Microsoft word - structural heart disease workshop - cases
Structural Heart DiseaseWorkshop
Presented by Michael Clark, MD Senior Vice President and Chief Medical Officer Valerie R. Kaufman, MD, FACC, DBIM Vice President and Medical Director Reinsurance Group of America AAIM Annual Meeting 2015 Broadmoor, Colorado Springs, Colorado AAIM 2015: Structural Heart Disease Workshop - 1 - Case 1: Diastolic Dysfunction
73 year old male • 6'0" (183 cm), 245 lbs (111 kg) [266 lbs (121 kg) in APS] Cholesterol 181 mg/dl (4.68 mmol/L) HDL cholesterol 70 mg/dl (1.81 mmol/l), Total Cholesterol/HDL ratio 2.57 Attending physician records • June 1: Periodic assessment. Feels well except for intermittent edema for which he takes furosemide as needed. Medications: amlodipine/atorvastatin (Caduet), chlorthalidone, metoprolol, esomeprazole (Nexium), tadalafil (Cialis), ASA. AAIM 2015: Structural Heart Disease Workshop - 2 - Exercise test with nuclear study February AAIM 2015: Structural Heart Disease Workshop - 3 - Echocardiogram June Left ventricular mass: 340 gm/m2 LV mass index: 135 gm/m2 (nl up to 115 gm/m2) AAIM 2015: Structural Heart Disease Workshop - 4 - Diastolic measurements from June echocardiogram
Applied for insurance August….
Discussion Questions: Diastolic Dysfunction
1. Medications – what do you think of the medical regime? Anything missing? 2. Take note of the pattern of blood pressure response to exercise. What does that 3. A "non-homogenous distribution of radionuclide tracer" is reported. What are they saying here? 4. The echocardiogram report includes a classification of diastolic dysfunction severity. How are each of the diastolic function parameters determined? Which correlate best with increased LVEDP or HFNEF (heart failure with normal ejection fraction)? 5. What are the positive and negative factors of this case related to your mortality AAIM 2015: Structural Heart Disease Workshop - 5 -
Case 2: Hypertrophic Cardiomyopathy
58 year old man, nonsmoker
5'7" (170 cm) tall, 180 lbs (82 kg)
History of hyperlipidemia and cardiomyopathy
Total cholesterol 151 mg/dl (3.9 mmol/L), HDL 76 mg/dl (1.96 mmol/L), ratio 1.99
Medications: ezetimibe/simvastatin combination, enteric-coated aspirin
EKG: Deep T wave inversions in V2-V6
AAIM 2015: Structural Heart Disease Workshop - 6 -
Attending physician records •
Abnormal EKGs date back at least to 2000
Coronary calcium score 2006 (age 49): 276. Exercise stress test negative for ischemia.
Echocardiogram from 2014 showed the following:
Concentric left ventricular hypertrophy with septal and posterior wall thickness of 1.3 cm (normal up to 1.1 cm)
Upper limits of normal left ventricular chamber size (5.7 cm at end diastole)
Dilated left atrium of 4.7 cm (normal up to 4.0 cm)
Normal mitral and aortic valves with mild mitral regurgitation
Compared to 2010 echo, the left atrium is slightly larger (up from 4.4 cm)
Cardiac MRI 2011: apical hypertrophic cardiomyopathy with maximum thickness of 1.9 cm. Mild left atrial enlargement. Moderate myocardial fibrosis involving the inferoapex and apical anterior wall in a non-coronary distribution.
Two week event recorder March 2015, done as routine follow up. 2 episodes of nonsustained ventricular tachycardia, the longest consisting of 9 beats.
Discussion Questions: Hypertrophic Cardiomyopathy
1. What is known about the long-term mortality in hypertrophic cardiomyopathy? 2. Are there markers of higher or lower risk? 3. Is apical hypertrophic cardiomyopathy different from other varieties of
hypertrophic cardiomyopathy?
4. What is the significance of the cardiac MRI findings?
AAIM 2015: Structural Heart Disease Workshop - 7 -
Case 3: Dilated Cardiomyopathy
49 year old male •
6' (183 cm) tall, 235 lbs (107 kg), BMI 31.9
Total cholesterol 151 mg/dl (3.90 mmol/l), HDL 40 mg/dl (1.03 mmol/l),
TC/HDL ratio 3.8 ECG 2012
AAIM 2015: Structural Heart Disease Workshop - 8 -
Echocardiogram 2012
AAIM 2015: Structural Heart Disease Workshop - 9 -
Left ventricular mass: 315 gm Left ventricular mass index: 138 gm/m2 (nl up to 115 gm/m2
AAIM 2015: Structural Heart Disease Workshop - 10 -
Nuclear scan 2012
AAIM 2015: Structural Heart Disease Workshop - 11 -
Cardiac catheterization 2012
AAIM 2015: Structural Heart Disease Workshop - 12 -
Prophylactic internal defibrillator (AICD) placed 2012
AAIM 2015: Structural Heart Disease Workshop - 13 -
AAIM 2015: Structural Heart Disease Workshop - 14 -
Discussion Questions: Dilated Cardiomyopathy
1. ECG – there appears to be some widening of the QRS in the lateral chest leads.
What do you think?
