
sion required for the left hand in violinists compared to
cal amelioration and in reversed somatosensory map
distortions giving additional evidence for a practice-
Furthermore, in our sample of musicians with uni-
induced cortical map alteration ().
lateral hand dystonia, an association was observed
The importance of practice and the use of the limb in
between the handedness and the side affected by dys-
musician's dystonia was additionally underscored by
tonia. The majority of right-handed patients were af-
the finding of improved symptoms after the immobili-
fected in the right hand and the majority of left-handed
zation of the affected limb in dystonic musicians (
patients were affected in the left hand. Although the
). An impressive finding was reported by
number of left-handed patients was small, this dif-
), who used focal vibratory
ference was significant and indicated that the hand
input to individual hand muscles to produce sensory
with a higher total workload tended to be affected. It
input whilst the excitability of corticospinal outputs to
is noteworthy that there was no string player in the
the vibrated hand and the other hand muscles was
group of left-handed patients. The musical genre of
evaluated with transcranial magnetic stimulation. In
the overwhelming majority of patients was classical
musicians with dystonia, focal vibratory input to hand
music. In contrary to pop or jazz music with impro-
muscles resulted in abnormally suppressed short-la-
vised structures and great freedom of interpretation,
tency intracortical inhibition of all other hand muscles
musical constraints are most severe in classical music.
examined, independent of their functional connectiv-
The latter requires maximal temporal accuracy in the
ity with the vibrated muscles. In healthy non-musi-
range of milliseconds which is scrutinized by the per-
cians, such vibratory input increased short-latency
forming musician as well as by the audience at any
intracortical inhibition of neighbouring muscles. In
Hans-Christian Jabusch and Eckart Altenmüller
healthy musicians, however, vibratory input resulted
This may result in painful overuse syndromes in a
in a suppressed short-latency intracortical inhibition
subgroup of patients.
only of those neighbouring muscles that functionally connected with the vibrated muscles. In patients with
Possible coaction between
writer's cramp, short-latency intracortical inhibition
predisposition and extrinsic and
of neighbouring muscles was unchanged. It was con-
intrinsic factors
cluded that the pathophysiology of musician's dystonia differs from that of writer's cramp. Furthermore, it was
In view of neurophysiological, epidemiological and
hypothesized that long hours of practicing complex
psychological findings in musicians with focal dysto-
movements first produce the modulation of sensorimo-
nia, predisposing factors have been identified such as
tor interaction seen in healthy musicians, and that this
later progresses into the non-focal pattern of short-
as well as a positive family his-
latency intracortical inhibition in musician's dystonia
T he findings of an increased workload and complexity
constitute a particular vulnerability or susceptibility to
of movements as well as increased spatial and temporal
musician's dystonia. Additional extrinsic and intrinsic fac-
sensorimotor requirements being related to musician's
tors may trigger the manifestation of musician's dystonia
dystonia harmonize with the hypothesis of a pathomecha-
on the basis of a given susceptibility. Intrinsic triggering
nism which includes practice-induced alterations. A
factors are physical disorders resulting in local pain and
higher workload in affected musicians might addition-
/ or intensified somatosensory input (trauma, nerve en-
ally be reflected by the observation of a more perfec-
trapment, overuse injury) (;
tionist attitude in dystonic musicians – even before on-
) as well as psychologi-
set of dystonia – compared to other musicians
cal conditions such as perfectionism and anxiety, which
and by the finding of a preponderance of
were found to be related to musician's dystonia (
soloists (51%) in our sample of dystonic musicians. This
. Anxiety has been hypothezised to be an
high rate is in contrast to a rate between 1% and 8% of
aggravating factor during onset of musician's dystonia,
musicians in Germany working as soloists depending on
triggering an emotion-dependent mechanism of motor
the instrument group . A per-
memory consolidation of dystonic movements
fectionist attitude as well as an outstanding professional
position might point at a different and more intense
intracortical disinhibition in musician's dystonia
working behavior resulting in a higher workload in those
might be an acquired, practice-induced phenomenon.
musicians who develop focal dystonia.
