Doi:10.1016/s0197-2510(06)70334-5
82 JEMS MARCH 2006

Story by Jay Carter, MSEE, MD, FACEP,
& David Enzman, NREMT-P;
Photos by Bruce Graham, NREMT-P,
Hudson EMS Operations Manager
Extrication of patients from motor vehicle
accidents is usually well covered in EMTcourses, and EMS personnel gain ex-
pertise in this component of rescue operations—many calls, many scenarios, much extricationexperience—early on in their careers. But a crewfrom Hudson (Ohio) EMS (HEMS), with acombined EMS experience totaling more than100 years, responded to a call that presented aunique situation.
The call
The tones dropped for a man injured on a
trampoline and unable to move. The man's
wife had made the call to 9-1-1. The crew
suspected a cervical spine injury from the
start, and they anticipated putting the pa-
tient on a backboard and being off to the
hospital in short order. In their minds, extri-
cating and transferring a patient from a back-
yard trampoline would certainly be easier
than removing someone from an upstairs
bathroom, the bottom of the basement stairs
or a small, subcompact car. Surprisingly, this
was not the case.
On scene, Hudson EMS found a large, back-
yard trampoline, elevated three feet off theground. The patient, an adult male, was lying onit, partially prone. His head was positioned nearthe edge of the canvas, and his feet were near the openhis eyes and respond appropriately to question-ing. He complained of some soreness in his neck.
He denied any headache, change in vision, chestpain, shortness of breath, or abdominal, back orextremity pain. He also denied any numbness ortingling in his extremities. He stated that he hadattempted to do a flip and had been unable tomove since landing.
The physical exam revealed an awake patient
who was oriented x 3. The patient had no obvi-ous head or facial trauma, but complained ofmild tenderness on palpation of the posterior
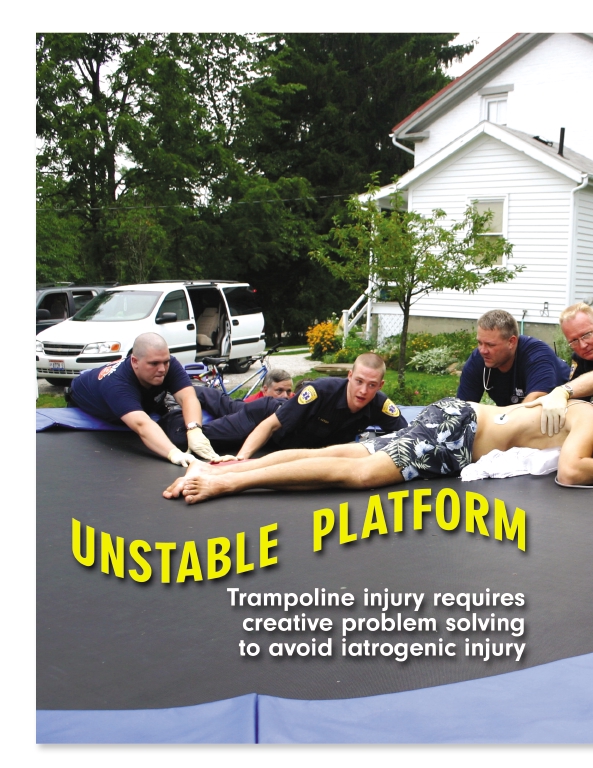
Photo 1: Responding to a backyard trampoline injury, crews work togetheras a team and use innovative methodsto stabilize and prevent further injury tothe patient.
WWW.JEMS.COM MARCH 2006 JEMS 83


Photo 2: Two cribbing towers, air bags and a backboard are placed
and the initial patient assessment completed, the crew's at-
beneath the markedly sagging trampoline canvas to elevate
tention turned to immobilization.
and stabilize the patient prior to further immobilization.
Without anyone on it, a trampoline canvas is normally
taut and level. However, loaded with the weight of an adultmale, the canvas sagged significantly, almost 18 inches froma level plane. Additionally, although the trampoline surfacelooked firm, it wasn't; the canvas had significant spring to it.
Any additional pressure applied caused it to bounce up anddown, much like a water bed's surface.