2. Echo 2012 – The left ventricle in diastole is 6.9 cm but "indexed" within the
normal range at 3.1 cm. What do you think? The left ventricle in systole is 5.5 cm. Where have you seen that measurement before?
3. Perfusion scan 2012 – Exercise capacity at 8 minutes! Overall, does this report
change your impression of the case?
4. Cardiac catheterization 2012 – Do we have a final diagnosis and assessment? 5. An AICD (automatic implantable cardiac defibrillator) has been implanted for
prophylaxis. What do the reports reveal and how would that revise your ultimate assessment?
AAIM 2015: Structural Heart Disease Workshop - 15 -
Case 4: Athlete's Heart Syndrome
44 year old man, nonsmoker, assistant basketball coach for major Division 1 program (former player) •
6' (183 cm), 180 lbs (81.8 kg)
Palpitations 4 years ago. Had echocardiogram. No treatment and no recurrence
Lab studies within normal limits
Attending physician records •
Only seen a few times for minor acute issues
Palpitations 4 years ago. Started after a strenuous work out. Felt heart pounding and a little "shaky". EKG showed LBBB, and atrial fibrillation with rapid ventricular response. Converted to sinus rhythm with vagal maneuver. Echocardiogram showed the following:
Normal Range
Left ventricular internal
dimension (diastole) Left atrium
Septal thickness
Posterior wall thickness
Normal mitral and aortic valves. Mild mitral regurgitation. Mild apical hypokinesis with an ejection fraction of 45% Normal tricuspid valve with mild-moderate tricuspid regurgitation. Estimated pulmonary artery systolic pressure is 35. The right atrium and right ventricle appear mildly dilated Conclusion: Mild dilatation of the left atrium and left ventricle with slightly diminished ejection fraction. Correlate clinically.
Advised at the time of the episode to follow up with cardiologist, but has felt relatively well. Has 2 young children, feels like he never gets enough sleep. He travels for his job and is not able to work out regularly, but is very active especially during the season. He has not had any recurrent palpitations.
Primary care physician feels likely athlete's heart, so not really necessary to follow up unless patient wishes.
AAIM 2015: Structural Heart Disease Workshop - 16 -
Discussion Questions: Athlete's Heart Syndrome
1. How is athlete's heart syndrome defined? 2. Are you comfortable that this is likely athlete's heart syndrome? Why or why
3. What is known about the long-term outcome of athlete's heart syndrome? 4. Are there factors in this case of concern? 5. Would you like to have additional information? If so, what? 6. If proposed insured was 6'9" (206 cm) and 250 lbs (114 kg), would you view risk
AAIM 2015: Structural Heart Disease Workshop - 17 -
Case 5: Peri-partum Cardiomyopathy
36 year old female
•
5'4" (163 cm), 142 lbs (64.5 kg)
Family history: Father had an MI at age 40; also had multiple cerebral aneurysms. No family history of cardiomyopathy.