Extrinsic triggering factors, according to epidemiological
Local pain and intensified sensory input due to
findings (Tubiana & Chamagne, 2000; Brandfonbrener &
various causes such as nerve entrapment or trauma
Robson, 2002; ), are spatial
or overuse have been described as potential trig-
and temporal sensorimotor constraints as well as mu-
gers of dystonia (
sical and social constraints typical of the performance
situation in classical music. The possible coaction be-
The parallels of abnormal cortical processing of
tween predisposition and intrinsic and extrinsic trigger-
sensory information and cortical reorganization in
ing factors in the manifestation of musician's dystonia is
patients with focal dystonia and those with chronic
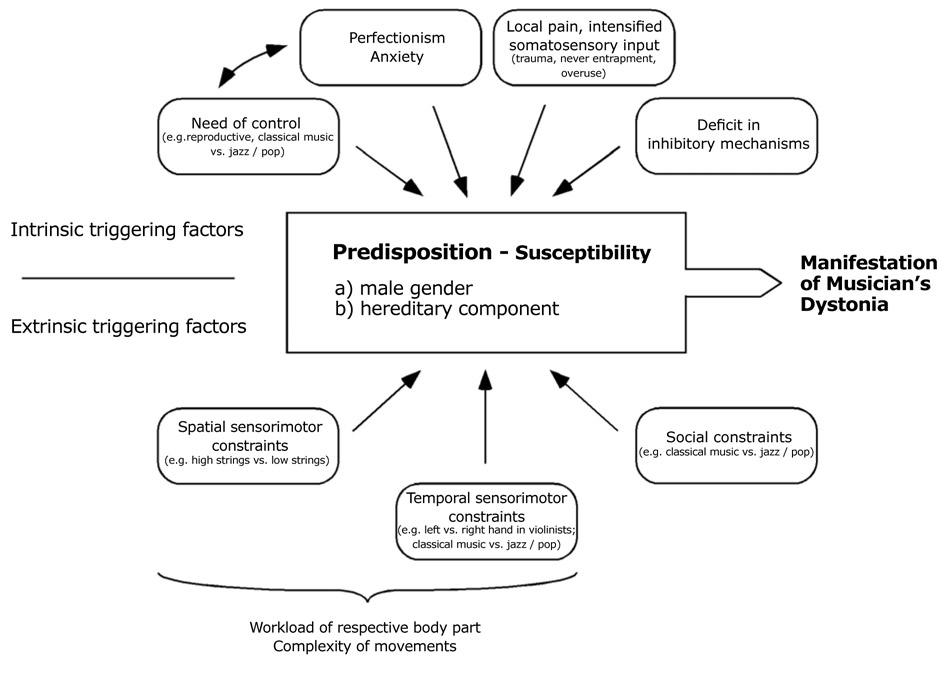
displayed in Figure 4.
pain have already been reported (; . Local
TREATMENT STRATEGIES
pain preceded focal dystonia in 9% of the patients
AND RESULTS
in the present study. In this context, it should be emphasized that local pain is not a typical symp-
For a survey of treatment results, 160 consecu-
tom of focal dystonia. Seventy-four percent of the
tive professional musicians and music students with
patients of our sample never experienced pain in
musician's dystonia were recruited
the affected region. However, as discussed above,
). Treatment strategies included: medication with
pain syndromes may serve as triggers for the de-
Trihexyphenidyl; injection therapy with Botulinum
velopment of dystonia and pain may also occur as a
Toxin; ergonomic changes; pedagogical retraining;
consequence of the persistent attempts by patients
non-specific exercises on the instrument. Outcome
to correct the involuntary movements and postures.
data were assessed using a standardized question-
Focal dystonia in musicians: From phenomenology to therapy
Figure 4.
The possible coaction between predisposition and intrinsic and extrinsic triggering factors in the manifestation of musician's
dystonia. Further explanations are given in the text.
naire which was mailed to patients. Those patients
after the initial visit (range 1-8 years). At the time of
who did not respond were contacted by phone, and
the survey, 77 patients (54%) reported an alleviation of
a standardized interview was conducted using the
symptoms as compared to the time of their first visit,
questionnaire. Patients were asked to estimate 1) the
two of these (1%) reported to be free of symptoms.
cumulative treatment response on a four-step scale
Fifty patients (35%) did not notice any changes and
(free of symptoms – improved – no change – deterio-
16 patients (11%) reported deterioration. Regardless
rated); 2) the treatment response to individual thera-
of treatment, a smaller fraction of patients with
pies (improvement – no effect – deterioration). They
embouchure dystonia showed an improvement (3 of 20
were asked about 3) the nature and duration of thera-
patients; 15 % of these) compared to those with limb
pies not applied by the authors (e.g. exercises on the
dystonia (62 of 123 patients; χ2 = 8.7, df = 1, p < .01).
instrument); 4) their musical activity and professional
A change of profession was reported by 35 patients
situation today. Outcome data of the aforementioned
(29%). A larger fraction of music students changed
144 patients could be obtained. Data were analyzed
their profession (12 of 21 patients, 57%) compared to
using χ2-tests for outcome measures, and multiple
those who were already in their professional careers
regression analyses for predictability of treatment re-
at onset of symptoms (23 of 100 patients; χ2 = 9.84,
sponses. Percentage rates were calculated based on
df = 1, p < .01) ).
the total number of available answers.