It was clear that the patient had a significant, unstable cer-
vical spine injury. The providers were concerned that any fur-ther motion could result in respiratory failure or death.
Initially, consistent with standard EMS practices, a back-
board was placed on the trampoline, adjacent to the patientwith the goal being to immobilize him without inflicting anyfurther injury. The board was supported at each end, but thecanvas and the patient sagged well below the level of thebackboard. It looked like a bridge spanning a valley.
The crew considered placing providers on the trampoline,
Photo 3: Post air-bag inflation, the patient is elevated to a non-sagging, horizontal position with the canvas stabilized to minimize motion.
adjacent to the patient's shoulders, hips and legs, to both liftand logroll the patient onto the board—but quickly decided
neck. His chest was non-tender and without any crepitus.
this was impractical. The amount of lifting, coupled with the
He had adequate bilateral breath sounds and no obvious res-
instability and bouncing it would have caused, would have
piratory distress. His abdomen and back were non-tender.
made adequate cervical immobilization impossible.
The extremities were also non-tender and without any obvi-
The EMS incident commander requested the Hudson
Fire Department for assistance with patient extrication.
The crew observed no voluntary motion of the patient's
The EMS and fire incident commanders, brainstorming
hands or feet. Sensation to light touch was intact on the
and soliciting input from others on scene, evaluated sev-
face, but absent from his chest, abdomen, back and ex-
eral options and elected to construct an "elevator" (see
tremities. The crew's clinical impression was of a cervical
Photos 2 and 3, above) to level and stabilize the trampo-
spine injury with resultant quadriplegia. With a safe scene
line and patient. The amount of lifting necessary to bring
84 JEMS MARCH 2006

tient was then logrolled in a slow, controlled manner ontothe backboar
The patient's head was initially found to be anteriorly
positioned with lateral displacement and significant rota-tion. A single, smooth roll and positioning were desirableto regain neutral alignment and minimize the potential forinflicting further, iatrogenic injury. The patient's head wasmanaged by the HEMS medical director, who had re-sponded to the scene, and the patient's shoulders weremanaged by the EMS IC, who optimized the positioningof the patient's head, neck and shoulders.
To avoid hesitation or pause while logrolling the patient,
the medical director cautioned the crews in advance not tostop the logroll mid-procedure for any reason. Althoughthe patient did not experience any pain during the transfer,
the patient to a level position is evident in the pre- and
the providers noted bony crepitation while logrolling and
Photo 4:Logrolling a
positioning him.
Two cribbing towers were placed beneath the patient.
After the patient was positioned on the board, a cervical
traumatic cervical
An inflatable air bag was placed on each tower, and a
collar was carefully applied, followed by head blocks. The
spine injury war-
backboard was placed across the top of the air bags. With
patient's neurologic status was assessed both pre- and post-
one crew stabilizing the patient from above and another
positioning. Fortunately, there was no deterioration in the
crew stabilizing the elevator from below, the bags were
patient's baseline condition, no sudden apnea and no sud-
the infliction of
slowly inflated.
den death. Unfortunately, there was no readily apparent
further injury or
The backboard beneath the trampoline canvas rose gen-
improvement in the patient's quadriplegia. (Photo 5 [p.
tly, lifting the patient's body up to a level, horizontal posi-
88] illustrates the patient post-immobilization and ready
tion. It formed a rigid platform beneath the patient and
helped stabilize the neighboring region of canvas. The pa-
The patient was placed on high-flow oxygen by mask to
86 JEMS MARCH 2006
augment his respiratory status, and two large-bore IVs
Fortunately, no intervention was required. The patient
were started to permit fluid resuscitation should the patient
remained conversant and had no respiratory distress
manifest spinal shock with hypotension and bradycardia. A
throughout the call. After hospital arrival, the patient did
fingerstick glucose level and ECG were obtained to rule
eventually tire and subsequently received a tracheotomy
out hypoglycemia or arrhythmia as possible precipitating
and ventilator support. Following a stormy course, which
factors for the event.
included blood clots in his legs, pneumonia and cardiac
The medical director instructed providers to administer
arrest, he was ultimately weaned off the ventilator.