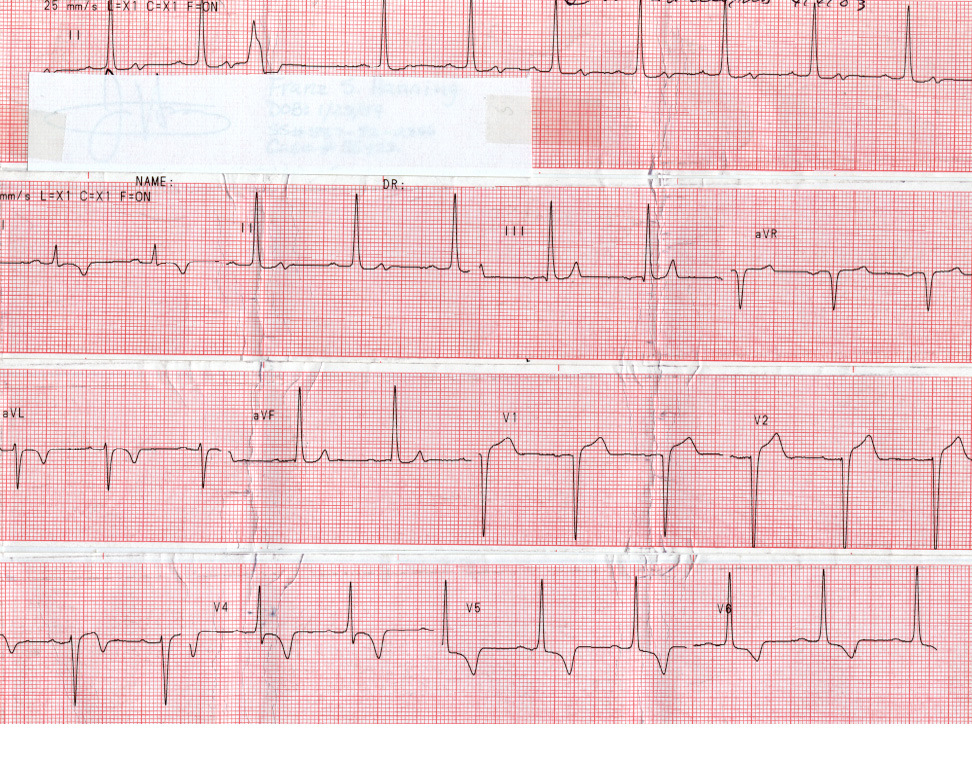
Attending physician records One week post-partum normal delivery of twins noted extreme fatigue, swollen legs, and "could not lie flat without getting short of breath". A run of ventricular tachycardia was noted at the local urgent care center and again in the Emergency Department of the tertiary care hospital on transfer. ECG 7/23
AAIM 2015: Structural Heart Disease Workshop - 18 -
Persantine Thallium 7/24
AAIM 2015: Structural Heart Disease Workshop - 19 -
Holter monitor 7/26: PVCs but no episodes of ventricular tachycardia
Echo 8/26
AAIM 2015: Structural Heart Disease Workshop - 20 -
Echo one year later 7/18
AAIM 2015: Structural Heart Disease Workshop - 21 -
MD letter 3 years later. Current meds: lisinopril, metoprolol, and spironolactone
Discussion Questions: Peri-partum cardiomyopathy
1. What are the risk factors for peri-partum cardiomyopathy? 2. What features of the clinical presentation are associated with an adverse
prognosis? Are there any positive features that might improve your assessment?
3. An AICD (automatic internal cardiac defibrillator) was not implanted in this case.
Would it change your assessment if an AICD was in place and well-monitored?
4. Comparing echo reports from 7/29 and one year later, the impression might be
that there was further deterioration during that time. What do you think of the echo from one year later 7/18?
AAIM 2015: Structural Heart Disease Workshop - 22 -
Case 6: Mitral Regurgitation
62 year old man, nonsmoker
5'9" (175 cm), 212 lbs (96 kg)
BP 146/88, pulse 64
History of HTN, high cholesterol, diabetes
Current medications: valsartan/HCTZ combination, atorvastatin, glipizide
On insurance lab studies
Total cholesterol 176 mg/dl (4.6 mmol/L), HDL 45 mg/dl (1.2 mmol/L), ratio 3.9
Hemoglobin A1c 7.1%
Urinalysis within normal limits
NTproBNP 491 pg/ml
EKG: Normal sinus rhythm, rate 76. Prominent voltage, minor nonspecific ST-T changes diffusely
Attending physician records •
Routine care, regular visits
Long history of a heart murmur, described as Grade 2-3/6 systolic murmur
Abnormal EKG noted 4 years ago. Nuclear stress test done.
Resting heart rate 66, BP 138/84. Resting EKG - nonspecific ST-T changes
Exercised 7 minutes on a Bruce protocol to a peak heart rate of 150 and a BP of 204/96. Stopped due to shortness of breath and fatigue.
With exercise, accentuation of resting ST abnormalities, reaching a maximum of 2 mm of ST depression in the inferior and lateral precordial leads. There were also frequent PVCs throughout the later stages of exercise and early recovery. The EKG returned to baseline at 8 minutes of recovery.
No perfusion defects on the nuclear scan. Left ventricular size appeared normal and ejection fraction was low normal.
Resting echocardiogram (also done 4 years ago):
Normal Range
Left ventricular internal
dimension (diastole) Left atrium
Septal thickness
Posterior wall thickness
Trileaflet, mildly sclerotic but freely mobile aortic valve. Mild mitral annular calcification with thickening of both mitral valve leaflets. No prolapse. Left ventricular ejection fraction 52%. Doppler study: − Mean gradient of 6 mm Hg across aortic valve − Moderately severe (eccentric posterolateral jet) mitral regurgitation − Right ventricular systolic pressure estimated at 36 mm Hg − Evidence of mild diastolic dysfunction Conclusion: Mild left ventricular hypertrophy. Aortic sclerosis. Moderately severe mitral regurgitation.