Trihexyphenidyl is an anticholinergic medication which
The mean age at the time of the completion of the
is applied orally. Trihexyphenidyl was given to patients
questionnaire was 42 years (range 23-69 years).
with all kinds of musician's cramps when no contraindi-
Outcome was revealed on average 8.4 years after onset
cation was present. Trihexyphenidyl was administered
of dystonic symptoms (range 1-30 years) and 3.4 years
beginning with 1 mg/d, and the dosage was slowly
Hans-Christian Jabusch and Eckart Altenmüller
increased until therapeutic effects were observed.
two fingers vs. non-localized dystonia), type of dysto-
Adjustment of the dosage was made depending on
nia (flexion / extension / embouchure), task specificity
beneficial effects and side effects. Patients with side
at first visit, duration of dystonia were not sufficient
effects and no improvement of symptoms were with-
predictors of the rating of Trihexyphenidyl effects.
drawn from Trihexyphenidyl treatment.
The main predictors of an improvement after treat-
Trihexyphenidyl was applied in 69 patients (48%
ment with Trihexyphenidyl were the localization of
of all patients) with an average maximum dosage of
dystonia in a limb, a high maximum dosage, and a low
11 mg/d (range 1-30 mg/d). Within two months, the
number of concomitant treatments. The low number
medication was interrupted in 20 patients due to side
of concomitant treatments may be a consequence of
effects or unsatisfying treatment response. The other
a successful treatment with Trihexyphenidyl in some
49 patients (34% of all) received Trihexyphenidyl in
patients which limits its value as a predictor variable.
the average for 16 months (range 3-67 months). Most
A high maximum dosage was a sufficient, but not a
frequent side effects were dry mouth (29 patients;
necessary condition for an improvement. One patient
42% of patients receiving Trihexyphenidyl), tiredness
who tolerated a maximum dosage of 30 mg/d had an
(15 patients; 22%), dizziness (13 patients; 19%),
improvement, but in other patients an improvement
agitation (10 patients; 14%), memory impairment
was seen after low dosages. However, there was no
(8 patients; 12%), drowsiness (7 patients; 10%),
patient with high maximum dosages in the group of
depression (7 patients; 10%), loss of concentration
non-responders to Trihexyphenidyl. Taken together,
(5 patients; 7%), nausea (4 patients; 6%), hyperki-
the applicability of Trihexyphenidyl was limited due to
nesia (3 patients; 4%), impaired visual accommoda-
the frequent occurrence of side effects. These were
tion (2 patients; 3%), and tremor (2 patients; 3%).
more often reported by responders than by non-re-
The average minimum dosage at which side effects
sponders although both groups had the same average
occurred was 9 mg/d (range 1-20 mg/d). Due to
maximum dosage. All patients with embouchure dys-
side effects, 16 patients (23%) were withdrawn from
tonias were non-responders. Due to the easy handling,
Trihexyphenidyl. Side effects were not related to age
a treatment attempt with Trihexyphenidyl appears to
or gender. After Trihexyphenidyl, an improvement was
be an option for musicians with limb dystonia when no
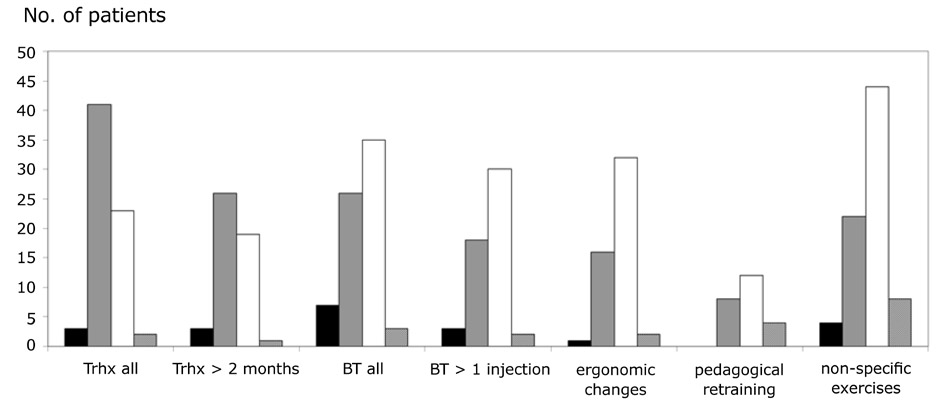
reported by a total of 23 patients (33%) and by 19 pa-
tients with limb dystonia who received Trihexyphenidyl for more than two months (42% of these; average
duration 26 months). Patients' ratings of treatment results are displayed in Figure 5. None of the five pa-
After injection of a small dosage of Botulinum Toxin A
tients with embouchure dystonia had an improvement
(BT) into a muscle, the activity of the injected muscle
after Trihexyphenidyl. Side effects occurred more
is reduced by blocking the release of acetylcholine at
often in patients who reported an improvement after
the neuromuscular junction. This effect persists for a
Trihexyphenidyl (side effects present in 22 out of 23