Phenergan, if needed, to treat nausea experienced by the pa-
Although he remains quadriplegic, he is currently in a
tient during transport. Narcotic analgesics were also consid-
spinal cord rehabilitation unit in Cleveland.
ered, but proved unnecessary. Throughout the call, thepatient's pain was surprisingly minimal.
The crew included several "old-timers" who normally
To fully understand the significance of this case and the ex-
enjoy the challenge of performing invasive procedures, in-
trication and immobilization procedures used, it's impor-
cluding intubation. But not during this call—not on this pa-
tant to review spinal anatomy and discuss this patient's
tient. Each of the seasoned providers later said they were
specific injury. The spine can be viewed as a structural sup-
thinking, "Please keep breathing," throughout the call.
port for the body. It comprises 33 vertebra (seven cervical,
Much like the prospect of field amputations, intubation
12 thoracic, five lumbar, five sacrum and four coccyx). The
of a patient with cervical trauma is a bridge that the in-
vertebral bodies are strong, cylindrical bony structures that
sightful practitioner would prefer never to cross; the risk of
support an individual's weight.
inducing further injury or death is just too high.
Posterior to the vertebral bodies is a bony ring that pro-
Treatment options were mulled over before any ac-
tects the spinal cord it encompasses. The bodies are sepa-
tion was taken so that if an intervention became neces-
rated by disks that serve as shock absorbers for the spine
sary, the plan of action would already be in place and
and increase mobility. The ring has bony prominences that
indecision would not delay treatment. Oral intubation,
extend posteriorly and bilaterally. The posterior promi-
surgical cricothyrotomy and bag-valve-mask ventilation
nences can be felt as bumps down the center of your back.
were all discussed. Paralytics and LMAs were not avail-
They serve as attachment points for muscles.
able for consideration.
A multitude of possible spinal fractures exist, a review of
WWW.JEMS.COM MARCH 2006 JEMS 87

pain and temperature.
The goal of prehospital cervical spine immobilization
is to maintain the head and neck in a neutral position andprevent any motion from inducing or worsening nerveinjury. C-spine protocols are designed to protect the pa-tient with a known or potential neck injury, recognizingthat once injury occurs, it's frequently irreversible andoften devastating.
This patient sustained quadriplegia, which was evident
during the crew's initial assessment. The concern for hisbreathing was due to the fact that the level at which the spinewas injured determines the ability of the patient to breathe.
Breathing encompasses ventilation (i.e., moving air in and
out of the lungs) and respiration (i.e., the exchange of gasesbetween the alveoli and the blood). Ventilation is controlled
which is beyond the scope of this article. Of concern to
subconsciously, with conscious override. You breathe with-
EMS is the fact that some fractures may impinge on the
out thinking about it but you can also take a deep breath or
integrity is ascer-
spinal canal and the spinal cord within. Fractures may be
hold your breath, if you so desire.
tained both prior
unstable, permitting the bones to shift and to compress or
Ventilation is so crucial to life that nature has built in re-
sever the spinal cord.
dundancy, providing two separate neuromuscular mecha-
Severed nerve fibers result in permanent loss of func-
nisms to make sure it happens. Nerve roots branch off the
tion. Compressed nerves may recover but, unfortunately,
spinal cord at cervical levels C3, C4 and C5, forming the
are prone to permanent injury. Damage to a motor nerve
phrenic nerves. The right and left phrenic nerves travel down
will result in paralysis of the muscle innervated by that
to innervate the diaphragm. The muscular diaphragm con-
nerve. In addition to para- or quadriplegia, motor nerve
tracts, pulls downward and draws air into the lungs.
injury can result in respiratory insufficiency, or apnea.
Additionally, the thoracic nerves, which branch off the
Damage to sensory nerves results in the loss of sensation,
spinal cord at thoracic levels T1 through T11, innervate the
88 JEMS MARCH 2006

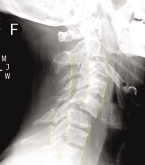
FIGURE 1: In this normal cross table lateral
FIGURE 1: Normal X-ray
FIGURE 2: Patient's X-ray
cervical spine X-ray, the vertebral bodies are
in proper alignment (yellow lines). Opposing
arrows allow you to see the overlying vertebral
bodies (3, 5 and 7) through which an uninjured,
unimpeded spinal cord traverses.