AAIM 2015: Structural Heart Disease Workshop - 23 -
Discussion Questions: Mitral regurgitation
1. What factors in this case, both clinical and from the echo report, can be used to
help assess the severity of the mitral regurgitation?
2. How do you view the ejection fraction of 52%? Is it normal and favorable? 3. What is the significance of the NTproBNP? 4. Does the severity of mitral regurgitation correlate with mortality risk? 5. Is there likely to be excess mortality associated with the findings in this case?
What about morbidity?
6. What is the likelihood that this person will need surgical intervention? Repair or
replacement? Would it matter from an insurance risk perspective?
7. What is the recommended clinical follow up for mitral regurgitation, and how is
that relevant for insurance risk selection?
AAIM 2015: Structural Heart Disease Workshop - 24 -
Case 7: Ventricular Noncompaction
26 year old male, professional athlete
6' 5" (196 cm), 200 lbs (90.9 kg), BMI 23.7
Total cholesterol 208 mg/dl (5.38 mmol/l). HDL 112 mg/dl (2.9 mmol/l). mm TC/HDL ratio 1.8
AAIM 2015: Structural Heart Disease Workshop - 25 -
Echocardiogram 2012
AAIM 2015: Structural Heart Disease Workshop - 26 -
Echocardiogram 2013
AAIM 2015: Structural Heart Disease Workshop - 27 -
Discussion Questions: Ventricular non-compaction
1. Interesting ECG – how would you best describe the findings? 2. Echo 2012 – do you agree with the assessment of the findings? Ventricular
size? Finding at the ventricular apex?
3. Echo 2012 – no clinical comment or evaluation. If this was all you had, what
4. Echo 2013 – do you agree with the assessment of the findings? Do you think
there has been any significant change? What if the next LVED had been 5.9 cm?
5. If it was 2013, what would you do? 6. Team switch and league rules change – no further studies. It's 2015 – what
do you want to do?
AAIM 2015: Structural Heart Disease Workshop - 28 -
Case 8: Takotsubo Cardiomyopathy
68 year old woman, nonsmoker •
5'5" (165 cm) tall, 166 lbs (75 kg), BMI 28
BP 134/76, pulse 62
Treated for hypertension, chronic anxiety and depression.
History of "broken heart syndrome" 2 years ago. Hospitalized for 6 days. Resolved.
Current medications: losartan 50 mg daily
atorvastatin 10 mg daily
metoprolol 25 mg bid
citalopram 20 mg daily
alprazolam 0.25 mg as needed
Discussion Questions
1. What is "broken heart syndrome"? 2. How is it different from acute coronary syndrome?
Attending physician records
Long history of anxiety and recurrent depression. On a variety of medications over the years. Missed occasional days of work, but no long periods of disability, never hospitalized and no suicide attempts
Two years ago, acute grief reaction in response to sudden death of her husband of 42 years
The day after her husband's death, she presented with chest pain and acute congestive heart failure. Diagnosed with takotsubo cardiomyopathy (broken heart syndrome)
EKG showed ST elevation in inferolateral leads
Troponins elevated; creatine kinase (CK) not elevated
Echocardiogram showed ballooning of the left ventricular apex during systole with an ejection fraction (EF) of 40%
Cardiac cath revealed minor nonobstructive coronary disease
Treated supportively, and was discharged after 6 days
EKG and echo obtained 3 months later both back to baseline (normal). Left ventricular size was normal and EF was 55%
Cardiac follow up 5 months prior to application was also favorable, with no symptoms reported. EKG remains normal.
Discussion Question
1. What is the long-term outlook for takotsubo cardiomyopathy?
AAIM 2015: Structural Heart Disease Workshop - 29 -
Source: http://aaimedicine.org/annualmeetingpresentations/documents/AAIM15-Workshop-StructuralHeartDisease-Cases.pdf
mesotherapie1.free.fr
A.M.M.E. Cahier n° 1 • Bienvenue à l'AMME Corée p 2• Le mot du Président • La mésodissolution • Lumière pulsée Lampe flash • Traitement du vieillissement cutané par produits de comble-ments • L'acide hyaluronique • Le site estheticmeso.com
10-6-00
Electronic Commerce Advisory February 19, 2002 FTC Settles Eli Lilly Prozac Privacy The recently announced settlement between Eli Lilly and Company (Lilly) and the Federal Trade Commission (FTC) demonstrates once again the importance of backing up promises made in corporate privacy policies with acomprehensive corporate program. It also dramatically reconfirms the fact that even an unintentional violation of acompanys posted privacy policy can result in a regulatory enforcement action and damage to brand and reputation.