period of 4 to 6 months. BT injections were recom-
patients) than in patients with no improvement (side
mended only to those patients in which primary dys-
effects present in 32 out of 44 patients: χ2 = 6.66,
tonic movements could be clearly distinguished from
df = 1, p < .01). Trihexyphenidyl average maximum
secondary compensatory movements. A lyophilized
dosage was 11 mg/d (range 4-30 mg/d) in patients
Botulinum Toxin A powder (Dysport®, Ipsen Ltd.,
who had an improvement and 11 mg/d (range
Berkshire, UK) was injected using an EMG-guided
1-20 mg/d) in patients with no improvement. Multiple
regression analysis revealed a model predicting 49%
Target muscles were identified by visual
of the variance of patients' ratings of Trihexyphenidyl
inspection of the dystonic movements while patients
effects (R-square = 0.52; R-square adjusted = 0.49).
were playing their instruments. In patients with flexion
The following variables predicted a positive rating:
or extension dystonia of individual fingers, injections in
limb localization of dystonia (vs. embouchure dysto-
the forearm muscles were preferred. Additional injec-
nia. Beta = 0.59; df = 1; F = 37; p < .001), a high
tions in the hand muscles were performed in patients
maximum dosage of Trihexyphenidyl (Beta = 0.28;
with dystonic flexion in the MCP joints and an exten-
df = 1; F = 6.8; p = .01), a low number of con-
sion component in the PIP and DIP joints.
comitant treatments (Beta = -0.35; df = 1; F = 11;
BT injections were applied in 71 patients (49%),
p < .01). The variables age, gender, localized vs. non-
three of whom had embouchure dystonia. Eighteen
localized dystonia (localized dystonia affecting one or
patients had only one injection due to unsatisfying
Focal dystonia in musicians: From phenomenology to therapy
Figure 5.
Patients' rating of treatment results. Black bars: deterioration of dystonic symptoms. Grey bars: no change of dystonic symp-
toms. White bars: alleviation of dystonic symptoms. Hatched bars: no answer.
Trihexyphenidyl (Trhx): results are given separately for all patients who received Trhx vs. for those who received Trhx for
more than two months.
Botulinum toxin (BT): results are given separately for all patients who received BT vs. for those who received more than one
injection (from Jabusch et al., 2005).
treatment results. Five patients who reported an im-
the affected left hands of one guitarist and two string
provement were not satisfied enough to continue BT
players after injections in the forearm muscles and
treatment. 53 patients (37%) received more than one
hand muscles. None of two patients with injections
injection (average 5.7 injections per patients, range
in the upper arm / shoulder muscles experienced an
2-25) with an average treatment duration of 16 months
improvement and none of three patients with embou-
(range 1-58 months) and an average interval of 4.2
chure dystonia experienced an improvement after BT.
months (range 1-22 months) between treatment ses-
Multiple regression analysis did not reveal any of the
sions. The average dosage per treatment session was
following variables as predictors of outcome after BT:
128 Units (range 9-428). The most injected muscles
gender, age, duration of dystonia, localized vs. non-
were the flexor digitorum superficialis and the flexor
localized dystonia, type of dystonia, target muscles,
digitorum profundus (each: 50 patients; 70% of pa-
mean BT dosage, task specificity at first visit, number
tients treated with BT), followed by the flexor carpi
of concomitant treatments. Positive rating of BT effects
radialis (13 patients; 18%), the flexor pollicis longus,
was correlated to the number of BT treatment sessions
the extensor digitorum and the extensor indicis (7 pa-
(Spearman r = 0.37, p < .01) and the duration of BT
tients for each; 10%), and the interosseus palmaris
treatment (Spearman r = 0.56, p < .01).