FIGURE 2: This X-ray shows a fracture and an
anterior subluxation (anterior displacement)
on top of C5 on C6, the reason for this
patient's quadriplegia. The spinal canal is
significantly disrupted, thereby compressing
or severing the spinal cord. The alignment of
the vertebral bodies and the lumen of thespinal canal are highlighted by the yellow lines.
chest wall musculature. Muscular contraction increases the
diameter and, hence, the volume of the thoracic cavity, again
recognizable landmarks. The solid vertebral bodies are
drawing air into the lungs. In both cases, muscular relaxation
seen stacked one on top of the next. Yellow lines, super-
leads to exhalation.
imposed on the figure, demonstrate the smooth arc of the
A high cervical spinal injury (above C3) can disrupt neu-
front and back edges of the vertebral bodies.
ral control of both the phrenic and thoracic nerves, leading
The arrows (overlying vertebral bodies 3, 5 and 7) mark
to cessation of respiration (apnea) and death. Injury below
the interior of the spinal canal, through which the spinal
C3 and above T1 leaves the phrenic component of respira-
cord runs, just posterior to the vertebral bodies. On X-rays
tion intact while disrupting the thoracic component. Cord
such as these, the bony structures that make up the spinal
injury below T11 leaves both neural pathways intact, there-
canal are well seen. The soft tissue comprising the spinal cord
by not causing impaired ventilation. Based on the specific in-
itself, however, is not actually seen within the canal. In any
jury location, partial nerve disruption or unilateral
case, you should keep in mind that at the cervical level, the
impairment may also occur.
spinal cord fills the majority of the spinal canal space. The
A normal lateral cervical spine X-ray is depicted in
posterior spinous processes can be imagined to all point to-
WWW.JEMS.COM MARCH 2006 JEMS 89
ward a single focal point.
The white vertebral bodies are again seen stacked
This lateral cervical spine X-ray demonstrates the
one upon another, with the C5 body displaced an-
teriorly. The white posterior spinous processes are
p. 89). He sustained both a fracture and an anterior
also easily seen. The spinal canal is the space be-
subluxation of C5 on C6. Subluxation refers to the
tween them. The severe narrowing of the canal,
anterior displacement, or shift in position, of the C5
which pinches on and either compresses or severs
vertebral body on top of C6.
the spinal cord, is marked with opposing arrows and
The spinal canal is significantly disrupted, there-
can be readily appreciated. The space (lumen/spinal
by compressing or severing the spinal cord. The
canal) remaining for the spinal cord is markedly re-
two anterior yellow lines again demonstrate the
duced, resulting in the catastrophic neurologic in-
alignment of the vertebral bodies, highlighting the
jury seen in this patient.
subluxation. The middle and posterior yellow lines
Of incidental note are the patient's trachea
outline the spinal canal, making the disruption
and epiglottis, both of which are also well visual-
readily apparent. Imagine the spinal canal as a ver-
ized on this image. The trachea appears as a
tically oriented pipe through which the spinal cord
black (air-filled) column anterior to the vertebral
FIGURE 3: The CAT scan demon-
runs. In this case, the pipe is sawed in half, and the
bodies. The epiglottis is marked with a single,
strates marked narrowing of
top section is shifted significantly forward,
the spinal canal, which
markedly narrowing the lumen through which the
The significant narrowing of the spinal canal and
compressed the spinal cord
cord must run.
the resultant compression of the spinal cord seen
at the C5–C6 level (see arrows).
om a CAT (computed
in these images is particularly noteworthy when
The black column of air ante-
axial tomography) scan performed on this pa-
you realize that these images were obtained in
rior to the vertebral bodies is
tient's cervical spine. The CAT scan permits such
the emergency department. This was what it
the trachea. The epiglottis is
soft tissues as the spinal cord to be well visualized.
looked like after the patient's head was carefully
marked with a single red arrow.