(5 patients; 7%). The average dosage per muscle
According to these results, BT treatment was suc-
group was 112 Units (range 88-150) in the upper arm
cessful in those patients in which primary dystonic
and shoulder muscles, 38 Units (range 5-85) in forearm
movements could be clearly distinguished from second-
extensors, 65 Units (range 10-175) in forearm flexors,
ary compensatory movements. This was difficult when
26 Units (range 5-84) in hand muscles. After BT, an
compensatory movements were more pronounced
improvement was reported by 35 patients (49%) and
than primary dystonic movements. EMG-guidance was
by 30 patients who received more than one injection
always applied and seems mandatory since a previ-
(57% of these; average duration 26 months). Of the
ous study has demonstrated that in the absence of
latter group, 21 of 33 patients with injections given
EMG-guidance, only 37% of the needle placements
only in the forearm muscles reported an improve-
reached the desired muscles ). In
ment (64%), and 7 of 13 patients with injections in
our patient group, the best outcome was reported af-
the forearm muscles and hand muscles (54%) had an
ter injections in forearm muscles. Additional injections
improvement: two out of two keyboard players, two of
in hand muscles were useful in patients with a dystonic
four woodwind players, and three of four guitarists with
flexion in the MCP joints and an extension component
the right hand affected. No improvement was seen in
in the PIP and DIP joints. BT injections in hand muscles
Hans-Christian Jabusch and Eckart Altenmüller
appear to be recommendable only in instrumentalists
non-dystonic movements; 4) body awareness tech-
with little lateral finger motion such as in woodwind
niques (e.g. Feldenkrais®) were applied to increase the
players and guitarists (right hand). Keyboard players
patient's perception of non-dystonic movements.
may benefit from this option when they avoid reper-
Pedagogical retraining was applied in 24 patients
toire requiring a wide hand span and extreme lateral
(17% of all), 12 patients (50% of these) experienced
finger motion. BT injections in hand muscles were
improvement. Patients reporting an improvement had
not successful in musicians who needed to perform
undergone this treatment for an average of 28 months
lateral finger movements such as in the left hands of
(range 3-72 months). Two patients with embouchure
one guitarist and of two string players. Musicians with
dystonia took part in pedagogical retraining and re-
embouchure dystonia and such with dystonia affecting
ported no improvement.
the upper arm and shoulder muscles did not benefit
Besides of the reported therapies recommended by
from BT treatment ().
the authors, patients additionally or alternatively per-formed unspecific technical exercises on their instru-
ments which are usually practiced by instrumentalists to improve their technique. 78 patients (54% of all)
Ergonomic changes were recommended whenever ap-
were practicing such unspecific technical exercises, 44
plicable. The aim of ergonomic changes was either a
patients (56% of these) experienced improvement.
blocking of dystonic movements, for example by at-
Six out of 11 patients with embouchure dystonia re-
taching splints to the affected fingers. Alternatively,
ported an improvement after practicing such exercises
circumvention of dystonic movements was achieved
by modifications of the instrument, e.g. the reposition-
These results provide evidence for the benefit of a
ing of individual keys in woodwind instruments or the
behavioral approach, either by pedagogical retrain-
replacement of ring keys by plateau keys
ing or by exercises on the instrument. Pedagogical
). Support systems (belts, stands, tripods) were
retraining was applied in patients with all forms of
recommended when the dystonic hand had to carry the
musician's dystonia, however, only patients with limb
instrument while playing such as in oboe-, clarinet- ,
dystonia improved. More than half of the patients
bassoon players. Ergonomic changes were applied in
who were practicing unspecific exercises reported
51 patients (35% of all), 32 patients (63% of these)
improvement, among them were six out of 11 pa-
experienced improvement and used the ergonomic
tients with embouchure dystonia who were engaged
changes for an average of 35 months (range 3-125
in such exercises. It is noteworthy that the results of
months). Two patients with embouchure dystonia used
these exercises were rated better than that of medical
an ergonomic aid and reported no improvement. As a
therapies. These positive results may be biased by a
conclusion, ergonomic changes should be considered
particular attitude among musicians and the perceived
in all patients with limb dystonia. They are not helpful
self-control through exercises. On the other hand,
in embouchure dystonia (
positive results of retraining and of exercises underline the benefit of an active involvement of patients in the
Pedagogical retraining and
treatment process. At present, the existing behavio-
ral approaches are heterogeneous (Instrument-spe-
Pedagogical retraining was applied in patients with
cific retraining programs ought to be elaborated which
all forms of musician's dystonia. They comprised a
include the aforementioned principles. All approaches
variety of behavioral approaches which were taking
of retraining therapy require time and patience on the
place under the supervision of instructors and included
part of the affected musician, which seem to be limiting
elements based on the following principles reported
factors of these therapies. Behavioral aspects, how-
ever, should be included in all treatment approaches,
): 1) movements of
at least as an adjunct.
affected body parts were limited to a level of tempo and force at which the dystonic movement would not
Findings in the light of the
occur; 2) compensatory movements (e.g. of adjacent
fingers) were avoided, partially under the applicationof splints; 3) instant visual feedback with mirrors or
With regard to the overall outcome, which was re-
monitors helped patients to recognize dystonic and
corded on average 8.4 years after the onset of symp-
Focal dystonia in musicians: From phenomenology to therapy
toms, 71% of patients managed to stay in their musical the zenith of their career have no choice and have to profession. In other studies, focal dystonia had led to undergo treatment in order to improve their situation. the end of the musical career in more than half of the Instrumental students, in contrary, are young and flex-patients (Outcome ible enough to change their profession. In our group, measures were conducted 13.8 (string instrumen-
12 out of 21 affected students changed their profession
talists) () and 8.5 years during the follow-up period. According to our impres-
(woodwind players) (after sion, therapy results do not justify keeping students
the onset of symptoms in these reports. The shorter busy with treatment attempts over years in the most
duration of dystonia might be an explanation for the flexible and productive period of their lives. We con-
better outcome of our patient group compared to the clude that strategies for students with musician's dys-
report on the string players. In the study on woodwind tonia should include early support and encouragement
players, the rate of patients with embouchure dystonia to change to another profession.
was 25% which differs from our group (13.9%). A gen-
erally worse outcome in embouchure dystonia might Limitations
explain the different outcome after similar durations of dystonia in both studies. In another report, 17 out of Besides the reported inclusion / exclusion criteria, the 33 musicians with focal dystonia had stopped playing choice of treatment was strongly influenced by prefer-at the end of the follow-up period ences of patients. Time investment appeared to influ-). Duration of dystonia and total follow-
ence the choice of treatment. Older patients who de-
up time were, however, not mentioned which did not sired a quick improvement preferred BT injections. In allow a direct comparison. This was also the case in a contrast, several patients found the injection therapy report of 145 musicians with an average rehabilitation ‘unnatural' and preferred a retraining therapy. A major time of 24 months, after which 35 musicians returned limitation of the study was the lack of objective as-to playing in public (
sessment tools for musician's dystonia which were not available at the beginning of the follow-up. Recently,
reliable and precise objective methods have been developed for quantification of musician's dystonia
Since psychological conditions such as perfectionism ). and anxiety were found to be related to musician's In future studies, such methods will have to be applied dystonia, psychotherapy has been recommended to be for reliable monitoring of treatment effects. Although included in the treatment (Some we were limited in our assessment to a retrospective patients suffer dramatically from the loss of their abili-
and subjective rating, several considerations support
ties on the instrument and from the whole situation. the validity of our result. Consistent negative results Psychotherapy may be helpful for such patients to reported by patients with embouchure dystonia after find coping strategies and to handle the situation. In
treatment with BT, Trihexyphenidyl and retraining seem
order to improve the preconditions for an effective ap-
to indicate a low placebo-sensitivity of musician's dys-
plication of other therapies, the authors occasionally tonia. Most previous studies observed that a significantrecommended psychotherapy to patients with these number of musicians discontinued treatment within a secondary psychoreactive phenomenons. The direct year if they felt the response did not meet their needs. effects of psychotherapy on the motor coordination of The adherence to treatment seen in our study, with an patients with musician's dystonia, especially in those average treatment duration in responders between two with extreme perfectionism or with anxious traits, have and three years (and up to ten years), seems unlikely not yet been investigated.
that the result did not improve their instrumental per-formance significantly.