This view represents what it would look like if the
positioned and collared by EMS, and after they
The mal-alignment evident is following field repositioning
patient were sliced down the midline, dividing the
had logrolled him onto the backboard for immo-
to a neutral position.
body into right and left halves, and you could
bilization and extrication. Further narrowing may
then view the cut surface.
have been present prior to the positioning and
90 JEMS MARCH 2006
immobilization performed on scene.
the call, a single ambulance and crew seemed reasonable.
Additionally, both the lateral displacement and the rota-
Subsequently, two EMS crews, fire personnel for extrication
tion of the patient's head and neck, evident on the initial
and to manage the helicopter landing zone, and police at
physical exam, were corrected on scene and are not evident
both sites were necessary.
on these views. To follow the pipe analogy, imagine shifting
Creative problem solving and multidisciplinary team
the top section of pipe not only forward but also sideways
work resulted in efficient, optimal prehospital care for this
to envision what this patient's cervical spine looked like
patient. There was a significant potential for iatrogenic in-
prior to prehospital care.
jury or death, which was prevented by the crew's recogni-
The patient's cervical injury was primarily at the C5-C6
tion of the seriousness of the initial injury, innovative
level. The phrenic nerves, originating above the level of the in-
underside cribbing/stabilization and careful handling of
jury, continued to work, innervating his diaphragms. The pa-
the patient by experienced personnel.
tient's spinal cord was disrupted above the level of the
Encountering patients with a potential for cervical spine
thoracic nerves, T1–T11, resulting in paralysis of the chest
injury is a common occurrence in EMS. It's important that
wall musculature, as well as everything else below the injury
crews not become complacent or cavalier in their manage-
level. Chest wall expansion ceased to function, and the patient
ment of these patients. Although many patients may safely
was breathing using only his diaphragm. The loss of his chest
have their cervical spine "cleared" in the field, it's crucial to
wall component of ventilation explains why he eventually
adhere to protocol to minimize the risk of negligently pre-
tired to the point of requiring an invasive, surgical airway.
cipitating, or exacerbating, a devastating injury. JEMS
Jay Carter is an emergency medicine physician and the medical
The EMS incident commander activated air medical trans-
director for Hudson EMS. He has in excess of 30 years' experience
port for this patient as part of his initial scene size-up.
in prehospital care, serving as an EMT, a flight surgeon and a
Smooth, rapid transport to a trauma center well versed in
medical director.
spinal trauma, coupled with the advanced care capabilities
David Enzman is a 30-year EMS veteran with Cleveland EMS,
of the flight physician/nurse team, was appropriate. It's
serving as a chief paramedic and field training officer. Enzman
worth noting the rapid escalation in resources required to
served as EMS incident commander for this incident. He's also the
care for this patient upon making this decision. En route to
acting fire chief of Northfield Center (Ohio) Fire Department.
WWW.JEMS.COM MARCH 2006 JEMS 91
Source: http://www.docjc.us/Tramp/JEMSTrampoline.pdf
Newsletter 20, 26 november 2015
matters in Newsletter No 20, Ngā mihi nui ki a koutou. Greetings to you all. Kia ora, Namaste, Mingalaba, Sua's dei, Talofa Lava, Malo e Lelei, Kia Orana, Bula Term Dates 2016 Tuesday 2 February - Friday 15 April Monday 2 May - Friday 8 July Monday 25 July - Friday 23 September Monday 10 October - Wednesday 14 Ngā mihi nui ki a koutou.
awmsg.org
All Wales Guide: Pharmacotherapy for Smoking Cessation July 2014 This guidance has been prepared by Rosemary Allgeier, Principal Pharmacist in Public Health, Public Health Wales, with support from the All Wales Prescribing Advisory Group (AWPAG) and the All Wales Therapeutics and Toxicology Centre (AWTTC), and has subsequently been endorsed by the All Wales Medicines Strategy Group (AWMSG). Please direct any queries to AWTTC: All Wales Therapeutics and Toxicology Centre University Hospital Llandough Penlan Road Llandough Vale of Glamorgan CF64 2XX 029 2071 6900 This document should be cited as: All Wales Medicines Strategy Group. All Wales Guide: Pharmacotherapy for Smoking Cessation. July 2014.