The subgroup of instrumental students deserve some additional consideration. Focal dystonia is regarded as
Focal dystonia in musicians is still the main chal-
incurable at present. Although there are some patients lenge in Musicians' Medicine. With the available thera-with encouraging follow-up results, therapy remains pies, the majority of patients manage to stay in their difficult and requires years and sometimes decades of
profession, many of them, however, with substantial
patience, effort and stress. Most patients who are at compromises. Therapy of patients with embouchure
Hans-Christian Jabusch and Eckart Altenmüller
dystonia remains problematic. The available medical A review of approaches are ineffective, and other options have yet
111 musicians with focal dystonia seen at a perform-
to be developed. There is a pressing need for novel
ing artist's clinic 1985-2002. Mov. Disord., 17, 1135
therapies for musician's dystonia. As a new method, A immobilization of affected limbs for four to five weeks
primate genesis model of focal dystonia and repeti-
with a splint was reported (). This
tive strain injury: I. Learning-induced dedifferentia-
treatment resulted in a reduced severity of symp-
tion of the representation of the hand in the primary
toms and improved performance in seven patients
somatosensory cortex in adult monkeys. Neurology,
with musician's cramp and one patient with writer's
47, 508-520
cramp four weeks after removal of the splint, after Treatment effective-24 weeks improvement was still observed in seven
ness for patients with a history of repetitive hand
patients. As another experimental approach, oral
use and focal hand dystonia: a planned, prospective
medication with 5 mg ∆9-Tetrahydrocannabinol (the
follow-up study. J. Hand Ther., 13, 289-301
major psychoactive ingredient of Cannabis sativa L.) in a pianist resulted in significant improvement of the
A constraint-induced movement
pianistic performance for a period of 5 hours
therapy for focal hand dystonia in musicians. Lancet,
. These treatment approaches have to
be investigated in larger numbers of patients in order to confirm beneficial effects. Behavioral therapies and
Sensory motor retun-
interdisciplinary strategies combining pharmacological
ing: a behavioral treatment for focal hand dystonia
and pedagogical methods are promising, but the dif-
of pianists and guitarists. Arch. Phys. Med. Rehabil.,
ferent approaches need to be evaluated. Since phe-
83, 1342-1348.
nomenological and epidemiological data and results from electrophysiological studies and from follow-up
. Effective behavioral treatment of focal
studies imply a behavioral component in the develop-
hand dystonia in musicians alters somatosensory
ment as well as in the treatment of musician's dysto-
cortical organization. Proc. Natl. Acad. Sci. USA, 100,
nia, future research is required to identify ‘beneficial
behavior' on the instrument. This may possibly also be . Functional dystonia in musicians: of help for finding strategies with the particular aim of
rehabilitation. Hand Clin., 19, 309-316.
preventing musician's dystonia.
Ulnar neuropathy and dystonic flexion of the fourth
and fifth digits: clinical correlation in musicians.
A modified version of this review appeared in:
Muscle Nerve, 19, 431-437.
Altenmüller E., Kesselring J., Wiesendanger M., eds. Cole, R. A., Cohen, L. G., Hallett, M. (1991). Treatment Music, Motor Control and the Brain. Oxford University
of musician's cramp with Botulinum Toxin. Med.
Press, 2006.
Probl. Perform. Art., 6, 137-143
Movement-related cortical potentials in writer's
Focal dystonia: advances in
cramp. Ann. Neurol., 38, 862-868
brain imaging and understanding of fine motor con-
trol in musicians. Hand Clin., 19, 523-538
Alteration of digital representations in somatosen-
sory cortex in focal hand dystonia. Neuroreport, 9,
. Abnormal somatosensory homunculus in
dystonia of the hand. Ann. Neurol., 44, 828-831
. The Physics of
. Is there a cure for focal dystonia?
Musical Instruments. New York, Springer.
Experiences with a new retraining therapy for pia-
nists. Proceedings of the German Society for Music
Extensive reorganization of primary somatosensory
Physiology and Performing Arts Medicine, 9, 17
cortex in chronic back pain patients. Neurosci. Lett.,
. Musicians with focal
dystonia: A report of 58 cases seen during a ten-
year period at a performing arts medicine clinic. Med.
ral history of embouchure Dystonia. Mov. Disord.,
Probl. Perform. Art., 10, 121-127
16, 899-906
Focal dystonia in musicians: From phenomenology to therapy
Von der Musikhochschule Musicians' cramp:
zum Arbeitsmarkt (From Music Academy to the Job
Instrumental and gender differences. Med. Probl.
Market). Kraemer RD (ed.) Augsburg, Wissner-
Perform. Art., 18, 21-26
Verlag. pp 71-72
The neurophysiology of dystonia.
. Accuracy of muscle localization without
[Review]. Arch. Neurol., 55, 601-603
EMG: Implications for treatment of limb dystonia.
Neurology, 58, 805-807
Microelectrode studies of normal organization and plasticity of human somatosensory thalamus. J. Clin.
Imaging the pre- and
Neurophysiol., 17, 559-574
postsynaptic side of striatal dopaminergic synapses
in idiopathic cervical dystonia: a SPECT study using
. Inhibitory control of acquired mo-
[123I] epidepride and [123I] beta-CIT. Mov. Disord.,
tor programmes in the human brain. Brain 125, 404-
13, 319-323
. Cerebral activation patterns in
an aggravating factor during onset of focal dys-
patients with writer's cramp: a functional magnetic
tonia in musicians. Med. Probl. Perform. Art., 19,
resonance imaging study. J. Neurol., 248, 10-17
Limb immobilization for the treatment of
sional movement analysis as a promising tool for
focal occupational dystonia. Neurology, 57, 405-409
treatment evaluation of musicians' dystonia. Adv. Neurol., 94, 239-45
. Brain cortical activation during guitar-in-
Anxiety in musicians with focal dystonia and those
duced hand dystonia studied by functional MRI.
with chronic pain. Mov. Disord., 19, 1169-1175
Neuroimage, 12, 257-267
Quantification of focal dystonia in pianists using Scale
Pathophysiological
Analysis. Mov. Disord., 19, 171-180
differences between musician's dystonia and writer's
cramp. Brain doi:10.1093/brain/awh402
∆9-Tetrahydrocannabinol (THC) improves motor control in a patient with musician's dystonia. Mov.
Disord., 19, 990-991
Dominantly transmitted focal dystonia in families of
. Focal dystonia in musicians:
patients with musician's cramp. Neurology, 67, 691-
treatment strategies and long-term outcome in 144
patients. Mov. Disord., 20, 1623-1626
. Focal dystonia in
Dystonia in musicians.
woodwind instrumentalists: long-term outcome.
Semin. Neurol., 9, 131-135
Med. Probl. Perform. Art., 18, 15-20
Long-term outcome
. Long-term botulinum toxin treat-
of focal dystonia in string instrumentalists. Mov.
ment of focal hand dystonia. Neurology, 44, 70–76.
Disord., 19, 43-8
Botulinum toxin treatment of oc-
. Botulinum toxin injections in the treatment
cupational and focal hand dystonia. Mov. Disord., 19
of musician's dystonia. Neurology, 64, 341-343.
Suppl, 8, 116-119.
Focal dystonia in instrumental-
lated electroencephalographic desynchronization in
ists: clinical features. Med. Probl. Perform. Art., 6,
patients with hand cramps: evidence for motor corti-
cal involvement in focal dystonia. Ann. Neurol., 47,
Reorganization in the cuta-
neous core of the human thalamic principal somatic . Prolonged reha-sensory nucleus (Ventral caudal) in patients with
bilitation treatment of musician's focal dystonia. In:
dystonia. J. Neurophysiol., 82, 3204-3212
Tubiana R., Amadio P. C. (eds.) Medical problems of
Hans-Christian Jabusch and Eckart Altenmüller
the instrumentalist musician. London, Martin Dunitz
to pain occur at multiple levels of the human soma-
tosensory system: A somatosensory-evoked poten-
tials study in patients with cervical radicular pain. J.
. Neuroplastic changes related
Neurosci., 20, 9277-9283.
Source: http://embouchure.nl/bestanden/Jabusch_and_AltemullerFD_Advances%20in%20Cognitive%20Psychology.pdf
Microsoft word - hiv report-draft5.doc
HIV Services and QIPP Contents 1. Executive Summary What is ‘QIPP'? HIV Services – the current picture Outcomes – Developing measures that matter Treatment – Developing clinical and cost effective prescribing in the context of choice Care – Developing approaches to meet the needs of people living with HIV
aou.udine.it
UNIVERSITÀ DEGLI STUDI DI UDINE DIPARTIMENTO DI SCIENZE MEDICHE E BIOLOGICHE Corso di Studi in Infermieristica IMPATTO DELLA TERAPIA DIURETICA DOMICILIARE SULLA QUALITÀ DI VITA DEI PAZIENTI CON SCOMPENSO CARDIACO Relatore Laureanda Dott. Stefano Fabris Angelica Moro Anno Accademico 2012 - 2013